近端指间关节置换术
Patients › Rehabilitation
在手指近端指间关节(PIP关节)磨损后进行硅胶假体置换术,其受保护康复计划中,开始活动的速度取决于外科医生是从手指前方(掌侧)还是后方进入。
本方案旨在指导您完成手指中间关节(近端指间关节(PIP),即中间指节)置换术后的康复过程。该手术由基兰·希尔帕拉(Kieran Hirpara)医生在罗克汉普顿 Mater 私立医院采用柔性硅胶间隔物进行。方案首先介绍您的家庭锻炼计划,随后附上为您手治疗师制定的结构化临床方案。请在首次治疗访视时携带此页面或其 PDF 版本,以确保康复过程协调一致。您的治疗师可能会根据您的康复进展对计划进行调整。
如果您对术后伤口有任何疑虑,请与诊所联系。拍摄伤口照片并通过电子邮件发送以供审查通常很有帮助。
预期情况
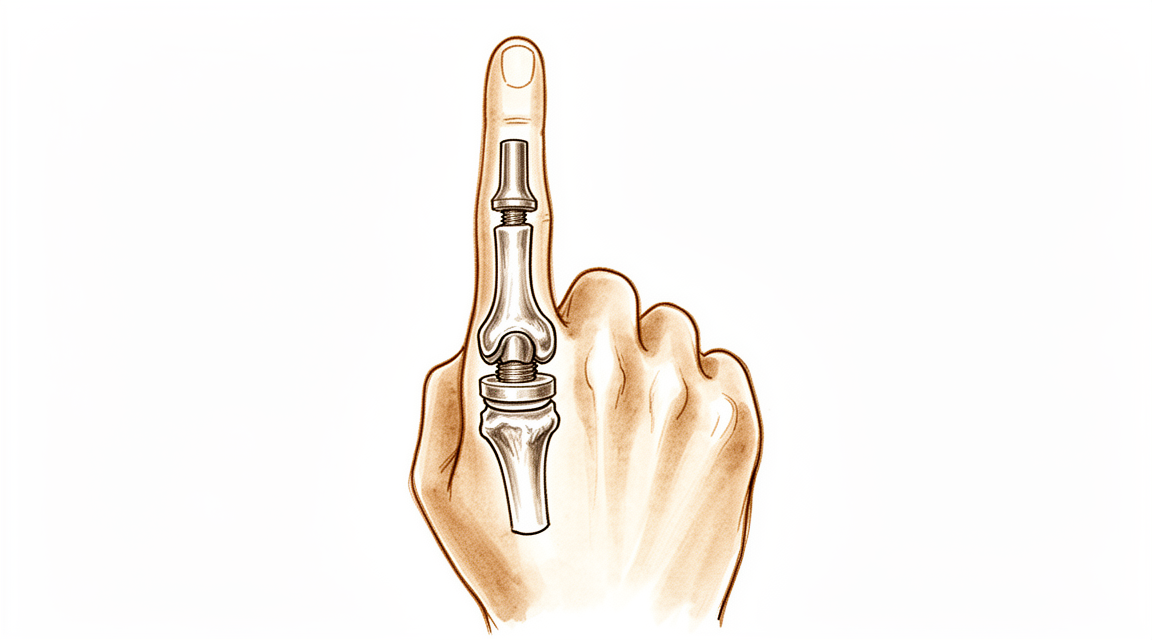
您的手指中间关节因关节炎而磨损,导致疼痛和僵硬。在此手术中,磨损的关节面被切除,并在两根骨头之间放置一个柔性硅胶间隔物(Swanson型植入物)。该间隔物并非刚性机械铰链,而是一种柔性的间隔物,它使骨头保持分离,允许手指弯曲,并让自身的瘢痕组织在其周围形成新的支撑套。最主要且最可靠的益处是缓解疼痛。您还应预期获得有用且适度的弯曲弧度(通常为40至60度),而非完全正常的活动范围。大多数人非常满意,因为疼痛消失且手指使用舒适。
康复过程中最重要的一点是手术入路的方向,因为这决定了您何时可以开始活动:
- 从前侧(掌侧,掌侧入路): 手指背侧的伸直肌腱保持完整。由于背侧无需愈合,您通常可在几天内开始活动手指。
- 从后侧(背侧入路): 伸直肌腱(中央束)必须被切开或抬起以到达关节,然后进行修复。该修复初期需加以保护,因此手指早期需夹板固定于伸直位,并在手部治疗师的指导下逐渐引入弯曲活动。
您的手部治疗师将根据您的手术入路执行计划。 Hirpara医生会告知他们使用了哪种入路,以下的时间安排也据此量身定制。无论您接受哪种入路,新关节都是一个铰链:它喜欢直线方向的弯曲和伸直,但不喜欢受到侧向推力或扭转。避免侧向应力是使其长期稳定的关键。
注意事项与限制
- 仅沿直线(屈曲和伸直)活动手指,避免对患指施加任何侧向或扭转力。新关节为铰链结构,侧向应力可能导致其松动或变形。
- 遵医嘱佩戴夹板,并在活动中使用邻指固定(buddy strapping)以保持手指轨迹笔直。
- 若手术切口位于手指背侧,请勿在早期自行将手指伸直超过规定的限度:伸肌腱正在愈合中。
- 在手治疗师允许进行强化训练之前(通常为术后约六周),禁止进行用力握持、强力捏取或负重及扭转动作。
- 从一开始就应保持其他指间关节、腕关节及肩关节的活动,并在舒适范围内用手进行日常轻度活动。
关于伤口、肿胀及瘢痕管理,请参阅诊所的伤口护理指南。
您的锻炼
这些是您讲义中的锻炼项目。仅在 Hirpara 医生和您的手部治疗师的指导下开始锻炼,并严格遵循您被允许的关节活动范围和限制。早期锻炼旨在使手指在直线范围内活动,避免侧向应力:包括保护性屈曲、轻柔的伸直、邻指固定(buddy strapping)以及肌腱滑动练习。如果您的手术是在手指背侧进行的,则需特别注意保护主动伸直锻炼,并缓慢逐步增加。握力强化属于后期阶段,在未获得明确许可前不得开始。任何引起锐痛或使手指感觉不稳定的动作均应立即停止。
您的临床方案
本页面其余部分为硅胶近端指间关节(PIP)置换术后康复的分阶段临床方案。本节内容将提供给您的手部治疗师,每个阶段均以通俗易懂的语言解释当前的治疗内容。本方案取决于手术入路,这是核心的分支点:掌侧(volar)入路保留伸肌机制完整,允许在数天内进行早期主动活动;背侧(dorsal)入路则切断或劈开中央束,因此必须首先通过伸展支具和分级屈曲来保护伸肌愈合。在整个过程中,硅胶假体作为柔性间隔物,其长期稳定性依赖于假体周围关节囊,因此避免冠状面(外侧)应力,并将活动限制在纯粹的矢状面弧内。
在治疗开始前,请与主治医生确认手术入路(掌侧与背侧)、中央束及侧副韧带的完整性/修复情况,以及术中活动范围。Hirpara 医生将指定入路;请据此选择掌侧(早期主动活动)或背侧(保护性伸展)路径。预期的功能目标是获得约 40–60° 的无痛活动范围,而非完全的活动范围。
第一阶段——保护并启动活动(第0至3周)
最初几周旨在保护软组织并防止僵硬,康复节奏完全由手术入路决定。植入物在屈伸方向上稳定,但侧向负荷下脆弱,因此所有活动均保持在纯净的矢状面内,手指通过邻指固定和夹板进行支撑。
致您的手部治疗师:
教育与注意事项 - 明确手术入路并遵循相应的康复路径: - 掌侧入路: 伸肌机制完整 → 于术后3–5天开始主动PIP/DIP活动。佩戴掌侧伸肌阻滞夹板/模板夹板,允许短屈曲弧(通常初始为~30°),并逐渐增加。 - 背侧入路(中央束切开/修复): 保护伸展。PIP关节全天候夹板固定于接近完全伸直位;在监督下引入受限的短弧主动屈曲,尊重中央束的修复情况。(可根据主刀医生偏好采用相对运动/动态伸展方案。) - 严格避免对手术关节施加冠状面(侧向/桡尺侧)应力:通过邻指固定引导纯矢状面轨迹。 - 禁止抓握、捏持或抗阻/负重使用。
管理措施 - 伤口:按医嘱进行外科敷料处理;监测感染迹象 - 水肿:抬高患肢、轻柔的向心性按摩、轻度加压包扎 - 锻炼:在设定弧度的保护下主动进行PIP/DIP屈伸活动;肌腱滑动练习;未受累关节(DIP、MCP、腕关节、拇指)的主动活动;开始在活动中使用邻指固定 - 锻炼间隙全天候佩戴夹板
进阶标准 - 伤口愈合满意;无伸肌滞后出现(背侧路径);在当前弧度内活动舒适且可控
第二阶段——活动度进阶(第3至6周)
屈曲弧逐渐打开,对于背侧入路的指趾,随着中央束的愈合,伸肌保护逐渐放宽。此阶段的目标是在瘢痕成熟固定关节活动度之前,建立有用的活动弧(约40–60°)。
为您手治疗师:
评估 - 主动和被动PIP关节活动弧;伸肌滞后(背侧入路);冠状面稳定性;疼痛和水肿;伤口/瘢痕复查
教育和注意事项 - 逐步增加允许的屈曲弧,向功能目标(约40–60°)迈进 - 掌侧: 在耐受范围内推进主动屈曲;若伸肌活动完全且稳定,可加入轻柔的被动屈曲 - 背侧: 根据中央束愈合情况逐步停用伸肌夹板(通常在4–6周期间逐步停用日间支撑);警惕伸肌滞后:切勿以牺牲主动伸肌活动为代价来追求屈曲 - 继续严格避免侧向/扭转负荷;尚未开始抗阻力量训练
管理 - 练习:分级主动及主动辅助PIP关节屈伸;针对PIP关节活动的阻断练习;继续肌腱滑动练习和邻指固定;伤口愈合后开始瘢痕按摩 - 保持相邻关节的全范围活动
进阶标准 - 伤口愈合;冠状面关节稳定;已建立无痛的功能性活动弧;伸肌滞后极小(背侧入路)
第三阶段——强化与恢复(第6周至12周及以后)
一旦关节活动度建立且软组织愈合良好(约6周时),即可开始轻度强化训练,并逐步增加强度。强化训练应保持在轴向(握力和直线负荷),长期尊重对植入物的侧向/扭转应力。
供手部治疗师参考:
评估 - 与健侧对比的握力和捏力;末次近端指间关节(PIP)活动弧;冠状面稳定性;功能性和任务特异性测试
教育与注意事项 - 从约6周开始进行轻度握力强化,并逐步增加 - 谨慎引入捏合负荷,并长期避免对患侧关节施加剧烈的侧向/扭转负荷(以延长植入物使用寿命) - 设定合理预期:持久的疼痛缓解是主要获益;最终活动弧较小(约40–60°),且在约3个月时基本固定
管理 - 练习:渐进式握力/治疗泥训练;分级功能性和工作特异性负荷;继续进行任何残留的活动度训练和瘢痕处理 - 当手指稳定、舒适、功能良好且拥有有用的无痛活动弧时,可考虑出院 - 如果恢复出现平台期、关节变得不稳定/发生偏斜,或怀疑植入物失效,请转诊回主治医生
出院/恢复标准 - 关节舒适、无痛、冠状面稳定且拥有功能性活动弧;握力充足;能够满足日常生活和工作需求
恢复工作与活动
从术后开始,即可在舒适范围内进行日常手部轻度活动(如进食、书写、轻度自理),前提是保持手指伸直,并避免对手术手指施加侧向或扭转力。通常在术后数周,当您能够舒适地握住方向盘并安全操控车辆、已拆除限制性夹板,且不再服用强效止痛药时,即可恢复驾驶,具体需经复查确认。
更用力的抓握及负重任务需等待至约六周,随后逐步增加。重体力劳动或涉及扭转的工作是最后恢复的,其时机取决于手指是否恢复至舒适、稳定状态且握力充足,由Hirpara医生及您的手部治疗师综合评估,而非仅依据日历时间。请记住,本手术的核心获益在于可靠的疼痛缓解及约40至60度的有用活动范围,长期内需避免关节承受侧向应力,以保护植入物。
术后方案
本方案与诊所的一般康复建议并行;请参阅术后疼痛管理、伤口护理和疤痕管理。上述分阶段计划反映了硅酮PIP关节成形术后的康复指南,您的持续康复将由Hirpara医生和您的手部治疗师根据所采用的手术入路及手指的恢复进展进行个体化指导。
Evidence & references
Silicone PIP Joint Replacement — Procedure Outcomes & Post-operative Rehabilitation (Swanson-type Arthroplasty for PIP Osteoarthritis)
Topic scope: post-operative rehabilitation after silicone (Swanson-type) proximal interphalangeal (PIP) joint arthroplasty for primary osteoarthritis. The worn joint surfaces are excised and a flexible silicone spacer is implanted; this is an interposition / encapsulation arthroplasty, not a rigidly-fixed mechanical hinge. The implant works as a flexible spacer around which a peri-implant fibrous capsule forms to provide stability. The dominant, reliable benefit is pain relief; the functional gain is a modest active arc (~40–60°), not restoration of normal range.
Defining principle of the rehab here: the rehabilitation pathway is dictated by the surgical approach, because the rate-limiting tissue is the extensor mechanism, not the implant. A volar (palmar) approach leaves the central slip and extensor mechanism intact → it permits immediate / early active motion (within 3–5 days). A dorsal approach must split or reflect the central slip to reach the joint → the extensor repair must be protected first with extension orthotics and a graded, short-arc flexion programme. Across both pathways the silicone spacer is stable in the sagittal (flexion–extension) plane but vulnerable in the coronal plane, so the programme deliberately avoids lateral / torsional load and tracks the joint in a pure sagittal arc (buddy strapping). Therapy aims to bank the useful arc before scar maturation fixes it while protecting extension and the implant — it is not an immobilise-to-heal construct in the volar case.
A. PROCEDURE OUTCOMES (silicone PIP arthroplasty for osteoarthritis)
Silicone PIP arthroplasty is a reliable pain-relieving operation with predictable but modest motion; the principal debates are over surgical approach and implant choice (silicone vs surface-replacement/pyrocarbon), not whether arthroplasty relieves pain.
- Pain relief is high and durable; motion gains are modest. A long-term series of Swanson silicone PIP arthroplasty for osteoarthritis (mean ~10-year follow-up) reported excellent pain relief (mean VAS ~0.4) with essentially unchanged arc (≈55° pre-op → ≈50° post-op) and high patient satisfaction — patients would have the surgery again despite limited motion gain [Bales, Wall & Stern, J Hand Surg Am 2014]. Moderate (level-IV long-term cohort).
- The volar approach can improve the active arc. A volar-approach silicone PIP series reported the active arc improving from ~33° to ~72°, with good function and satisfaction, by preserving the extensor mechanism and enabling early motion [Proubasta et al., J Hand Surg Am 2014]. Moderate–weak (level-IV).
- Radiographic implant deformation/fracture is common but poorly correlated with symptoms. In the long-term Swanson series most implants deformed and many fractured radiographically, yet clinical revision was uncommon (survivorship ~90% at ~10 years) and there was no correlation between radiographs and satisfaction [Bales, Wall & Stern 2014]. Strong natural-history signal within a cohort.
- Silicone vs surface-replacement and pyrocarbon implants give broadly comparable clinical results; no implant is clearly superior. Systematic review across implants/approaches found comparable outcomes with implant-/approach-specific complication profiles [Yamamoto et al., Plast Reconstr Surg 2017; Carlson Strother, Moran & Rizzo, JAAOS 2023]. Moderate (SR + narrative review).
- Pyrocarbon and resurfacing implants carry their own failure modes (subsidence, squeaking, intra-operative periprosthetic fracture, instability), informing implant choice rather than rehab [Watts et al., J Hand Surg Am 2012; Wagner et al. medium-term 2018 & intra-op fractures 2015; Branam et al. resurfacing-vs-silicone 2007]. Moderate.
B. REHABILITATION / THERAPY EVIDENCE
The central rehab questions are (1) how soon to move and (2) how to splint, and the answer to both is set by the surgical approach and the extensor mechanism. The evidence base is low-level (expert consensus / single-cohort therapy series) — there are no RCTs comparing PIP arthroplasty rehab pathways.
- Approach dictates the timeline (the core principle). Surgical reviews establish that a volar approach preserves the central slip and permits immediate active and passive motion, while a dorsal approach requires post-operative protection of the split/repaired central slip before flexion is advanced [Renfree, Bone Joint J 2022 (surgical approaches); Herren, Hand Clin 2017; Yamamoto et al. 2017]. Moderate (surgical evidence) — strong mechanistic basis.
- A structured 12-week, splint-based therapy programme is the consensus framework (dorsal pathway). Feldscher's hand-therapy protocol for PIP (pyrocarbon, central-slip-splitting dorsal approach) uses a volar static finger orthosis allowing a limited short-arc PIP/DIP active arc that is increased over the rehab course, with a hand-based resting splint (MCP flexed, PIP/DIP near 0°) for full-time use except during template-splint exercise [Feldscher, J Hand Ther 2010]. Weak (expert-consensus protocol).
- A defined controlled-motion program exists and reports good arcs. A controlled-motion rehabilitation program for PIP arthroplasty reported favourable range-of-motion outcomes, supporting graded controlled motion over rigid immobilisation [Ramanathan, Koludrovich & Evans, J Hand Ther 2021]. Weak (cohort / programme description).
- Static and dynamic extension splinting give similar results. A comparison of static vs dynamic splinting after PIP pyrocarbon arthroplasty found comparable outcomes, favouring static splinting for simplicity and patient convenience [Jennings & Livingstone / static-vs-dynamic cohort, J Hand Ther 2011]. Weak–moderate (comparative cohort).
- Coronal-plane protection is the durable, lifelong caveat. Collateral integrity and avoidance of lateral stress underpin long-term implant stability; collateral compromise drives instability/deviation [Carlo et al., collateral reconstruction, J Hand Surg Am 2016; Carlson Strother et al. 2023]. Consensus / mechanistic.
Recovery trajectory (expected, evidence-anchored)
| Phase | Window | Restraint (by approach) | Hand-therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Protect & initiate motion | Week 0–3 | Volar: active motion at 3–5 days, short flexion arc (~30°) in template/extension-block splint. Dorsal: PIP splinted near extension full-time; supervised short-arc flexion only | Protected sagittal PIP/DIP motion; tendon glides; buddy strapping; uninvolved-joint motion; no lateral/torsional load | None (no grip/pinch) | Implant stable in flexion–extension, vulnerable coronally |
| II — Advance motion | Week 3–6 | Progressively increase flexion arc toward ~40–60°. Dorsal: wean extension splint as central slip consolidates (≈wk 4–6); guard against extensor lag | Graded active/AAROM flexion–extension; blocking; scar massage once healed; continue buddy strapping | Still no resisted strengthening | Bank the useful arc before scar maturation fixes it |
| III — Strengthen & return | Week 6–12+ | Lifting/grip restrictions progressively lifted; lateral/twisting load avoided indefinitely | Light grip → cautious pinch; functional & work-specific loading | Grip from ~6 wk, graded | Pain relief is the durable gain; final arc (~40–60°) largely set by ~3 months |
(Phase windows mirror the precautions in the patient protocol; they are typical guides — not trial-derived deadlines — and the volar vs dorsal split is the dominant variable.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY
- Volar vs dorsal approach (the rehab-defining question). The volar approach spares the extensor mechanism and permits early active motion (and a better reported arc), at the cost of being more technically demanding; the dorsal approach is more familiar but mandates extensor protection and a slower, splint-led flexion programme. Choice is surgeon-dependent and drives the entire rehab pathway. Moderate surgical evidence; no head-to-head rehab RCT.
- Implant choice (silicone vs surface-replacement vs pyrocarbon). No implant is clearly superior on clinical outcomes; silicone is durable for pain relief with high radiographic deformation/fracture that poorly predicts symptoms, while pyrocarbon/resurfacing trade different complication profiles (subsidence, instability, intra-operative fracture). Moderate (SR + cohorts).
- Static vs dynamic splinting (dorsal pathway). Comparable outcomes; static splinting is favoured for simplicity and convenience. Weak–moderate.
- Motion gain is modest and that is expected, not failure. Patients reliably lose pain but gain little arc (especially via dorsal/silicone); mislabelling the modest arc as a poor result misframes a successful pain-relieving operation. Counsel the ~40–60° expectation up front. Strong natural-history signal.
- Lifelong coronal-stress avoidance. Long-term stability depends on the peri-implant capsule and collaterals; forceful lateral/twisting load risks deviation, instability and implant failure. Consensus.
D. EVIDENCE STRENGTH FLAGS (summary)
- STRONG (mechanistic / natural-history): the surgical-approach principle (volar preserves extensor mechanism → early motion; dorsal splits central slip → protect extension first); the modest-arc / reliable-pain-relief outcome pattern; radiographic implant deformation poorly predicting symptoms.
- MODERATE: procedure outcomes are level-IV case series (long-term Swanson silicone series; volar approach series); implant-comparison systematic review/narrative review; surgical-approach reviews.
- WEAK / EXPERT CONSENSUS: the specific rehabilitation regimen — short-arc controlled motion, 12-week splint-based programme, static-vs-dynamic splinting equivalence, exact phase timings. These are low-level, expert-consensus / single-cohort therapy descriptions, not trial-derived; individualise to the operative approach and tissue quality.
CITATIONS
RAG corpus (180,000+ Orthopaedic articles)
- Bales JG, Wall LB, Stern PJ. Long-term results of Swanson silicone arthroplasty for proximal interphalangeal joint osteoarthritis. J Hand Surg Am. 2014. DOI: 10.1016/j.jhsa.2013.11.008
- Proubasta IR, Lamas CG, Natera L, et al. Silicone proximal interphalangeal joint arthroplasty for primary osteoarthritis using a volar approach. J Hand Surg Am. 2014;39(6). DOI: 10.1016/j.jhsa.2014.03.033
- Weistra K, Kan HJ, van Alebeek VAHJ, et al. Proximal interphalangeal joint arthroplasty using a silicone implant: a comparison between Integra and NeuFlex in 72 cases. HAND. 2022. DOI: 10.1177/15589447221122829
- Branam BR, Tuttle HG, Stern PJ, et al. Resurfacing arthroplasty versus silicone arthroplasty for proximal interphalangeal joint osteoarthritis. J Hand Surg Am. 2007. DOI: 10.1016/j.jhsa.2007.04.006
- Yamamoto M, Malay S, Fujihara Y, et al. A systematic review of different implants and approaches for proximal interphalangeal joint arthroplasty. Plast Reconstr Surg. 2017. DOI: 10.1097/prs.0000000000003260
- Renfree KJ. Surgical approaches for proximal interphalangeal joint arthroplasty. Bone Joint J. 2022;104-B(12). DOI: 10.1302/0301-620x.104b12.bjj-2022-0946
- Herren DB. Current European practice in the treatment of proximal interphalangeal joint arthritis. Hand Clin. 2017. DOI: 10.1016/j.hcl.2017.04.002
- Carlson Strother CR, Moran SL, Rizzo M. Small joint arthroplasty of the hand: an update on indications, outcomes, and complications. J Am Acad Orthop Surg. 2023;31(15). DOI: 10.5435/jaaos-d-23-00034
- Feldscher SB. Postoperative management for PIP joint pyrocarbon arthroplasty. J Hand Ther. 2010. DOI: 10.1016/j.jht.2009.10.011
- Ramanathan D, Koludrovich J, Evans P. A new controlled motion program for rehabilitation of the proximal interphalangeal joint arthroplasty. J Hand Ther. 2021. DOI: 10.1016/j.jht.2019.04.003
- Watts AC, Hearnden AJ, Trail IA, et al. Pyrocarbon proximal interphalangeal joint arthroplasty: minimum two-year follow-up. J Hand Surg Am. 2012. DOI: 10.1016/j.jhsa.2012.02.012
- Wagner ER, Weston JT, Houdek MT, et al. Medium-term outcomes with pyrocarbon proximal interphalangeal arthroplasty: a study of 170 consecutive arthroplasties. J Hand Surg Am. 2018. DOI: 10.1016/j.jhsa.2018.06.020
- Wagner ER, Van Demark R, Kor DJ, et al. Intraoperative periprosthetic fractures in proximal interphalangeal joint arthroplasty. J Hand Surg Am. 2015. DOI: 10.1016/j.jhsa.2015.06.101
- McGuire DT, White CD, Carter SL, et al. Pyrocarbon proximal interphalangeal joint arthroplasty: outcomes of a cohort study. J Hand Surg Eur Vol. 2011;37(6). DOI: 10.1177/1753193411434053
- Carlo J, Dell PC, Matthias R, et al. Collateral ligament reconstruction of the proximal interphalangeal joint. J Hand Surg Am. 2016;41(1). DOI: 10.1016/j.jhsa.2015.10.007
- Aversano FJ, Calfee RP. Salvaging a failed proximal interphalangeal joint implant. Hand Clin. 2018. DOI: 10.1016/j.hcl.2017.12.011
PIP arthroplasty rehabilitation literature (URLs)
- Feldscher SB. Postoperative management for PIP joint pyrocarbon arthroplasty. J Hand Ther. 2010. https://pubmed.ncbi.nlm.nih.gov/20036511/
- Ramanathan D, Koludrovich J, Evans P. A new controlled motion program for rehabilitation of the proximal interphalangeal joint arthroplasty. J Hand Ther. 2021. https://pubmed.ncbi.nlm.nih.gov/31481342/
- Static versus dynamic splinting for proximal interphalangeal joint pyrocarbon implant arthroplasty: a comparison of current and historical cohorts. J Hand Ther. 2011. https://pmc.ncbi.nlm.nih.gov/articles/PMC3143198/
- Proubasta IR, et al. Silicone proximal interphalangeal joint arthroplasty for primary osteoarthritis using a volar approach. J Hand Surg Am. 2014. https://pubmed.ncbi.nlm.nih.gov/24799141/
- Bales JG, Wall LB, Stern PJ. Long-term results of Swanson silicone arthroplasty for PIP joint osteoarthritis. J Hand Surg Am. 2014. https://pubmed.ncbi.nlm.nih.gov/24559624/
- The dorsal approach to silicone implant arthroplasty of the proximal interphalangeal joint. J Hand Surg Am. 2007. https://www.sciencedirect.com/science/article/abs/pii/S0363502307004662
- Proximal interphalangeal joint arthroplasty using a silicone implant: a comparison between Integra and NeuFlex. HAND. 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC10953532/





