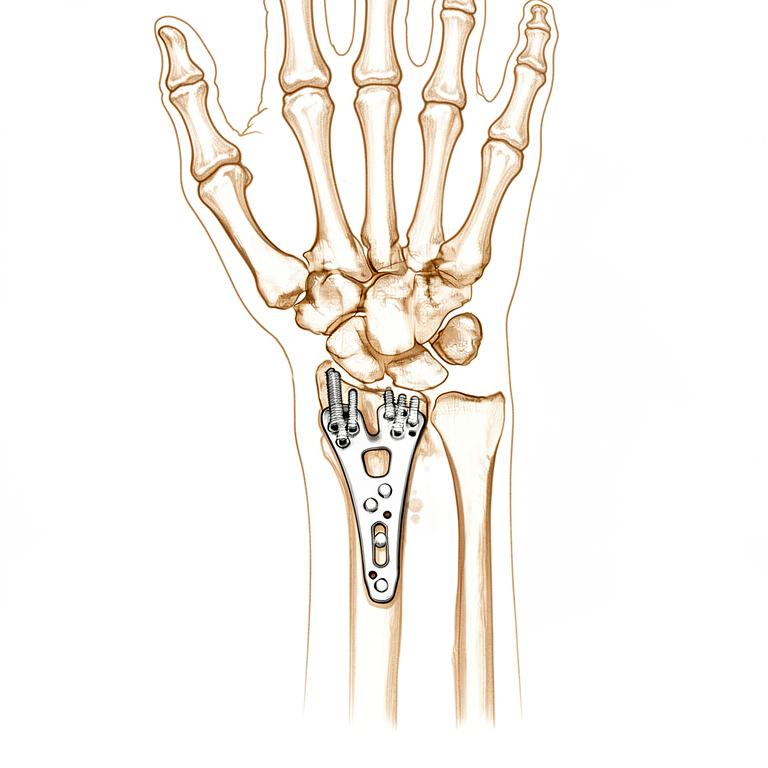
桡骨远端骨折(切开复位内固定术)
Patients › Rehabilitation
Staged rehabilitation after plate fixation of a distal radius fracture, from the first days to return to full activity.
本方案旨在指导您在基兰·希尔帕拉(Kieran Hirpara)医生于洛克汉普顿 Mater 私人医院接受桡骨远端(腕部)骨折切开复位内固定术(ORIF)后的康复过程。方案首先介绍您的家庭锻炼计划,随后是为您的物理治疗师或手部治疗师编写的结构化临床方案:请将此页面或其 PDF 文件带给您的首次治疗访视,以确保您的康复过程协调一致。您的治疗师可能会根据您的康复进展调整该计划。
如果您在术后对伤口有任何疑虑,请联系诊所。拍摄伤口照片并通过电子邮件发送以供审查通常很有帮助。
预期情况
关于伤口、肿胀和瘢痕管理,请参阅本诊所的伤口护理指南。
手术后,您可能被转诊至手治疗师以制作热塑性夹板。在此情况下,夹板将暂时佩戴以提供舒适和保护,您仍需在家进行锻炼时取下夹板。如果您被转诊制作夹板,您将收到有关佩戴和护理的更多信息。
以下练习对于恢复手指、手腕和前臂的活动度至关重要。热敷和冷敷是常用于恢复活动、恢复功能和改善舒适度的物理因子治疗方法。伤口愈合后,您可以在锻炼前热敷;锻炼后可使用冰袋以预防或减轻炎症。
瘢痕管理(尤其是按摩)在桡骨远端手术后非常重要,以便切口下方的肌腱保持自由滑动,避免与愈合中的瘢痕粘连(固定)。
掌侧锁定钢板的设计旨在足够牢固地固定骨折,以便尽早开始活动,本方案即基于此原则制定。比较早期手腕活动与掌侧钢板固定后数周制动期的研究表明,早期开始活动可在不损害骨折位置的前提下,改善短期内的活动度、握力和舒适度[1][2]。同时,比较约两周开始手腕活动与约六周开始手腕活动的试验发现,两组在术后三至六个月时结果相似[3],因此尽管早期活动具有益处,但无需急于求成,下文所述的稳步进展方案得到了充分支持。骨折愈合遵循其自身的时间线,与手腕的感觉无关,这就是为何即使活动变得舒适,仍需遵守后期注意事项(骨折后12周内禁止负重、提重物或参与对抗性运动)。
注意事项与限制
鼓励对手部进行轻度功能性使用,以完成日常活动,如自我护理、进食、穿衣、书写和打字。
术后长达8周内,重要的是避免提举、抓握、负重及冲击性活动。从大约第4周开始,逐步引入温和的力量训练,首先进行轻柔的手指活动和等长腕部练习,并谨慎增加强度,以免破坏早期的保护效果。
以下是您手册中的练习内容,旨在恢复手指、手腕和前臂的活动度。如果您佩戴夹板,请在练习时取下。请按照Hirpara医生和治疗师的指导开始练习。
您的练习
您的临床方案
本页面其余部分为经切开复位内固定术(使用掌侧钢板)治疗桡骨远端骨折的加速临床方案。本节内容将提供给您的物理治疗师或手治疗师,以下每个阶段均以通俗易懂的语言解释当前正在进行的处理。
术后第1–4天
在最初几天,重点是保护固定装置、减轻肿胀,并保持手指、手腕、前臂、肘部和肩部的活动。您的手术敷料将保留至第3天,届时将减少敷料并重新包扎伤口。休息时请抬高患手,在舒适范围内进行轻度日常活动(负重1–2公斤以下),避免手臂承重、紧握或提举重物。通常不需要夹板,但如果患者需重返工作岗位或手腕疼痛加重,可安排使用夹板。
致物理治疗师:
在治疗前,请查阅患者的X光片、手术报告及既往病史(PMHx),并与主刀医生沟通,以评估骨折固定的稳定性及预后情况。
教育与注意事项
- 避免手臂承重、紧握或提举重物
- 在疼痛耐受范围内及保持正常运动模式的前提下,鼓励使用患手进行轻度(小于1–2公斤)日常生活活动(ADL)
管理方案
- 夹板:通常无需使用,但若患者需重返工作岗位或疼痛加剧,可考虑使用;可选用热塑夹板或现成支撑具
- 伤口:手术敷料/绷带需保留至第3天;术后第3天起减少绷料并重新包扎伤口;提供伤口管理教育
- 水肿:提供抬高患肢的教育;根据需要施加压力治疗及逆行按摩
- 锻炼:提供“六块”主动锻炼以维持手指活动范围(ROM);提供手腕、前臂及手指的主动活动范围锻炼;鼓励定期进行肘部和肩部的主动活动范围锻炼
术后第2–4周
您的缝线将在术后第10–14天拆除,伤口愈合到一定程度后开始进行瘢痕按摩。锻炼计划继续进行(一旦手指恢复完全活动度,则停止“六组”练习),并开始轻柔的肌肉激活(等长)腕部强化训练。在此阶段,腕关节仍应仅依靠自身肌肉力量活动:在骨折仍在愈合期间,任何人(包括您自己)都不应对其进行被动推动或牵拉。请继续避免负重、紧握和提重物;鼓励进行1–2公斤以下的日常轻度活动。在腕部佩戴夹板期间严禁驾驶;经复查确认拆除夹板后,方可恢复驾驶。
致物理治疗师:
评估
- 患者自评量表:患者腕部评估量表(PRWE)、上肢功能残疾量表(DASH)
- 肢体周径测量(水肿)
- 视觉模拟疼痛评分(VAS)或数字评分量表
- 主动关节活动度(AROM)量角器测量:手、腕
- 主观回顾,包括患者对方案的依从性、手在日常生活活动(ADL)中的功能使用情况,以及存在的问题/顾虑
教育与注意事项
- 避免手臂负重、紧握或提重物
- 禁止被动活动腕关节
- 在疼痛限制和正常运动模式范围内,鼓励使用患手进行轻度(小于1–2公斤)的日常生活活动(ADL)
- 佩戴夹板期间严禁驾驶;经复查确认拆除夹板后,方可恢复驾驶
管理
- 伤口/瘢痕:术后第10–14天拆除缝线;根据愈合进展,酌情开始瘢痕管理
- 水肿:如有需要,考虑使用加压绷带、向心性按摩、手法水肿引流(MEM)、对比浴和/或抬高患肢
- 练习:一旦手指活动度完全恢复,则停止主动“六组”练习;如果手部主动活动度未完全恢复,可考虑被动手指和拇指练习,包括定位/保持练习;继续进行腕关节主动活动度练习;鼓励规律进行肘关节和肩关节主动活动度练习;开始腕部等长强化训练
故障排除
- 监测伤口感染迹象、手部感觉变化或复杂性区域疼痛综合征(CRPS)的早期迹象
- 识别异常运动模式并酌情干预
术后第4–6周
此阶段开始轻柔的力量训练:从第4周开始进行低阻力手指力量训练,同时继续进行等长腕部训练并逐步升级。如果X线片结果满意且固定稳定,可在术后4–6周开始轻柔的被动腕部拉伸(由另一只手或治疗师辅助移动腕部)。恢复活动度仍优先于力量增强。继续避免患肢负重和提重物,同时继续用手进行轻度的日常活动。
致物理治疗师:
评估
- 肢体周径水肿测量
- 视觉模拟疼痛评分(VAS)或数字评分量表(NRS)
- 主动关节活动度(AROM)量角器测量及运动模式质量评估
- 主观回顾,包括患者对治疗方案的依从性、手在日常生活活动(ADL)中的功能使用情况以及存在的问题/顾虑
- 握力测试(使用测力计,每侧肢体3次)
教育与注意事项
- 避免患肢负重或提重物
- 在疼痛限制和正常运动模式范围内,鼓励使用患手进行轻负荷(小于1–2公斤)的日常生活活动(ADL)任务
管理
- 瘢痕:根据需要继续瘢痕管理
- 水肿:根据需要继续加压治疗、逆行按摩、MEM(运动诱导运动)和抬高患肢;停止对比浴
- 练习:如果关节活动度(ROM)未完全恢复,继续被动手指和拇指练习;继续主动腕部ROM练习;第4周开始进行低阻力手指力量训练;如果切开复位内固定术(ORIF)稳定且X线片结果满意,在4–6周开始轻柔的被动腕部练习;鼓励规律进行肘部和肩部的主动ROM练习;继续/升级等长腕部力量训练
故障排除
- 复查复杂性区域疼痛综合征(CRPS)和肩痛的迹象
- 考虑家庭练习计划中的练习量,优先强调活动度(ROM)而非力量
- 如果腕部活动度显著受限,在获得外科医生批准且视觉模拟评分(VAS)低于4/10的情况下,考虑开始轻柔的被动关节活动度(PROM)腕部练习
术后第6–8周
此阶段在接下来的3周内逐步恢复至完全活动。腕部力量训练逐步增加至轻重量(0.5–1.0 公斤)或低阻力治疗带,手指力量训练的阻力也随之增加。仍有两项严格限制:在骨折后12周内,禁止负重、提重物或进行接触性运动。一旦您恢复完全的活动范围且功能恢复适宜,治疗师将考虑为您办理出院。
致您的物理治疗师:
评估
- 根据需要测量肢体周径以评估水肿
- 视觉模拟疼痛评分(VAS)或数字评分量表(NRS)
- 主动关节活动度(AROM)量角器测量
- 握力
- 主观回顾
教育与注意事项
- 在接下来的3周内逐步恢复至完全活动
- 骨折后12周内避免负重、提重物和进行接触性运动
管理
- 瘢痕:根据需要继续瘢痕管理
- 水肿:根据需要继续水肿管理
- 锻炼:如果关节活动度(ROM)未完全恢复,继续被动手指和拇指锻炼;如有需要,继续主动和被动腕关节活动度锻炼;增加手指力量训练的阻力;开始腕部力量训练,使用0.5–1.0 公斤的哑铃或低阻力治疗带;根据耐受情况,增加腕部力量训练计划中使用的重量和阻力
故障排除
- 如果关节活动度(ROM)改善缓慢,考虑/开始夜间连续渐进性夹板固定、拳击手套夹板或动态夹板固定
- 监测任何腕关节不稳的迹象,并酌情治疗
- 当关节活动度(ROM)完全恢复且功能恢复适宜时,考虑出院
- 如果病情停滞和/或预后不良,考虑转诊回主治医生
本方案由 Sarah Farrell, BOccThy AHT 和 Kristy Gerlach, BOccThy AHT 共同编写。
术后方案
本方案与诊所的一般康复建议并行;请参阅术后疼痛管理、伤口护理和手部治疗基础。关于手术本身及其治疗的损伤,请参阅桡骨远端固定术(切开复位内固定)和桡骨远端骨折。上述分阶段计划与掌侧锁定钢板固定术后康复的已发表证据一致,您的持续康复将由您的物理治疗师或手部治疗师根据您手腕的进展情况个体化指导。
参考文献
[1] Quadlbauer S, Pezzei C, Jurkowitsch J, 等. 与五周固定相比,使用掌侧锁定钢板固定的桡骨远端骨折早期活动可获得更好的短期预后:一项前瞻性随机试验. Arch Orthop Trauma Surg. 2022;142(5):1–11. https://pubmed.ncbi.nlm.nih.gov/34852677/ [2] Gutiérrez-Espinoza H, Araya-Quintanilla F, Olguín-Huerta C, 等. 早期与延迟活动对经掌侧锁定钢板治疗的桡骨远端骨折患者的有效性:系统综述和荟萃分析. Hand Surg Rehabil. 2020;39(4):261–271. https://www.sciencedirect.com/science/article/abs/pii/S2468122920302231 [3] Lozano-Calderón SA, Souer S, Mudgal C, Jupiter JB, Ring D. 桡骨远端骨折掌侧钢板固定后的腕关节活动. J Bone Joint Surg Am. 2008;90(6):1297–1304. https://pubmed.ncbi.nlm.nih.gov/18519324/ [4] Miller LK, Jerosch-Herold C, Shepstone L. 亚急性手部水肿管理技术的有效性:系统综述. J Hand Ther. 2017;30(4):432–446. https://pubmed.ncbi.nlm.nih.gov/28807598/
Evidence & references
Distal Radius Fracture (ORIF) — Post-operative Rehabilitation Evidence Brief
Topic scope: post-operative rehabilitation after open reduction and internal fixation (ORIF) of a distal radius fracture with a volar locking plate. This brief backs an early-motion-but-protected hand/wrist pathway delivered with hand therapy, where wrist motion begins early while bone-dependent loading (weight-bearing, heavy lifting, contact sport) is deferred until ~12 weeks. It does not cover the indications for surgery vs casting, nor fragment-specific/dorsal/bridge-plate constructs (which carry their own loading rules).
Defining principle of the rehab here: a volar locking plate is a fixed-angle construct stable enough to permit immediate wrist motion — the screws lock to the plate and hold the articular reduction independent of the cast. So (unlike a cast-treated fracture, and unlike a tendon or ligament repair) the wrist does not need weeks of immobilisation to protect the reduction: the rehab is an early-movement pathway — finger/forearm/wrist active motion and oedema control from day one, splint for comfort only, isometric then progressive strengthening from ~weeks 4–6. The one timeline that is not negotiable is bone healing: union takes ~6–12 weeks regardless of how the wrist feels, which is why weight-bearing, heavy lifting and impact are held to 12 weeks even once motion is comfortable.
A. PROCEDURE & CONSTRUCT — what the rehab is protecting
Volar locking plate fixation is the dominant operative construct for displaced distal radius fractures and is the reference standard against which other techniques are compared. Key surgical-outcome facts that shape the rehab:
- Volar locking plates restore and hold articular reduction reliably, and across randomised comparisons give equivalent or better functional outcomes than non-operative care and competing fixation methods (dorsal plating, intramedullary nailing, fragment-specific), with most differences favouring early function rather than final endpoint [JAAOS controversies review 2014; Hand Clinics plate-fixation review 2021; IM-nail-vs-volar-plate RCTs].
- The fixed-angle construct is the rationale for early motion. Because the locking screws hold the subchondral fragments rigidly, the plate — not a cast — maintains the reduction, so wrist motion can start before union without displacing the fracture [Hand Clinics 2021; accelerated-rehab RCT, JBJS 2014].
- In older patients the operative-vs-conservative outcome gap is small. A 3-year RCT in patients >70 found volar plating and non-operative care converged on similar patient-reported function — context that keeps post-operative rehab pragmatic and patient-centred rather than aggressive [BMC Musculoskelet Disord 2022; Hand Clinics geriatric review 2021].
- Recovery is gradual. Range, grip and patient-reported scores improve steadily over the first 3–6 months; the construct permits early motion but does not accelerate the biology of healing or the return of grip strength.
B. REHABILITATION / HAND-THERAPY EVIDENCE
The central rehab questions for this construct are (1) when to start wrist motion, (2) how much supervised therapy is needed, and (3) what the strengthening timeline should be. The evidence is clear on the first, nuanced on the second, and consensus-driven on the third.
- Early motion is safe and gives a short-term advantage. Multiple RCTs and a systematic review show that starting wrist motion early after volar plating improves short-term ROM, grip and comfort without compromising the radiographic reduction [accelerated-rehab RCT, JBJS 2014; early-vs-late motion RCT, HAND 2018; Hand Therapy systematic review 2020]. This is the direct warrant for the day-1 finger/forearm/wrist program in this protocol.
- "Early" need not mean "immediate," and the advantage washes out by 3–6 months. The landmark trial comparing wrist mobilisation at ~2 weeks vs ~6 weeks found the two groups equivalent by 3–6 months [Lozano-Calderón / JBJS 2008]. So there is a genuine early benefit but no penalty for a measured, comfort-led progression — which is exactly why this protocol can be unhurried.
- Routine supervised physiotherapy adds little over a coached home program for most patients. Systematic reviews and RCTs repeatedly find that a structured home exercise program preceded by instruction/coaching performs as well as formal supervised therapy for uncomplicated cases, and that prescribed exercise programs add limited benefit over advice for impairment/activity outcomes [HEP-vs-supervised SR, J Hand Ther 2014; J Physiother SR 2017; Hand Clinics "is therapy needed?" 2021; Arch Orthop Trauma Surg 2020]. This supports a home-program-first model with hand-therapy review, escalating supervision for stiffness, oedema or slow progress — the structure of this protocol.
- Oedema control and scar/tendon-glide management are standard therapy elements. Elevation, retrograde massage, manual oedema mobilisation and (early) compression are the evidence-informed oedema toolkit [edema-management SR, J Hand Ther 2017]; scar massage to keep the flexor tendons gliding under the volar incision is consensus hand-therapy practice rather than RCT-derived.
Phased post-op timeline (volar locking plate, early-motion pathway)
Phases match this topic's synthesis.md. Timings are post-operative weeks; the 12-week
loading limit is referenced to the fracture (injury) date.
| Phase | Window | Splint | Motion / use | Strengthening | Notes |
|---|---|---|---|---|---|
| I — Protect & move | Days 1–4 | Comfort only, not routine | Active finger (six-pack), wrist, forearm, elbow & shoulder ROM from day 1; light ADL < 1–2 kg within pain limits | — | Surgical bandage to day 3, then redress. Oedema control + elevation. No weight-bearing, gripping or lifting |
| II — Active range & oedema | Week 2–4 | Comfort/work only (no driving while splinted) | Continue active wrist ROM (no passive yet); six-pack stops once fingers full | Isometric wrist activation begins | Sutures out day 10–14; start scar massage once healed. Watch for CRPS. PRWE/DASH baseline |
| III — Passive range & light load | Week 4–6 | Off | Add gentle passive wrist stretches at 4–6 wk if x-ray satisfactory & fixation stable | Finger strengthening (low resistance) from wk 4; upgrade isometrics | Movement still prioritised over strength |
| IV — Graded strengthening & return | Week 6–8 | Off | Restore/maintain full active & passive ROM | Wrist strengthening with 0.5–1.0 kg / light theraband, progress as tolerated | Graded return over ~3 wk. No weight-bearing, heavy lifting or contact sport until 12 weeks post-fracture. Discharge on full ROM + functional return |
The phase structure mirrors published surgeon/hand-therapy ORIF protocols (early ROM → scar + oedema → passive range + light resistance → progressive strengthening, with heavy load/sport held to ~12–16 weeks) [Physiopedia Colles' ORIF protocol; institutional ORIF rehab guidelines].
C. KEY CONTROVERSIES / EVIDENCE QUALITY
- How early to mobilise. Early motion (immediate–2 wk) gives a real short-term ROM/grip/comfort advantage that equalises by 3–6 months vs starting at ~6 weeks. The evidence therefore supports early motion but does not mandate aggression — a measured progression is fully defensible. Moderate–strong (multiple RCTs + SR).
- Supervised therapy vs coached home program. For uncomplicated fractures the best available evidence finds no consistent benefit of routine formal physiotherapy over a well-instructed home program; supervision is best targeted to stiffness, oedema, CRPS risk or slow progress. Moderate (SRs/RCTs), but heterogeneous.
- Strengthening and return-to-load timing. The week-by-week strengthening ramp and the 12-week loading hold are construct- and biology-based consensus, drawn from surgeon/hand- therapy protocols rather than a strengthening-timing RCT. Weak/consensus.
- Whether the wrist needs any immobilisation at all. Some trials report that omitting post-op immobilisation does not worsen outcomes after volar plating, supporting the "splint for comfort only" stance here. Moderate.
D. EVIDENCE STRENGTH FLAGS (summary)
- STRONG / MODERATE–STRONG (RCT / SR): early wrist motion after volar plating is safe and improves short-term ROM/grip/comfort without loss of reduction (accelerated-rehab RCT JBJS 2014; early-vs-late RCT HAND 2018; Hand Therapy SR 2020); ~2-wk vs ~6-wk mobilisation equivalent by 3–6 months (Lozano-Calderón JBJS 2008).
- MODERATE: volar locking plate is a reliable fixed-angle construct with equivalent/favourable outcomes vs alternatives (JAAOS 2014; Hand Clinics 2021); operative-vs-conservative outcomes converge in the elderly (BMC 2022); coached home program ≈ supervised therapy for uncomplicated cases (J Hand Ther 2014; J Physiother 2017; Hand Clinics 2021); evidence-based oedema management (J Hand Ther 2017).
- WEAK / CONSENSUS: the detailed strengthening ramp and 12-week loading limit (surgeon & hand-therapy protocols; biology- and construct-based, not trial-derived); scar/tendon-glide massage practice.
CITATIONS
RAG corpus (180,000+ Orthopaedic articles)
- Accelerated rehabilitation compared with a standard protocol after distal radial fractures treated with volar open reduction and internal fixation. J Bone Joint Surg Am. 2014. DOI: 10.2106/jbjs.m.00860
- Wrist mobilization following volar plate fixation of fractures of the distal part of the radius. J Bone Joint Surg Am. 2008. DOI: 10.2106/jbjs.g.01368
- Early versus late motion following volar plating of distal radius fractures. HAND. 2018. DOI: 10.1177/1558944718787880
- A systematic review of how daily activities and exercises are recommended following volar plating of distal radius fractures and the efficacy and safety of early versus late mobilisation. Hand Therapy. 2020. DOI: 10.1177/1758998320967032
- AAOS/ASSH Clinical Practice Guideline Summary: Management of Distal Radius Fractures. J Am Acad Orthop Surg. 2022. DOI: 10.5435/jaaos-d-21-00719
- Controversies in the management of distal radius fractures. J Am Acad Orthop Surg. 2014. DOI: 10.5435/jaaos-22-09-566
- Plate fixation of distal radius fractures. Hand Clinics. 2021. DOI: 10.1016/j.hcl.2021.02.008
- Non-operative treatment or volar locking plate fixation for dorsally displaced distal radius fractures in patients over 70 years — a three-year follow-up of a randomized controlled trial. BMC Musculoskelet Disord. 2022. DOI: 10.1186/s12891-022-05394-7
- Distal radius fracture: HEP versus supervised therapy — a systematic review. J Hand Ther.
- DOI: 10.1016/j.jht.2013.08.017
- Prescribed exercise programs may not be effective in reducing impairments and improving activity during upper limb fracture rehabilitation: a systematic review. J Physiother. 2017. DOI: 10.1016/j.jphys.2017.08.009
- Is therapy needed after distal radius fracture treatment — what is the evidence? Hand Clinics.
- DOI: 10.1016/j.hcl.2021.02.012
- Rehabilitation after distal radius fractures: is there a need for immobilization and physiotherapy? Arch Orthop Trauma Surg. 2020. DOI: 10.1007/s00402-020-03367-w
- Management of complications of distal radius fractures. Hand Clinics. 2015. DOI: 10.1016/j.hcl.2014.12.002
- A comparison of the accuracy of two sets of diagnostic criteria in the early detection of complex regional pain syndrome following surgical treatment of distal radial fractures. J Hand Surg Eur Vol. 2012. DOI: 10.1177/1753193412469142
Distal radius / rehabilitation literature (URLs)
- AAOS/ASSH Clinical Practice Guideline Summary: Management of Distal Radius Fractures (full summary). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC9196973/
- Practical application of the 2020 distal radius fracture AAOS/ASSH clinical practice guideline: a clinical case. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC9035062/
- Rehabilitation for distal radial fractures in adults (Cochrane-style review). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC9250132/
- Rehabilitation after distal radius fractures: opportunities for improvement. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC10569825/
- Rehabilitation following surgically treated distal radius fractures: do immobilization and physiotherapy affect the outcome? PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8343619/
Published rehab protocols (surgeon / hand-therapy — basis for the phase structure)
- British Society for Surgery of the Hand / British Association of Hand Therapists — Distal Radius Fractures Working Group rehabilitation guidance (2024). https://www.hand-therapy.co.uk/_userfiles/pages/files/distal_radius_fractures_working_group_2024.pdf
- Colles' Fracture Post-Operative Rehabilitation Protocol. Physiopedia. https://www.physio-pedia.com/Colles%E2%80%99_Fracture_Post_Operative_Rehabilitation_Protocol
- Distal Radius ORIF Rehabilitation Guidelines. University of Virginia Department of Orthopaedic Surgery. https://med.virginia.edu/orthopaedic-surgery/wp-content/uploads/sites/242/2024/09/Distal-radius-ORIF.pdf
- Distal Radius ORIF Rehabilitation. Jared Lee, MD. https://jaredleemd.com/pdf/distal-radius-orif-rehabilitation/





