PIP கூட்டு மாற்று
Patients › Rehabilitation
ஒரு விரலின் அணிந்த நடுத்தர மூட்டு (PIP மூட்டு) க்கான சிலிகான் மாற்றத்திற்குப் பிறகு ஒரு பாதுகாக்கப்பட்ட மீட்புத் திட்டம், அங்கு இயக்கத்தின் துவக்க வேகம் அறுவை சிகிச்சையாளர் விரலின் முன் (கைத்தடி பக்கத்தில்) அல்லது பின்புறத்தில் இருந்து சென்றாரா என்பதைப் பொறுத்தது.
இந்த நெறிமுறை உங்கள் மீட்பு வழிகாட்டுகிறது ஒரு விரலின் நடுத்தர சங்கிலியை மாற்றுதல் இது உங்கள் வீட்டு உடற்பயிற்சி திட்டத்துடன் தொடங்குகிறது, அதைத் தொடர்ந்து உங்கள் கை சிகிச்சையாளருக்காக எழுதப்பட்ட கட்டமைக்கப்பட்ட மருத்துவ நெறிமுறை உள்ளது. உங்கள் மறுவாழ்வு எவ்வாறு முன்னேறுகிறது என்பதைப் பொறுத்து உங்கள் சிகிச்சையாளர் திட்டத்தை சரிசெய்யலாம்.
அறுவை சிகிச்சைக்குப் பிறகு உங்கள் காயத்தைப் பற்றி ஏதேனும் கவலைகள் இருந்தால், அறைகளைத் தொடர்பு கொள்ளுங்கள். காயத்தின் புகைப்படத்தை எடுத்து அதை மதிப்பாய்வு செய்ய மின்னஞ்சல் அனுப்புவது பெரும்பாலும் உதவியாக இருக்கும்.
எதிர்பார்ப்பது என்ன
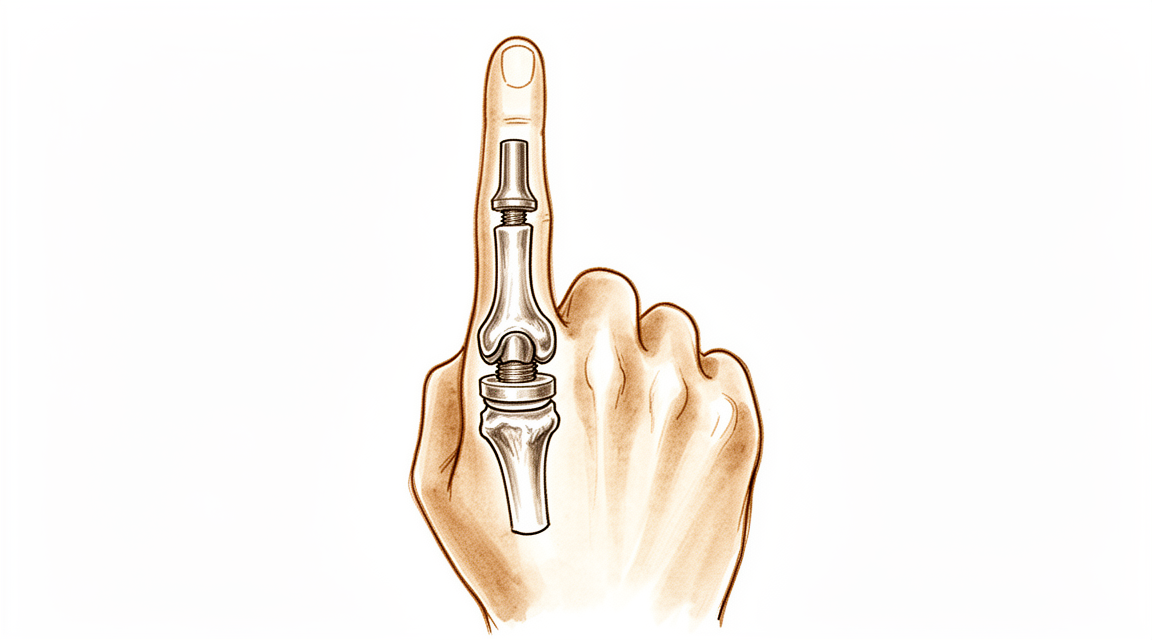
இந்த அறுவை சிகிச்சையின்போது, உங்கள் விரலின் நடுத்தர மூட்டு மூட்டுவலி மற்றும் இறுக்கத்தால் சிதைந்துவிட்டது. நெகிழ்வான சிலிகான் இடைவெளி (ஸ்வான்சன் வகை உள்வைப்பு) இரண்டு எலும்புகளுக்கு இடையில் வைக்கப்படுகிறது. இடைவெளி என்பது ஒரு கடினமான இயந்திர கீல் அல்ல; இது ஒரு வளைந்த இடைவெளி, இது எலும்புகளை ஒதுக்கி வைக்கிறது, விரலை வளைக்க அனுமதிக்கிறது, மேலும் உங்கள் சொந்த வடு திசு அதைச் சுற்றி ஒரு புதிய ஆதரவு சட்டை உருவாக்க அனுமதிக்கிறது. முக்கிய மற்றும் மிகவும் நம்பகமான நன்மை வலி நிவாரணம்நீங்கள் ஒரு பயனுள்ள, மிதமான வளைவு வளைவு (பொதுவாக சுமார் 40 முதல் 60 டிகிரி வரை) பெரும்பாலான மக்கள் மிகவும் திருப்தி அடைகிறார்கள் ஏனென்றால் வலி போய்விட்டது மற்றும் விரல் பயன்படுத்த வசதியாக இருக்கிறது.
உங்கள் மீட்பு பற்றி மிக முக்கியமான விஷயம் எந்த வழியில் அறுவை சிகிச்சை சென்றார், ஏனெனில் அது நீங்கள் எவ்வளவு சீக்கிரம் நகர்த்த முடியும் என்பதை தீர்மானிக்கிறது:
- முன்னால் இருந்து (கைத்தட்டல் பக்கத்தில், ஒரு ஃபோலார் அணுகுமுறை): விரலின் பின்புறத்தில் உள்ள சரிசெய்யும் தசை முற்றிலும் அப்படியே உள்ளது. பின்புறத்தில் எதுவும் குணமடைய வேண்டியதில்லை என்பதால், சில நாட்களுக்குள் விரலை நகர்த்த ஆரம்பிக்கலாம்.
- பின்புறம் இருந்து (ஒரு முதுகில் அணுகுமுறை): வலதுபுறம் உள்ள இடுப்பு (மத்திய ஸ்லிப்) பிரிக்கப்பட வேண்டும் அல்லது உயர்த்தப்பட வேண்டும், பின்னர் அதை சரிசெய்ய வேண்டும். அந்த சரிசெய்தல் முதலில் பாதுகாக்கப்பட வேண்டும், எனவே விரல் ஆரம்பத்தில் நேராக செதுக்கப்பட்டு, உங்கள் கை சிகிச்சையாளரின் வழிகாட்டுதலின் கீழ் மெதுவாக வளைக்கப்படுகிறது.
உங்கள் கை சிகிச்சையாளர் உங்கள் அறுவை சிகிச்சை அணுகுமுறையின் திட்டத்தை பின்பற்றுவார். எந்த அணுகுமுறையை நீங்கள் பயன்படுத்தினாலும், புதிய மூட்டு ஒரு கீல்ஃ இது ஒரு நேர் கோட்டில் வளைந்து நேராக்கப்படுவதை விரும்புகிறது, ஆனால் அது பக்கவாட்டாக தள்ளப்படுவதையோ அல்லது திருப்பப்படுவதையோ விரும்பவில்லை. பக்கவாட்டு அழுத்தத்திலிருந்து பாதுகாப்பது நீண்ட காலத்திற்கு அதை நிலையானதாக வைத்திருக்கிறது.
முன்னெச்சரிக்கைகள் மற்றும் வரம்புகள்
- விரலை ஒரு நேர் கோட்டில் மட்டுமே நகர்த்தவும் (வளைத்தல் மற்றும் நேராக்குதல்) எந்த பக்கவாட்டு அல்லது திருப்பு சக்தி தவிர்க்க அறுவை சிகிச்சை செய்யப்பட்ட விரலில். புதிய மூட்டு ஒரு சுருள் மற்றும் பக்க அழுத்தம் அதை தளர்த்தலாம் அல்லது சிதைக்கலாம்.
- உங்கள் அணிய அடுப்பு வழிகாட்டுதலின்படி, மற்றும் பயன்படுத்தவும் தோழர் கயிறு விரல்களின் பாதையை நேராக வைத்திருப்பதற்கான செயல்பாடு.
- உங்கள் அறுவை சிகிச்சை விரலின் பின்புறத்தில் இருந்து, செய் இல்லை ஆரம்பத்தில் உங்களுக்குக் கொடுக்கப்பட்ட வரம்பைத் தாண்டி உங்கள் சொந்த நேராக்குதலைத் தள்ளுங்கள்: நேராக்குதல் தசை குணமடைகிறது.
- செய் இல்லை உங்கள் கை சிகிச்சை நிபுணர் வலுவூட்டல் (பொதுவாக ஆறு வாரங்களுக்குப் பிறகு) செல்லும் வரை உறுதியான பிடிப்பு, கடினமான பிஞ்ச், அல்லது கனமான அல்லது திருப்புதல் பணிகளைச் செய்யுங்கள்.
- மற்ற விரல் மூட்டுகள், உங்கள் மணிக்கட்டு மற்றும் உங்கள் தோள்பட்டை ஆகியவற்றை தொடக்கத்திலிருந்தே நகர்த்தி வைத்துக் கொள்ளுங்கள், மேலும் சாதாரணமான அன்றாட பணிகளுக்கு உங்கள் கையை வசதியாகப் பயன்படுத்தவும்.
காயம், வீக்கம் மற்றும் வடுக்கள் மேலாண்மை, நடைமுறையில் பார்க்க காயம் பராமரிப்பு வழிகாட்டல்.
உங்கள் பயிற்சிகள்
இவை உங்கள் கையேட்டில் உள்ள பயிற்சிகள். டாக்டர் ஹிர்பரா மற்றும் உங்கள் கை சிகிச்சையாளரின் வழிகாட்டுதலின்படி மட்டுமே அவற்றைத் தொடங்குங்கள், உங்களுக்கு வழங்கப்பட்ட வரம்புகள் மற்றும் வரம்புகளுக்குள் இருங்கள். ஆரம்ப வேலை விரலை பக்கவாட்டு அழுத்தம் இல்லாமல் ஒரு நேர் கோட்டில் நகர்த்த வைக்கிறதுஃ பாதுகாக்கப்பட்ட வளைவு, மென்மையான நேராக்குதல், தோழர் கயிறுகள் மற்றும் இடுப்பு சறுக்கல்கள். உங்கள் அறுவை சிகிச்சை விரலின் பின்புறத்திலிருந்து இருந்தால், சுறுசுறுப்பான நேராக்குதல் உடற்பயிற்சி என்பது ஆரம்பத்தில் பாதுகாக்கவும் மெதுவாக உருவாக்கவும் ஒன்றாகும். பிடியை வலுப்படுத்துவது ஒரு பிற்கால கட்டத்திற்கு சொந்தமானது, நீங்கள் குறிப்பாக அகற்றப்படும் வரை தொடங்கக்கூடாது. கூர்மையான வலியை ஏற்படுத்தும் அல்லது விரலை நிலையற்றதாக உணர வைக்கும் எதையும் நிறுத்துங்கள்.
உங்கள் மருத்துவ நெறிமுறை
இந்த பக்கத்தின் மீதமுள்ள பகுதி சிலிகான் பிஐபி கூட்டு ஆர்த்தோபிளாஸ்டிக்குப் பிறகு மறுவாழ்வுக்கான மருத்துவ நெறிமுறை ஆகும். இந்த பிரிவு உங்கள் கை சிகிச்சையாளருக்கு வழங்கப்பட வேண்டும், மேலும் ஒவ்வொரு கட்டமும் என்ன நடக்கிறது என்பதற்கான எளிய ஆங்கில விளக்கத்துடன் தொடங்குகிறது. நெறிமுறை அணுகுமுறை சார்ந்தது, மற்றும் இந்த மத்திய கிளை புள்ளிஃ ஒரு வான்வழி (கைவழி) அணுகுமுறை எக்ஸ்டென்சர் இயந்திரத்தை அப்படியே விட்டுவிட்டு, சில நாட்களுக்குள் ஆரம்ப செயலில் இயக்கத்தை அனுமதிக்கிறது; பின்புற அணுகுமுறை எனவே எக்ஸ்டென்சர் குணமடைவதை முதலில் எக்ஸ்டென்ஷன் ஆர்த்தெசிக்ஸ் மற்றும் படிப்படியான வளைவு மூலம் பாதுகாக்க வேண்டும். முழுவதும், சிலிகான் உள்வைப்பு ஒரு நெகிழ்வான இடைவெளி ஆகும், அதன் நீண்ட கால நிலைத்தன்மை பெரி-இன்ப்ளாண்ட் காப்ஸ்யூலைப் பொறுத்தது, எனவே கொரோனல் (பக்க) அழுத்தம் தவிர்க்கப்படுகிறது மற்றும் இயக்கம் ஒரு தூய sagittal வில் வைக்கப்படுகிறது.
சிகிச்சைக்கு முன்னர், சிகிச்சையளிக்கும் அறுவை சிகிச்சை அணுகுமுறை (புறம் மற்றும் முதுகில்), மத்திய ஸ்லிப் மற்றும் பக்கவாட்டு இழைகளின் ஒருமைப்பாடு / பழுது மற்றும் எந்தவொரு இன்ட்ரா-ஆபரேட்டிவ் வளைவு ஆகியவற்றை சிகிச்சையளிக்கும் அறுவை சிகிச்சையாளருடன் உறுதிப்படுத்தவும். டாக்டர் ஹிர்பாரா அணுகுமுறையை குறிப்பிடுவார்; அதற்கேற்ப புல (ஆரம்ப-செயலில்-நடவடிக்கை) அல்லது முதுகில் (நீட்டிப்பு-பாதுகாக்கப்பட்ட) பாதையைத் தேர்ந்தெடுக்கவும். எதிர்பார்க்கப்படும் செயல்பாட்டு இலக்கு தோராயமாக 40 60 ° வலி இல்லாத வளைவு, முழு வரம்பு அல்ல.
கட்டம் I பாதுகாப்பு மற்றும் இயக்கத்தைத் தொடங்குதல் (0 முதல் 3 வாரங்கள் வரை)
முதல் வாரங்கள் மென்மையான திசுக்களைப் பாதுகாக்கின்றன, அதே நேரத்தில் கடினத்தன்மையைத் தடுக்கின்றன, அணுகுமுறையால் முற்றிலும் அமைக்கப்பட்ட வேகத்துடன். உள்வைப்பு வளைவில் நீட்டிப்பில் நிலையானது, ஆனால் பக்கவாட்டு சுமைக்கு பாதிக்கப்படக்கூடியது, எனவே அனைத்து இயக்கங்களும் சுத்தமான சாகிட்டல் விமானத்தில் வைக்கப்படுகின்றன, மேலும் விரல் தோழர் கயிறு மற்றும் ஒரு அடுக்கு மூலம் ஆதரிக்கப்படுகிறது.
உங்கள் கை சிகிச்சையாளருக்கு:
கல்வி மற்றும் முன்னெச்சரிக்கைகள் - அடையாளம் காணவும் அறுவை சிகிச்சை (இதற்கு) இணையான பாதையை நீங்கள் பின்பற்றுங்கள். - வோலார் அணுகுமுறை: நீட்டிப்பு இயந்திரம் முழுமையாக → தொடங்கு 35 நாட்களில் செயலில் உள்ள PIP/DIP இயக்கம். ஒரு volar நீட்டிப்பு-பிளாக் / டெம்ப்ளேட் ஸ்பிளின்ட் அனுமதிக்கிறது பொருத்தவும் குறுகிய வளைவு வளைவு (பொதுவாக ஆரம்பத்தில் ~30°), படிப்படியாக அதிகரித்தது. - பின்புற அணுகுமுறை (மத்திய ஸ்லிப் பிளவு / சரிசெய்யப்பட்டது): பாதுகாப்பு நீட்டிப்பு. PIP கிட்டத்தட்ட முழு நீட்டிப்பு முழுநேரமாக; ஒரு செயலில் வளைவு அறிமுகப்படுத்த வரையறுக்கப்பட்ட குறுகிய வில் மேற்பார்வையின் கீழ், சென்ட்ரல்-ஸ்லிப் பழுதுபார்ப்பை மதிக்கவும். (ஒரு உறவினர்-நடவடிக்கை / டைனமிக்-நீட்டிப்பு திட்டத்தை அறுவை சிகிச்சையாளரின் விருப்பப்படி பயன்படுத்தலாம்.) - கொரோனல் (பக்க / ரேடியல்) அழுத்தத்தை கண்டிப்பாக தவிர்ப்பது அறுவை சிகிச்சையளிக்கப்பட்ட மூட்டு மீதுஃ தூய சாகிட்டல் டிராக்கிங்கை வழிநடத்த அருகிலுள்ள விரல் மீது பட்டி ஸ்ட்ராப். - பிடிப்பு, பிஞ்ச் அல்லது எதிர்ப்பு / சுமை பயன்பாடு இல்லை.
நிர்வாகம் - காயம்: பரிந்துரைப்படி அறுவை சிகிச்சை பாண்டேஜ்கள்; தொற்றுநோயை கண்காணிக்கவும் - வீக்கம்: உயர்வு, மென்மையான பின்னோக்கி மசாஜ், லேசான அழுத்தமான மடக்குதல் - பயிற்சிகள்ஃ பாதுகாக்கப்பட்ட செயலில் PIP/DIP வளைவுஅதிகரிப்பு அமைக்கப்பட்ட வில் உள்ள; இடுப்பு சறுக்கல்செயலில் ஈடுபடாத மூட்டுகளின் (டிஐபி, எம்சிபி, மணிக்கட்டு, கட்டைவிரல்) செயலில் இயக்கம்; செயல்பாட்டிற்காக தோழர் கயிறு கட்டுவதைத் தொடங்குங்கள் - உடற்பயிற்சி அமர்வுகளுக்கு இடையில் முழுநேரமாக அணிந்திருக்கும் ஸ்பிளெண்ட்
முன்னேற்றத்திற்கான அளவுகோல்கள் - காயம் திருப்திகரமாக குணமடைகிறது; எக்ஸ்டென்சர் தாமதம் உருவாகவில்லை (முதுகெலும்பு பாதை); தற்போதைய வட்டத்திற்குள் வசதியான, கட்டுப்படுத்தப்பட்ட இயக்கம்
கட்டம் II முன்கூட்டியே முன்மொழிவு (3 முதல் 6 வாரங்கள் வரை)
வளைவு வளைவு திறக்கப்பட்டு, பின்புற அணுகுமுறை விரல்களுக்கு, நீட்டிப்பு பாதுகாப்பு படிப்படியாக தளர்த்தப்படுகிறது, ஏனெனில் மத்திய ஸ்லிப் ஒருங்கிணைக்கிறது. இந்த சாளரத்தின் நோக்கம் ஸ்கார் முதிர்ச்சி வரம்பை சரிசெய்யும் முன் பயனுள்ள வளைவை (≈40 60 °) வளைப்பதாகும்.
உங்கள் கை சிகிச்சையாளருக்கு:
மதிப்பீடுகள் - செயலில் மற்றும் செயலற்ற PIP வளைவு; நீட்டிப்பு பின்னடைவு (முதுகுப் பாதை); கொரோனல் ஸ்திரத்தன்மை; வலி மற்றும் வீக்கம்; காயம்/காயம் பற்றிய ஆய்வு
கல்வி மற்றும் முன்னெச்சரிக்கைகள் - படிப்படியாக அனுமதிக்கப்பட்ட வளைவு வளைவை அதிகரிக்கவும் செயல்பாட்டு இலக்கை நோக்கி (≈4060°) - பறவை: அனுமதிக்கப்பட்டபடி செயலில் உள்ள வளைவை முன்கூட்டியே; நீட்டிப்பு முழு மற்றும் நிலையானதாக இருந்தால் மென்மையான செயலற்ற வளைவைச் சேர்க்கவும் - முதுகு: நடுத்தர ஸ்லிப் குணமடைதல் (பொதுவாக 4 6 வாரங்கள் முழுவதும் பகல்நேர ஆதரவு); நீட்டிப்பு தாமதத்திற்கு எதிராக பாதுகாக்கவும்ஃ செயலில் நீட்டிப்பு செலவில் வளைவைத் துரத்த வேண்டாம் - தொடரவும் பக்கவாட்டு / திருகு சுமைகளை கண்டிப்பாக தவிர்ப்பதுஇன்னும் வலுவூட்டல் எதிர்ப்பு இல்லை
நிர்வாகம் - உடற்பயிற்சிகள்ஃ படிப்படியான செயலில் மற்றும் செயலில்-உதவி PIP வளைவு நீட்டிப்பு; PIP இயக்கம் கவனம் செலுத்த தடுப்பு பயிற்சிகள்; இடுப்பு glides மற்றும் தோழர் strapping தொடர; தொடங்க காயம் குணமடைந்தவுடன் வடுக்கள் மசாஜ் - அருகிலுள்ள மூட்டுகளின் முழு இயக்கத்தையும் பராமரிக்கவும்
முன்னேற்றத்திற்கான அளவுகோல்கள் - குணமடைந்த காயம்; கொரோனல் விமானத்தில் நிலையான மூட்டு; செயல்பாட்டு வலி இல்லாத வில் நிறுவப்பட்டது; குறைந்தபட்ச நீட்டிப்பு தாமதம் (இறுதி)
கட்டம் III வலுவூட்டல் மற்றும் திரும்புதல் (6 முதல் 12 வாரங்கள் மற்றும் அதற்கு அப்பால்)
இயக்கம் நிறுவப்பட்டதும் மற்றும் மென்மையான திசுக்கள் ஒலி (சுமார் ஆறு வாரங்கள்), ஒளி வலுவூட்டல் தொடங்குகிறது மற்றும் படிப்படியாக கட்டமைக்கப்படுகிறது. வலுவூட்டல் அச்சு (பிடிப்பு மற்றும் நேர் கோடு சுமை) வைக்கப்படுகிறது, அதே நேரத்தில் உள்வைப்பில் பக்கவாட்டு / முறுக்கு அழுத்தம் இன்னும் நீண்ட காலத்திற்கு மதிக்கப்படுகிறது.
உங்கள் கை சிகிச்சையாளருக்கு:
மதிப்பீடுகள் - மற்ற பக்கத்திற்கு எதிராக பிடிப்பு மற்றும் பிஞ்ச்; இறுதி PIP வில்; கொரோனல் ஸ்திரத்தன்மை; செயல்பாட்டு மற்றும் பணி-குறிப்பிட்ட சோதனை
கல்வி மற்றும் முன்னெச்சரிக்கைகள் - தொடங்கு லேசான பிடிப்பு வலுவூட்டல் சுமார் ஆறு வாரங்களில், படிப்படியாக வளரும் - அறிமுகம் எச்சரிக்கையுடன் சுமைகளை அழுத்துதல் தொடரவும் வலுவான பக்கவாட்டு/சுருக்கும் சுமைகளை தவிர்க்கவும் அறுவை சிகிச்சை செய்யப்பட்ட மூட்டு மீது காலவரையின்றி (உள்வைப்பு நீண்ட ஆயுள்) - யதார்த்தமான எதிர்பார்ப்புகளை அமைக்கவும்: நீடித்த வலி நிவாரணம் முதன்மை ஆதாயம்; இறுதி வில் உள்ளது மிதமான (≈4060°) மற்றும் பெரும்பாலும் ~ 3 மாதங்களில் அமைக்கப்படுகிறது
நிர்வாகம் - உடற்பயிற்சிகள்: படிப்படியான பிடிப்பு/கட்டி வேலை; படிப்படியான செயல்பாட்டு மற்றும் வேலை சார்ந்த சுமைகள்; எஞ்சியுள்ள இயக்கம் மற்றும் வடுக்கள் வேலை ஆகியவற்றைத் தொடரவும் - ஒரு நிலையான, வசதியான, செயல்பாட்டு விரல் ஒரு பயனுள்ள வலி இல்லாத வில் அடையப்பட்டதும் வெளியேற்றத்தை கருத்தில் கொள்ளுங்கள் - குணமடையும் நிலை ஏற்பட்டால், மூட்டு நிலையற்றதாக / விலகினால், அல்லது உள்வைப்பு செயலிழப்பு சந்தேகிக்கப்பட்டால் சிகிச்சையளிக்கும் மருத்துவரை மீண்டும் தொடர்பு கொள்ளவும்
விடுவிப்பு / திருப்பிச் செலுத்துவதற்கான அளவுகோல்கள் - வசதியான, வலி இல்லாத, கொரோனல் நிலையான கூட்டு ஒரு செயல்பாட்டு வில்; போதுமான பிடியில்; தினசரி மற்றும் வேலை கோரிக்கைகளை சந்திக்க முடியும்
வேலை மற்றும் செயற்பாட்டிற்கு திரும்புதல்
இலகுவான அன்றாட கை பயன்பாடு (உண்ணல், எழுதுதல், இலகுவான சுய-பராமரிப்பு) ஆரம்பத்தில் இருந்தே, வசதியாக இருக்கும் வரை, அது ஒரு நேர் கோட்டில் இருக்கும் வரை மற்றும் அறுவை சிகிச்சையளிக்கப்பட்ட விரலில் பக்கவாட்டாக அல்லது வளைக்கும் சக்தியைத் தவிர்க்கும் வரை ஊக்குவிக்கப்படுகிறது. நீங்கள் சக்கரத்தை வசதியாகப் பிடிக்கவும், காரை பாதுகாப்பாகக் கட்டுப்படுத்தவும் முடிந்தவுடன், நீங்கள் எந்தவொரு கட்டுப்படுத்தும் அடுப்படியிலிருந்தும் வெளியேறினீர்கள், மேலும் நீங்கள் இனி வலுவான வலி மருந்துகளை எடுத்துக் கொள்ளவில்லை, பொதுவாக இரண்டு வாரங்கள், உங்கள் மதிப்பாய்வில் உறுதிப்படுத்தப்பட்டது.
இறுக்கமான பிடிப்பு மற்றும் ஏற்றப்பட்ட பணிகள் சுமார் வரை காத்திருக்கவும் ஆறு வாரங்கள், பின்னர் படிப்படியாக உருவாக்கப்படுகின்றன. கனமான கையேடு அல்லது திருப்புதல் வேலை என்பது திரும்புவதற்கான கடைசி விஷயம், மற்றும் போதுமான பிடியுடன் ஒரு வசதியான, நிலையான விரலை மீட்டெடுப்பதை அடிப்படையாகக் கொண்டது, இது டாக்டர் ஹிர்பாரா மற்றும் உங்கள் கை சிகிச்சையாளரால் தீர்மானிக்கப்படுகிறது, காலண்டர் மூலம் மட்டும் அல்ல. இந்த அறுவை சிகிச்சையின் நீடித்த ஒப்பந்தத்தை நினைவில் கொள்ளுங்கள்ஃ நம்பகமான வலி நிவாரணம் மற்றும் ஒரு 40 முதல் 60 டிகிரி வரையிலான பயனுள்ள வில், இடுப்பில் பக்கவாட்டு அழுத்தம் நீண்ட காலத்திற்கு உள்வைப்பை பாதுகாக்க தவிர்க்கப்படுகிறது.
உங்கள் நெறிமுறை பிறகு
இந்த நெறிமுறை நடைமுறையின் பொது மீட்பு ஆலோசனையுடன் இணைந்து செயல்படுகிறது; அறுவை சிகிச்சைக்குப் பிந்தைய வலியை நிர்வகித்தல், காயம் பராமரிப்பு மற்றும் வடு மேலாண்மைமேலே உள்ள படிப்படியான திட்டம் சிலிகான் பிஐபி கூட்டு ஆர்த்தோபிளாஸ்டிக்கு பிறகு வெளியிடப்பட்ட மறுவாழ்வு வழிகாட்டுதல்களை பிரதிபலிக்கிறது, மேலும் உங்கள் தற்போதைய மீட்பு டாக்டர் ஹிர்பரா மற்றும் உங்கள் கை சிகிச்சையாளர் தனித்தனியாக எந்த அறுவை சிகிச்சை அணுகுமுறை பயன்படுத்தப்பட்டது மற்றும் உங்கள் விரல் எவ்வாறு முன்னேறுகிறது என்பதைப் பொறுத்து வழிகாட்டப்படுகிறது.
Evidence & references
Silicone PIP Joint Replacement — Procedure Outcomes & Post-operative Rehabilitation (Swanson-type Arthroplasty for PIP Osteoarthritis)
Topic scope: post-operative rehabilitation after silicone (Swanson-type) proximal interphalangeal (PIP) joint arthroplasty for primary osteoarthritis. The worn joint surfaces are excised and a flexible silicone spacer is implanted; this is an interposition / encapsulation arthroplasty, not a rigidly-fixed mechanical hinge. The implant works as a flexible spacer around which a peri-implant fibrous capsule forms to provide stability. The dominant, reliable benefit is pain relief; the functional gain is a modest active arc (~40–60°), not restoration of normal range.
Defining principle of the rehab here: the rehabilitation pathway is dictated by the surgical approach, because the rate-limiting tissue is the extensor mechanism, not the implant. A volar (palmar) approach leaves the central slip and extensor mechanism intact → it permits immediate / early active motion (within 3–5 days). A dorsal approach must split or reflect the central slip to reach the joint → the extensor repair must be protected first with extension orthotics and a graded, short-arc flexion programme. Across both pathways the silicone spacer is stable in the sagittal (flexion–extension) plane but vulnerable in the coronal plane, so the programme deliberately avoids lateral / torsional load and tracks the joint in a pure sagittal arc (buddy strapping). Therapy aims to bank the useful arc before scar maturation fixes it while protecting extension and the implant — it is not an immobilise-to-heal construct in the volar case.
A. PROCEDURE OUTCOMES (silicone PIP arthroplasty for osteoarthritis)
Silicone PIP arthroplasty is a reliable pain-relieving operation with predictable but modest motion; the principal debates are over surgical approach and implant choice (silicone vs surface-replacement/pyrocarbon), not whether arthroplasty relieves pain.
- Pain relief is high and durable; motion gains are modest. A long-term series of Swanson silicone PIP arthroplasty for osteoarthritis (mean ~10-year follow-up) reported excellent pain relief (mean VAS ~0.4) with essentially unchanged arc (≈55° pre-op → ≈50° post-op) and high patient satisfaction — patients would have the surgery again despite limited motion gain [Bales, Wall & Stern, J Hand Surg Am 2014]. Moderate (level-IV long-term cohort).
- The volar approach can improve the active arc. A volar-approach silicone PIP series reported the active arc improving from ~33° to ~72°, with good function and satisfaction, by preserving the extensor mechanism and enabling early motion [Proubasta et al., J Hand Surg Am 2014]. Moderate–weak (level-IV).
- Radiographic implant deformation/fracture is common but poorly correlated with symptoms. In the long-term Swanson series most implants deformed and many fractured radiographically, yet clinical revision was uncommon (survivorship ~90% at ~10 years) and there was no correlation between radiographs and satisfaction [Bales, Wall & Stern 2014]. Strong natural-history signal within a cohort.
- Silicone vs surface-replacement and pyrocarbon implants give broadly comparable clinical results; no implant is clearly superior. Systematic review across implants/approaches found comparable outcomes with implant-/approach-specific complication profiles [Yamamoto et al., Plast Reconstr Surg 2017; Carlson Strother, Moran & Rizzo, JAAOS 2023]. Moderate (SR + narrative review).
- Pyrocarbon and resurfacing implants carry their own failure modes (subsidence, squeaking, intra-operative periprosthetic fracture, instability), informing implant choice rather than rehab [Watts et al., J Hand Surg Am 2012; Wagner et al. medium-term 2018 & intra-op fractures 2015; Branam et al. resurfacing-vs-silicone 2007]. Moderate.
B. REHABILITATION / THERAPY EVIDENCE
The central rehab questions are (1) how soon to move and (2) how to splint, and the answer to both is set by the surgical approach and the extensor mechanism. The evidence base is low-level (expert consensus / single-cohort therapy series) — there are no RCTs comparing PIP arthroplasty rehab pathways.
- Approach dictates the timeline (the core principle). Surgical reviews establish that a volar approach preserves the central slip and permits immediate active and passive motion, while a dorsal approach requires post-operative protection of the split/repaired central slip before flexion is advanced [Renfree, Bone Joint J 2022 (surgical approaches); Herren, Hand Clin 2017; Yamamoto et al. 2017]. Moderate (surgical evidence) — strong mechanistic basis.
- A structured 12-week, splint-based therapy programme is the consensus framework (dorsal pathway). Feldscher's hand-therapy protocol for PIP (pyrocarbon, central-slip-splitting dorsal approach) uses a volar static finger orthosis allowing a limited short-arc PIP/DIP active arc that is increased over the rehab course, with a hand-based resting splint (MCP flexed, PIP/DIP near 0°) for full-time use except during template-splint exercise [Feldscher, J Hand Ther 2010]. Weak (expert-consensus protocol).
- A defined controlled-motion program exists and reports good arcs. A controlled-motion rehabilitation program for PIP arthroplasty reported favourable range-of-motion outcomes, supporting graded controlled motion over rigid immobilisation [Ramanathan, Koludrovich & Evans, J Hand Ther 2021]. Weak (cohort / programme description).
- Static and dynamic extension splinting give similar results. A comparison of static vs dynamic splinting after PIP pyrocarbon arthroplasty found comparable outcomes, favouring static splinting for simplicity and patient convenience [Jennings & Livingstone / static-vs-dynamic cohort, J Hand Ther 2011]. Weak–moderate (comparative cohort).
- Coronal-plane protection is the durable, lifelong caveat. Collateral integrity and avoidance of lateral stress underpin long-term implant stability; collateral compromise drives instability/deviation [Carlo et al., collateral reconstruction, J Hand Surg Am 2016; Carlson Strother et al. 2023]. Consensus / mechanistic.
Recovery trajectory (expected, evidence-anchored)
| Phase | Window | Restraint (by approach) | Hand-therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Protect & initiate motion | Week 0–3 | Volar: active motion at 3–5 days, short flexion arc (~30°) in template/extension-block splint. Dorsal: PIP splinted near extension full-time; supervised short-arc flexion only | Protected sagittal PIP/DIP motion; tendon glides; buddy strapping; uninvolved-joint motion; no lateral/torsional load | None (no grip/pinch) | Implant stable in flexion–extension, vulnerable coronally |
| II — Advance motion | Week 3–6 | Progressively increase flexion arc toward ~40–60°. Dorsal: wean extension splint as central slip consolidates (≈wk 4–6); guard against extensor lag | Graded active/AAROM flexion–extension; blocking; scar massage once healed; continue buddy strapping | Still no resisted strengthening | Bank the useful arc before scar maturation fixes it |
| III — Strengthen & return | Week 6–12+ | Lifting/grip restrictions progressively lifted; lateral/twisting load avoided indefinitely | Light grip → cautious pinch; functional & work-specific loading | Grip from ~6 wk, graded | Pain relief is the durable gain; final arc (~40–60°) largely set by ~3 months |
(Phase windows mirror the precautions in the patient protocol; they are typical guides — not trial-derived deadlines — and the volar vs dorsal split is the dominant variable.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY
- Volar vs dorsal approach (the rehab-defining question). The volar approach spares the extensor mechanism and permits early active motion (and a better reported arc), at the cost of being more technically demanding; the dorsal approach is more familiar but mandates extensor protection and a slower, splint-led flexion programme. Choice is surgeon-dependent and drives the entire rehab pathway. Moderate surgical evidence; no head-to-head rehab RCT.
- Implant choice (silicone vs surface-replacement vs pyrocarbon). No implant is clearly superior on clinical outcomes; silicone is durable for pain relief with high radiographic deformation/fracture that poorly predicts symptoms, while pyrocarbon/resurfacing trade different complication profiles (subsidence, instability, intra-operative fracture). Moderate (SR + cohorts).
- Static vs dynamic splinting (dorsal pathway). Comparable outcomes; static splinting is favoured for simplicity and convenience. Weak–moderate.
- Motion gain is modest and that is expected, not failure. Patients reliably lose pain but gain little arc (especially via dorsal/silicone); mislabelling the modest arc as a poor result misframes a successful pain-relieving operation. Counsel the ~40–60° expectation up front. Strong natural-history signal.
- Lifelong coronal-stress avoidance. Long-term stability depends on the peri-implant capsule and collaterals; forceful lateral/twisting load risks deviation, instability and implant failure. Consensus.
D. EVIDENCE STRENGTH FLAGS (summary)
- STRONG (mechanistic / natural-history): the surgical-approach principle (volar preserves extensor mechanism → early motion; dorsal splits central slip → protect extension first); the modest-arc / reliable-pain-relief outcome pattern; radiographic implant deformation poorly predicting symptoms.
- MODERATE: procedure outcomes are level-IV case series (long-term Swanson silicone series; volar approach series); implant-comparison systematic review/narrative review; surgical-approach reviews.
- WEAK / EXPERT CONSENSUS: the specific rehabilitation regimen — short-arc controlled motion, 12-week splint-based programme, static-vs-dynamic splinting equivalence, exact phase timings. These are low-level, expert-consensus / single-cohort therapy descriptions, not trial-derived; individualise to the operative approach and tissue quality.
CITATIONS
RAG corpus (180,000+ Orthopaedic articles)
- Bales JG, Wall LB, Stern PJ. Long-term results of Swanson silicone arthroplasty for proximal interphalangeal joint osteoarthritis. J Hand Surg Am. 2014. DOI: 10.1016/j.jhsa.2013.11.008
- Proubasta IR, Lamas CG, Natera L, et al. Silicone proximal interphalangeal joint arthroplasty for primary osteoarthritis using a volar approach. J Hand Surg Am. 2014;39(6). DOI: 10.1016/j.jhsa.2014.03.033
- Weistra K, Kan HJ, van Alebeek VAHJ, et al. Proximal interphalangeal joint arthroplasty using a silicone implant: a comparison between Integra and NeuFlex in 72 cases. HAND. 2022. DOI: 10.1177/15589447221122829
- Branam BR, Tuttle HG, Stern PJ, et al. Resurfacing arthroplasty versus silicone arthroplasty for proximal interphalangeal joint osteoarthritis. J Hand Surg Am. 2007. DOI: 10.1016/j.jhsa.2007.04.006
- Yamamoto M, Malay S, Fujihara Y, et al. A systematic review of different implants and approaches for proximal interphalangeal joint arthroplasty. Plast Reconstr Surg. 2017. DOI: 10.1097/prs.0000000000003260
- Renfree KJ. Surgical approaches for proximal interphalangeal joint arthroplasty. Bone Joint J. 2022;104-B(12). DOI: 10.1302/0301-620x.104b12.bjj-2022-0946
- Herren DB. Current European practice in the treatment of proximal interphalangeal joint arthritis. Hand Clin. 2017. DOI: 10.1016/j.hcl.2017.04.002
- Carlson Strother CR, Moran SL, Rizzo M. Small joint arthroplasty of the hand: an update on indications, outcomes, and complications. J Am Acad Orthop Surg. 2023;31(15). DOI: 10.5435/jaaos-d-23-00034
- Feldscher SB. Postoperative management for PIP joint pyrocarbon arthroplasty. J Hand Ther. 2010. DOI: 10.1016/j.jht.2009.10.011
- Ramanathan D, Koludrovich J, Evans P. A new controlled motion program for rehabilitation of the proximal interphalangeal joint arthroplasty. J Hand Ther. 2021. DOI: 10.1016/j.jht.2019.04.003
- Watts AC, Hearnden AJ, Trail IA, et al. Pyrocarbon proximal interphalangeal joint arthroplasty: minimum two-year follow-up. J Hand Surg Am. 2012. DOI: 10.1016/j.jhsa.2012.02.012
- Wagner ER, Weston JT, Houdek MT, et al. Medium-term outcomes with pyrocarbon proximal interphalangeal arthroplasty: a study of 170 consecutive arthroplasties. J Hand Surg Am. 2018. DOI: 10.1016/j.jhsa.2018.06.020
- Wagner ER, Van Demark R, Kor DJ, et al. Intraoperative periprosthetic fractures in proximal interphalangeal joint arthroplasty. J Hand Surg Am. 2015. DOI: 10.1016/j.jhsa.2015.06.101
- McGuire DT, White CD, Carter SL, et al. Pyrocarbon proximal interphalangeal joint arthroplasty: outcomes of a cohort study. J Hand Surg Eur Vol. 2011;37(6). DOI: 10.1177/1753193411434053
- Carlo J, Dell PC, Matthias R, et al. Collateral ligament reconstruction of the proximal interphalangeal joint. J Hand Surg Am. 2016;41(1). DOI: 10.1016/j.jhsa.2015.10.007
- Aversano FJ, Calfee RP. Salvaging a failed proximal interphalangeal joint implant. Hand Clin. 2018. DOI: 10.1016/j.hcl.2017.12.011
PIP arthroplasty rehabilitation literature (URLs)
- Feldscher SB. Postoperative management for PIP joint pyrocarbon arthroplasty. J Hand Ther. 2010. https://pubmed.ncbi.nlm.nih.gov/20036511/
- Ramanathan D, Koludrovich J, Evans P. A new controlled motion program for rehabilitation of the proximal interphalangeal joint arthroplasty. J Hand Ther. 2021. https://pubmed.ncbi.nlm.nih.gov/31481342/
- Static versus dynamic splinting for proximal interphalangeal joint pyrocarbon implant arthroplasty: a comparison of current and historical cohorts. J Hand Ther. 2011. https://pmc.ncbi.nlm.nih.gov/articles/PMC3143198/
- Proubasta IR, et al. Silicone proximal interphalangeal joint arthroplasty for primary osteoarthritis using a volar approach. J Hand Surg Am. 2014. https://pubmed.ncbi.nlm.nih.gov/24799141/
- Bales JG, Wall LB, Stern PJ. Long-term results of Swanson silicone arthroplasty for PIP joint osteoarthritis. J Hand Surg Am. 2014. https://pubmed.ncbi.nlm.nih.gov/24559624/
- The dorsal approach to silicone implant arthroplasty of the proximal interphalangeal joint. J Hand Surg Am. 2007. https://www.sciencedirect.com/science/article/abs/pii/S0363502307004662
- Proximal interphalangeal joint arthroplasty using a silicone implant: a comparison between Integra and NeuFlex. HAND. 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC10953532/





