肱骨近端骨折切开复位内固定术(钢板和髓内钉固定)
为何建议进行此手术
切开复位内固定术是一种通过钢板和螺钉将骨折断端重新对齐并固定的手术。您的外科医生可能建议您进行此手术,因为保守治疗选项(如休息和制动)未能提供足够的改善。虽然许多患者无需手术即可良好愈合,但您的特定骨折类型可能需要机械稳定性以确保正确愈合。这种方法特别适用于骨折碎片偏离自然位置的移位性骨折。
此手术的主要目标是恢复您肩部的稳定性,从而减轻疼痛并改善您使用手臂的能力。对于骨密度健康的患者,该方法可提供良好的长期结果。然而,了解风险至关重要。在60岁以上的患者中,并发症发生率为44%,失败率为34%。术后您必须佩戴悬吊带,且至少六周内不得驾驶。一旦您的外科医生在六周复查时解除限制,您方可恢复驾驶。更多详情,请参阅上肢手术后驾驶。
手术前
请在手术前禁食八小时。仅在您的外科医生建议后停止服用抗凝药物。安排接送回家,因为任何肩部手术后至少六周内不得驾驶。请携带所有当前用药的清单,并穿着舒适、宽松的衣物。您可能需要接受X线检查、血液检查或麻醉评估,以检查您的健康状况并规划手术。您的外科医生将采用开放入路,在肩部做一个单一切口。这可以直接进入以使用钢板和螺钉固定骨折。请遵循您的外科医生关于药物调整和到达时间的具体指示。
手术当天
本手术在全身麻醉联合区域神经阻滞下进行。手术期间您将完全入睡,神经阻滞(在苏醒前对支配手臂的神经进行注射以产生麻木效果)可在术后最初 12 至 24 小时内提供镇痛。麻醉师将在术前与您会面,并向您详细说明这两个部分。
您将抵达医院并办理入院。您的外科医生将在手术部位做一个常规的单一切口以固定骨折。随后您将进入手术室。术后,您将在复苏室苏醒。您的手臂将置于吊带中。无论哪一侧手臂接受了手术,肩部手术后至少六周内均不得驾驶。经您的外科医生批准(通常在六周复查时),您可恢复驾驶。更多详情,请参阅 上肢手术后的驾驶。
手术内容
您的外科医生会在您肩部前方做一个长约 8 至 10 厘米的切口。这种开放入路可为骨折部位提供清晰的视野。通过该切口,您的外科医生会小心地移开周围组织,以显露骨折部位。
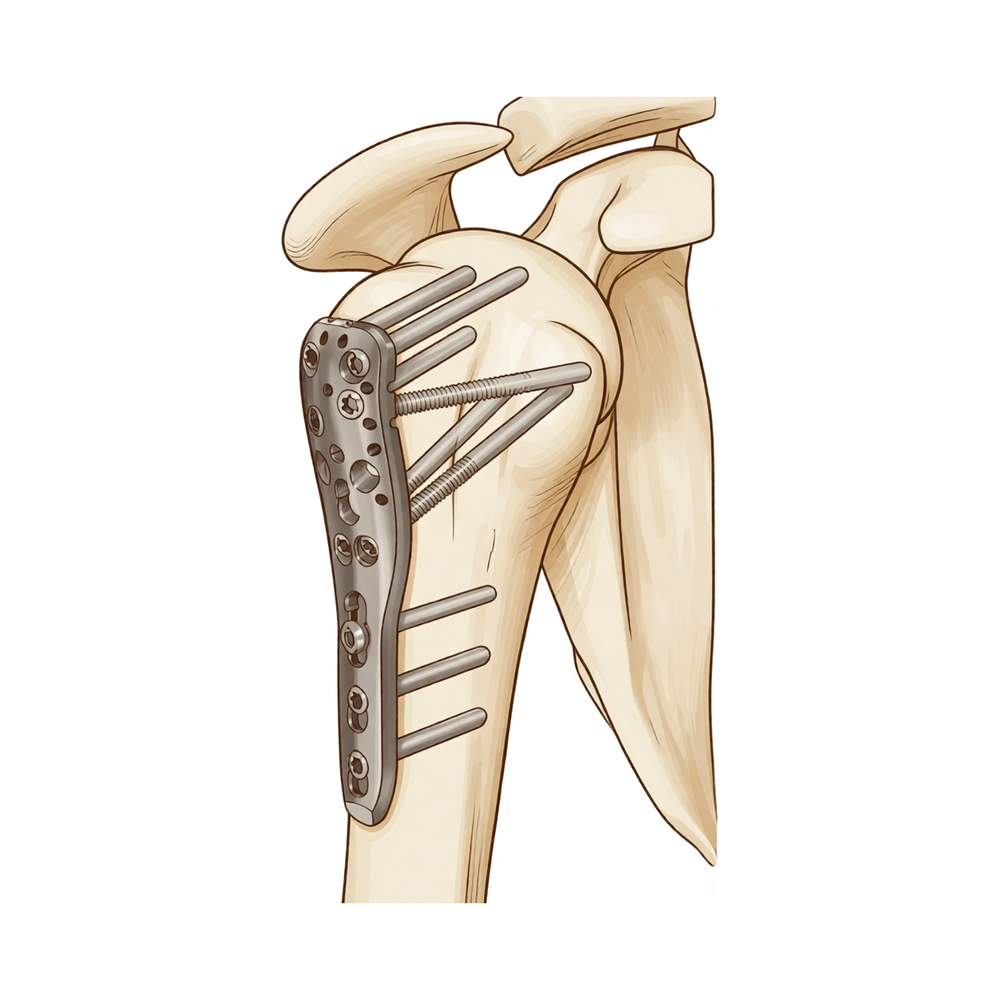
您的上臂骨骨折断端将被重新对位至正确位置。随后,您的外科医生将使用金属接骨板和螺钉将骨折块固定在一起。该接骨板起到内夹板的作用,在骨骼愈合过程中保持其稳定。在某些情况下,可能会在骨干部位中心置入一根金属髓内钉以提供支持。该髓内钉通过上下两端的螺钉进行固定。
您的外科医生会检查内固定的强度和稳定性。随后,切口将通过缝合线或吻合钉闭合。最后,敷上无菌敷料以保护伤口。
手术通常持续 1 至 2 小时。术后您将佩戴悬臂带以支撑手臂。无论手术哪一侧手臂,术后至少六周内不得驾驶车辆。您应等待外科医生许可后方可再次驾驶,通常可在术后六周复查时获得许可。更多详情,请参阅 上肢手术后驾驶。
术后
您将在复苏室苏醒,手臂佩戴吊带,切口处覆盖敷料。您的外科医生将管理您的疼痛,以确保您舒适。您应安排他人在术后24小时内陪伴您。大多数患者在该手术后需住院一晚,但部分患者可于同日出院。无论哪一侧手臂接受手术,您在肩部手术后至少六周内不得驾驶。经您的外科医生许可后,您方可恢复驾驶,通常可在六周复查时获得许可。详见上肢手术后驾驶以获取更多信息。在下一次就诊前,请保持敷料清洁干燥。
恢复过程
您的肩部将有一个切口。在最初几天,疼痛和肿胀是正常的。您的外科医生会开具药物以帮助您保持舒适。休息时支撑手臂有助于减轻肿胀。您需要佩戴悬带来保护修复部位。请按照指示佩戴。
您的物理治疗师将指导您进行锻炼。早期活动对愈合非常重要。手术后不久,您将开始进行轻柔的活动。这有助于防止僵硬。在您的外科医生允许之前,请勿提重物或举手过头。简单的任务,如进食或刷牙,可能可以用未手术的手臂完成。
起初睡觉可能会有困难。尝试用枕头支撑身体。这可以减轻肩部的压力。随着疼痛缓解和活动能力恢复,您将逐渐增加活动量。在您的外科医生允许后,您可以恢复驾驶,通常是在六周复查时。有关更多详细信息,请参阅上肢手术后的驾驶。
您的恢复时间表可能有所不同。您的外科医生和物理治疗师将根据您的愈合进度为您提供指导。大多数患者在一年内恢复到基础功能水平。坚持进行锻炼有助于获得最佳效果。
可能发生的问题
大多数患者恢复良好,但偶尔也会出现并发症。您的外科医生和医疗团队会密切监测您,以便尽早发现任何问题。
感染是此类手术后的严重风险。您可能会感到深部的搏动性疼痛,且普通止痛药无法缓解。切口周围的皮肤可能会变红、发热或肿胀。您可能会看到伤口有脓液或异常分泌物。如果出现发热或寒战,请立即联系诊所。这是一种可能严重影响您康复的严重并发症。
您的骨骼可能无法正确愈合。这称为骨不连。当您尝试活动手臂时,骨折部位可能会出现持续性疼痛。骨碎片可能会移位,导致出现咔哒声或研磨感。您的外科医生会在随访检查中排查这种情况。
您上臂骨(肱骨)头部的血液供应可能会受损。这称为缺血性坏死。您可能会感到肩部深处有酸痛感,且随时间推移加重。您的活动范围可能会减小。您可能会注意到僵硬感,且这种僵硬感不同于术后正常的酸痛。如有任何新的深部疼痛,请向您的外科医生报告。
用于固定骨骼的内固定物可能会失效。这包括钢板或螺钉松动或断裂。您可能会突然感到肩部感觉发生变化。可能会出现弹响感或稳定性丧失。如果您的手臂感到无力或不稳定,请立即寻求医疗建议。
如果您的骨折伴有脱位,再次手术的可能性更大。这意味着肩关节的肱骨头脱出了关节盂。您可能会注意到不稳定性,或感觉关节有滑脱感。如果出现这种情况,请及时联系您的外科医生。
老年患者面临更高的手术本身风险。60岁以上患者的住院不良事件和死亡率较高。您在住院期间可能会出现全身虚弱、意识混乱或呼吸困难。这些都是需要医疗团队立即关注的严重迹象。
本页面上的并发症表格列出了典型的发生率,如果您需要了解具体数据,请参阅该表格。
何时联系我们
如果您出现发热、伤口红肿加重或渗出,请立即联系我们。如突发剧烈疼痛、小腿肿胀或呼吸困难,请寻求紧急医疗救助。如果您感觉丧失或无法活动肢体,请立即与我们联系。这些症状需要紧急评估,以防止严重并发症的发生。
Evidence & references
Overview
- Locking plate fixation of proximal humerus fractures in patients older than 60 years is associated with a 44% complication rate and a 34% failure rate [1].
- ORIF of nonosteoporotic proximal humeral fractures with locking plates leads to favorable functional and radiologic outcomes at a minimum of 10 years of follow-up [2].
- Nail versus plate fixation of three-part proximal humeral fractures yields similar 1-year outcomes, suggesting both techniques are useful for internal fixation [3].
- Percutaneous treatment of selected proximal humeral fractures results in predictable union and good clinical results with a low rate of complications [5].
- Fixation of proximal humeral fractures with locking plates or locking intramedullary nails produces similar clinical and radiologic results [6].
- The locking plate is an excellent device for managing displaced unstable proximal humeral fractures and expands the indications for ORIF in these fractures [7].
- Distal AO/OTA C-type distal humerus fractures in older adults can be treated reliably with good outcomes using ORIF with modern locking plates [10].
- Locking plates are a good treatment alternative for elderly patients with displaced 2-part fractures of the surgical neck of the proximal humerus, offering acceptable complication rates and functional outcomes, provided rigorous attention is paid to avoid screw penetration [11].
- Patients undergoing ORIF for proximal humerus fracture dislocations have reasonable functional outcomes but relatively high avascular necrosis and reoperation rates [14].
- There are no level 1 studies in the English language literature comparing ORIF with hemiarthroplasty for proximal humeral fractures [17].
- Intramedullary fixation represents an alternative treatment option for proximal humeral fractures with specific fixation and biologic advantages, including reported outcomes comparable with other techniques [18].
- Locking plate fixation appears to provide a good option for the majority of patients with unstable proximal humeral fractures, with good functional outcomes [24].
Anatomy & Pathophysiology
- Reverse total shoulder arthroplasty can reliably improve shoulder function, patient satisfaction, and pain levels after failed open reduction and internal fixation of proximal humerus fractures [8].
- Greater tuberosity healing does not impact reverse shoulder arthroplasty biomechanics during abduction or forward flexion [30].
- Greater tuberosity healing affects reverse shoulder arthroplasty biomechanics during external rotation [30].
- Range of motion and strength thresholds can identify subjects with normal shoulder function in the context of proximal humerus fractures [31].
- With minimal and moderate amounts of glenohumeral abduction, glenohumeral joint forces are significantly displaced superiorly when inferior tuberosity placement occurs during hemiarthroplasty for four-part proximal humeral fractures [32].
- The biomechanical literature regarding proximal humerus fracture implants is diverse and heterogeneous [33].
- Biomechanical results regarding the safe distance between humerus shaft fracture and distal locking screws in antegrade nailing require confirmation with clinical studies [34].
- A minimally invasive approach combined with a novel anatomical locking plate provides a biomechanical basis to guide clinical treatment of scapular body fractures [35].
- Modified minimally invasive reduction osteosynthesis system (MIROS) fixation for Neer 2 and 3-Part proximal humeral fractures provides adequate fracture stability and permits early shoulder motion [36].
- Modified minimally invasive reduction osteosynthesis system (MIROS) fixation for Neer 2 and 3-Part proximal humeral fractures yields satisfactory functional and radiologic outcomes with fewer complications [36].
- Shoulder rotational ability is improved by systematically repairing tuberosities around the implant in complex shoulder fractures treated by reverse shoulder arthroplasty, provided their consolidation is anatomic [39].
- The insertion of the deltoid muscle in a 90° abduction position in the scapula plane is recommended for assessing objective strength using the Constant score [42].
- Dominance of the affected shoulder has no influence on functional and quality of life outcomes compared with the nondominant shoulder and should not be used to make treatment decisions [44].
- Reliable bony union and improved shoulder function can be expected with thoughtful surgical planning, appropriate implant choice, and meticulous surgical technique in the management of clavicle nonunion and malunion [45].
- Robot navigation-assisted intramedullary nail treatment for humeral shaft fractures helps surgeons determine the insertion point and proximal opening direction faster and more easily [46].
- Robot navigation-assisted intramedullary nail treatment for humeral shaft fractures shortens surgical time and reduces bleeding [46].
- Robot navigation-assisted intramedullary nail treatment for humeral shaft fractures avoids more intraoperative fluoroscopy [46].
- Robot navigation-assisted intramedullary nail treatment for humeral shaft fractures enables patients to achieve better shoulder functional outcomes [46].
- There is variability in the glenopolar angle with increased AP rotational offset of the shoulder radiograph, revealing inaccuracies even at institutions with established protocols [47].
- The SB suture anchor construct has superior interface contact immediately after fixation in humeral greater tuberosity fracture compared to the DR construct [48].
- The DR suture anchor construct offers better contact performance at all abduction angles with applied force in humeral greater tuberosity fracture compared to the SB construct [48].
- Varus and antecurvatum proximal humerus deformities as small as 15 degrees are associated with statistically significant alterations in glenohumeral joint mechanics in proximal humeral fracture malunion [49].
Classification
- The HGLS classification is a reliable method of describing fractures of the proximal humerus compared with the Neer and AO systems [79].
- The Neer fracture classification differentiates function in patients treated with locked plating for unstable proximal humeral fractures [82].
Clinical Presentation
- Locking plate fixation of proximal humerus fractures in patients older than 60 years is associated with a 44% complication rate and a 34% failure rate [1].
- Percutaneous treatment of selected proximal humeral fractures results in predictable union and good clinical results with a low rate of complications [5].
- Operative treatment, particularly open reduction and internal fixation, is an independent risk factor for inpatient adverse events and mortality in older-aged patients admitted with an isolated fracture of the proximal humerus [12].
- A majority of patients with proximal humeral fractures undergo non-operative treatment [20].
- Surgical treatment of proximal humerus fractures remains far from straightforward, with unpredictable outcomes where factors associated with poor results include being a woman, four-part fracture dislocation, and absence of metaphyseal head extension [64].
Investigations
- Locking plate fixation of proximal humerus fractures in patients older than 60 years is associated with a 44% complication rate and a 34% failure rate [1].
- ORIF of nonosteoporotic proximal humeral fractures with locking plates leads to favorable functional and radiologic outcomes at a minimum of 10 years of follow-up [2].
- Percutaneous treatment of selected proximal humeral fractures results in predictable union and good clinical results with a low rate of complications [5].
- In young, active patients with delayed presentation of complex proximal humeral fractures, ORIF with osteotomy and bone grafting is recommended to preserve the humeral head despite the risk of avascular necrosis, as conservative management yields poor functional outcomes [9].
- Failure of the calcar screw to purchase both the proximal and distal fragments was associated with a significantly higher rate of failure of fixation in the surgical treatment of proximal humeral fractures using a locking plate [16].
- The inherent nature of medial comminution of proximal humeral fracture may lead to inferior radiographic outcomes [76].
- BMD changes appeared swiftly in the proximal humerus after treatment of displaced 3- or 4-part fractures with ORIF, particularly affecting the proximal diaphysis [91].
- Intraoperative 3D imaging with a 160° orbital rotation yields sufficient image quality, enabling the reliable identification of intra-articular screws during plate osteosynthesis of the proximal humerus [92].
Treatment
Operative Fixation: Locking Plates
- Locking plate fixation of proximal humerus fractures in patients older than 60 years is associated with a 44% complication rate and a 34% failure rate [1].
- ORIF of nonosteoporotic proximal humeral fractures with locking plates leads to favorable functional and radiologic outcomes at a minimum of 10 years of follow-up [2].
- Primary ORIF is supported for medically fit patients with severely displaced fractures or fracture-dislocations of the proximal humerus in centers with appropriate expertise [4].
- Percutaneous treatment of selected proximal humeral fractures results in predictable union, good clinical results, and a low rate of complications [5].
- The locking plate is an excellent device for managing displaced unstable proximal humeral fractures and expands the indications for ORIF in these cases [7].
- Locking plates are a good treatment alternative for elderly patients with displaced 2-part fractures of the surgical neck, offering acceptable complication rates and functional outcomes, provided screw penetration is avoided [11].
- Operative treatment, particularly open reduction and internal fixation, is an independent risk factor for inpatient adverse events and mortality in older-aged patients admitted with an isolated proximal humerus fracture [12].
- Failure of the calcar screw to purchase both the proximal and distal fragments is associated with a significantly higher rate of fixation failure when using locking plates [16].
- Using the Locking Proximal Humerus Plate for all types of proximal humeral fractures is a reliable procedure with good results when careful planning and familiarity with the technique are maintained [19].
- Early results with locked plate fixation are encouraging, providing a potentially viable alternative to prosthetic replacement [23].
- The combined application of medial anatomical locking plate fixation and minimally invasive lateral locking plate fixation is effective in maintaining reduction and preventing varus collapse and implant failure in fractures with an unstable medial column [56].
- The Humerus Block technique is a predictable, minimally invasive, percutaneous operative technique for various proximal humeral fractures that results in good pain relief, mobility, and pull force with a low incidence of avascular necrosis [78].
- Long PHILOS plate fixation provides reliable secure fixation for complex humeral fractures, including long segment periarticular fractures, segmental fractures involving the proximal humerus and shaft, periprosthetic fractures around well-fixed humeral resurfacing prostheses, and pathological fractures [71].
- Dual plating is indicated for certain cases, particularly old ununited fractures where intramedullary nailing is difficult, but is contraindicated in severely comminuted fractures requiring extensive dissection [68].
Operative Fixation: Intramedullary Nails
- Fixation of proximal humeral fractures with locking plates or locking intramedullary nails produces similar clinical and radiologic results [6].
- The intramedullary nail is superior to the locking plate in reducing total complications, intraoperative blood loss, operative time, postoperative fracture healing time, and postoperative humeral head necrosis rate [13].
- Intramedullary fixation represents an alternative treatment option with specific fixation and biologic advantages and reported outcomes comparable to other techniques [18].
- Modern proximal humeral nail designs and techniques have demonstrated promising outcomes and can provide stable fixation [70].
Operative Fixation: Other Techniques
- Double plate fixation combined with autogenous iliac crest bone grafting results in successful salvage of humeral shaft nonunion after prior failed surgical interventions [15].
- An anterior approach for open reduction and internal fixation of humeral midshaft fractures allows supine positioning and yields union and complication rates comparable to a posterior approach [54].
- The use of a modified anterolateral approach and intra-osseous portal is safe and effective for minimally invasive reduction and plating of three-part proximal humeral fractures [53].
Operative vs. Non-Operative Management
- Similar 1-year outcomes for nail versus plate fixation of three-part proximal humeral fractures suggest both techniques are useful for internal fixation [3].
- A majority of patients with proximal humerus fractures undergo non-operative treatment [20].
- Nonsurgical management of proximal humerus fractures decreased during the study period analyzed in one cost-minimization analysis [69].
- There is no significant difference in clinical outcomes at 2 years between surgery and non-operative treatment in patients 60 years of age or older with displaced 2-part fractures of the proximal humerus [59].
- Nonsurgical treatment should have a more prominent role in the treatment of proximal humeral fractures, with better midterm outcomes observed compared to surgical treatment in one study [72].
- Treatment for proximal humerus fractures remains controversial, with nonsurgical management demonstrating successful outcomes and union rates greater than 90% [60].
- Most proximal humeral fractures in elderly patients can be treated nonoperatively with good functional outcomes [73].
- Short and long periods of immobilization yield similar results for nonoperatively treated proximal humeral fractures, independent of the fracture pattern [63].
Perioperative Considerations and Risk Factors
- The most important risk factors for postoperative opioid dependence following proximal humerus fractures are preoperative dependence and fracture complexity [80].
Complications
- Locking plate fixation of proximal humerus fractures in patients older than 60 years is associated with a 44% complication rate and a 34% failure rate [1].
- ORIF of nonosteoporotic proximal humeral fractures with locking plates leads to favorable functional and radiologic outcomes at a minimum of 10 years of follow-up [2].
- Percutaneous treatment of selected proximal humeral fractures results in a low rate of complications [5].
- Operative treatment, particularly open reduction and internal fixation, is an independent risk factor for inpatient adverse events and mortality in older-aged patients admitted with an isolated fracture of the proximal humerus [12].
- Intramedullary nailing is superior to locking plate fixation in reducing the total complication rate of proximal humerus fractures [13].
- Intramedullary nailing is superior to locking plate fixation in reducing the postoperative humeral head necrosis rate of proximal humerus fractures [13].
- ORIF of proximal humerus fracture dislocations carries a high rate of reoperation [27].
- The incidence of major wound complications after fixation of distal humerus fractures is substantial, with Grade III open fractures and the use of a plate to stabilize the olecranon osteotomy identified as significant risk factors [28].
- Acute deep infection after ORIF of proximal humeral fractures is a devastating complication with high complication rates, poor functional outcomes, and a notably high nonunion rate [93].
- Fixation of proximal humeral fractures in elderly patients using cement-augmented locked plates may result in lesser implant failure and total complication rates compared to using a locked plate alone [96].
- The overall complication rate of locking plate osteosynthesis for proximal humeral fractures has been decreasing considerably within the last years [97].
- In-hospital complications are more likely to occur after reverse shoulder arthroplasty than after locked plating for proximal humeral fractures [98].
- The risk of short-term complications is highest in patients undergoing shoulder arthroplasty for a fracture compared with nonfracture indications [101].
- Mortality at 1 year for fragility proximal humerus fractures is universally high regardless of risk factors [103].
- Complications of shoulder arthrodesis are not uncommon, including nonunion, malunion, fracture, and infection [107].
Recovery
- Locking plate fixation of proximal humerus fractures in patients older than 60 years is associated with a 44% complication rate and a 34% failure rate [1].
- ORIF of nonosteoporotic proximal humeral fractures with locking plates leads to favorable functional and radiologic outcomes at a minimum of 10 years of follow-up [2].
- Percutaneous treatment of selected proximal humeral fractures results in predictable union and good clinical results with a low rate of complications [5].
- Shoulder function, patient satisfaction, and pain levels can be reliably improved after reverse total shoulder arthroplasty for failed open reduction and internal fixation of fractures of the proximal humerus [8].
- In young, active patients with delayed presentation of complex proximal humeral fractures, ORIF with osteotomy and bone grafting is recommended to preserve the humeral head, despite the risk of avascular necrosis, as conservative management yields poor functional outcomes [9].
- The intramedullary nail is superior to locking plate in reducing total complication, intraoperative blood loss, operative time, postoperative fracture healing time, and postoperative humeral head necrosis rate of proximal humerus fractures [13].
- Patients undergoing ORIF for proximal humerus fracture dislocations have reasonable functional outcomes but relatively high avascular necrosis and reoperation rates [14].
- Double plate fixation combined with autogenous iliac crest bone grafting results in successful salvage of humeral shaft nonunion after prior failed surgical interventions [15].
- Elective implant removal in symptomatic patients after internal fixation of proximal humerus fractures improves clinical outcome, with symptomatic patients showing statistically significant improvement of the Constant score after implant removal [21].
- Delays beyond 5 days to surgery do not affect outcome following plate and screw fixation of proximal humerus fractures [22].
- ORIF of proximal humerus fracture dislocations carries a high rate of reoperation [27].
- Early active motion rehabilitation for postoperative treatment after locking plate fixation of proximal humerus fractures was not inferior to a restrictive treatment protocol after a follow-up period of 24 months [38].
- Intramedullary stabilization of proximal humeral fractures with an angular and sliding stable antegrade locking nail allows for immediate postoperative mobilization [50].
- Patients with proximal humeral fractures treated with early range of motion exercises do well, largely returning to baseline functional status by 1 year [51].
- Treatment with continuous passive motion (CPM) increases the range of motion after plate osteosynthesis of proximal humerus fractures in the first 6 weeks after surgery, but this effect is not sustained after 3 and 12 months [52].
- External fixation is a preferred surgical treatment option for paediatric proximal humerus fractures because early mobilization of the affected limb can be realized [62].
- The locked plate may prove useful in earlier pain-free rehabilitation of proximal humeral fractures [66].
- Ten years after locked plating of displaced proximal humeral fractures, patients show good to excellent outcomes in the majority of cases with no relevant decline compared with the shoulder function 1 year after surgery [67].
Key Evidence
- [L4] ORIF of proximal humerus fractures with locking plates in patients aged >60 years resulted in a 44% complication and 34% failure rate. [1] (10.1016/j.jse.2019.11.026)
- [L3] ORIF of nonosteoporotic proximal humeral fractures with locking plates led to favorable functional and radiologic outcomes at a minimum of 10 years of follow-up. [2] (10.1097/corr.0000000000002895)
- [L2] The similar 1-year outcomes for nail versus plate fixation of three-part proximal humeral fractures suggest that both techniques may be useful for internal fixation of these fractures. [3] (10.1007/s11999-011-2056-y)
- [L4] Our results support the use of primary ORIF in medically fit patients with a severely displaced fracture or a fracture-dislocation of the proximal part of the humerus in centers where the expertise to carry out such treatment exists. [4] (10.2106/jbjs.19.00595)
- [L4] Percutaneous treatment of selected proximal humeral fractures results in predictable union and good clinical results with a low rate of complications. [5] (10.1016/j.jse.2006.09.006)
- [L1] Fixation of proximal humeral fractures with locking plates or locking intramedullary nails produces similar clinical and radiologic results. [6] (10.1016/j.jse.2016.02.003)
- [L2] The locking plate is an excellent device in the management of displaced unstable proximal humeral fractures and is expanding the indications for ORIF in these fractures. [7] (10.1016/j.jse.2009.08.008)
- [L4] Shoulder function, patient satisfaction, and pain levels can be reliably improved. [8] (10.1016/j.jse.2016.05.020)
- [L4] In young, active patients with delayed presentation of complex proximal humeral fractures, ORIF with osteotomy and bone grafting is recommended to preserve the humeral head, despite the risk of avascular necrosis, as conservative management yields poor functional outcomes. [9] (10.1016/j.jse.2007.12.012)
- [L3] Distal AO/OTA C-type distal humerus fractures in older adults can be treated reliably and with good outcomes with ORIF using modern locking plates. [10] (10.1186/s12891-022-05431-5)
- [L4] Locking plates appear to be a good treatment alternative in elderly patients with a displaced 2-part fracture of the surgical neck of the proximal humerus with an acceptable complication rate and an acceptable functional outcome; however, rigorous attention has to be paid to avoid screw penetration. [11] (10.1016/j.jse.2009.11.046)
- [L3] Operative treatment, particularly open reduction and internal fixation, is an independent risk factor for inpatient adverse events and mortality in older-aged patients admitted with an isolated fracture of the proximal humerus and should perhaps be offered more judiciously. [12] (10.1016/j.jse.2013.09.006)
- [L1] The intramedullary nail is superior to locking plate in reducing the total complication, intraoperative blood loss, operative time, postoperative fracture healing time and postoperative humeral head necrosis rate of PHF. [13] (10.1186/s13018-019-1345-0)
- [L4] Patients undergoing ORIF for proximal humerus fracture dislocations have reasonable functional outcomes but relatively high avascular necrosis and reoperation rates. [14] (10.1016/j.jse.2022.04.018)
- [L4] Double plate fixation combined with autogenous iliac crest bone grafting results in successful salvage of humeral shaft nonunion after prior failed surgical interventions. [15] (10.1186/s12891-020-03743-y)
- [L3] Failure of the calcar screw to purchase both the proximal and distal fragments was associated with a significantly higher rate of failure of fixation in the surgical treatment of proximal humeral fractures using a locking plate. [16] (10.1302/0301-620x.107b9.bjj-2024-1649.r1)
- [L5] There are no level 1 studies in the English language literature comparing ORIF with hemiarthroplasty for proximal humeral fractures. [17] (10.1016/j.jhsa.2010.07.019)
- [L4] Intramedullary fixation represents an alternative treatment option for proximal humeral fractures with specific fixation and biologic advantages, including reported outcomes comparable with other techniques. [18] (10.5435/jaaos-d-18-00360)
- [L2] Using the Locking Proximal Humerus Plate for treatment of proximal humeral fractures of all types is a reliable procedure, with good results being obtained with careful planning and familiarity with the special features of the operative technique. [19] (10.1097/01.blo.0000137554.91189.a9)
- [L3] A majority of patients with proximal humeral fractures underwent non-operative treatment. [20] (10.1186/s12891-019-2812-9)
- [L4] Symptomatic patients after locked plate osteosynthesis for proximal humerus fractures showed statistically significant improvement of the Constant score after implant removal. [21] (10.1186/s12891-016-0977-z)
- [L3] Timing of surgery did not impact outcomes of patients who underwent ORIF for proximal humerus fractures. [22] (10.1016/j.jse.2025.02.019)
- [L4] Early results with locked plate fixation for the treatment of proximal humerus fractures have been encouraging, providing a potentially viable alternative to prosthetic replacement. [23] (10.5435/00124635-200805000-00008)
- [L4] Locking plate fixation appears to provide a good option for the majority of patients with unstable proximal humeral fractures, with good functional outcomes. [24] (10.1016/j.jse.2006.06.006)
- [L4] ORIF of proximal humerus fracture dislocations carries a high rate of reoperation. [27] (10.1016/j.jse.2021.01.025)
- [L4] The incidence of major wound complications after fixation of distal humerus fractures is substantial, with Grade III open fractures and the use of a plate to stabilize the olecranon osteotomy identified as significant risk factors. [28] (10.1016/j.jse.2013.09.014)
- [L5] Greater tuberosity healing does not seem to impact reverse shoulder arthroplasty biomechanics during abduction or forward flexion; however, it does affect biomechanics during external rotation. [30] (10.1016/j.jse.2019.07.022)
- [L3] Range of motion and strength thresholds can identify subjects with normal shoulder function. [31] (10.1016/j.jse.2010.06.005)
- [L5] With minimal and moderate amounts of glenohumeral abduction, glenohumeral joint forces are significantly displaced superiorly. [32] (10.1016/j.jse.2007.06.017)
- [L4] The biomechanical literature was found to be both diverse and heterogeneous. [33] (10.1186/s12891-015-0627-x)
- [L5] These biomechanical results, although very promising, should be confirmed with clinical studies. [34] (10.1186/s12891-025-08711-y)
- [L5] The study provided a biomechanical basis to guide the clinical treatment of scapular body fractures. [35] (10.1186/s13018-024-04905-7)
- [L3] It is a minimally invasive procedure that provides adequate fracture stability and permits early shoulder motion, with satisfactory functional and radiologic outcomes and fewer complications. [36] (10.1186/s12891-025-08600-4)
- [L2] Early active motion rehabilitation for postoperative treatment after locking plate fixation of proximal humerus fractures was not inferior to a restrictive treatment protocol after a follow-up period of 24 months. [38] (10.1016/j.jse.2025.01.042)
- [L3] Shoulder rotational ability is improved by systematically repairing the tuberosities around the implant, provided their consolidation is anatomic. [39] (10.1016/j.jse.2012.03.011)
- [L3] The authors recommend performing the measurement at the insertion of the deltoid muscle in a 90° abduction position in the scapula plane. [42] (10.1186/s12891-019-2795-6)
- [L3] Dominance of the affected shoulder has no influence and should not be used to make treatment decisions. [44] (10.1016/j.jse.2014.10.006)
- [L5] Reliable bony union and improved shoulder function can be expected with thoughtful surgical planning, appropriate implant choice, and meticulous surgical technique. [45] (10.1016/j.jse.2013.01.022)
- [L3] It can help surgeons determine the insertion point and proximal opening direction faster and more easily, shorten the surgical time, reduce bleeding, avoid more intraoperative fluoroscopy, and enable patients to achieve better shoulder functional outcomes. [46] (10.1186/s12891-024-07848-6)
- [L4] The study demonstrates variability in the glenopolar angle with increased AP rotational offset of the shoulder radiograph, revealing inaccuracies even at an institution with an established protocol. [47] (10.1302/0301-620x.95b8.30631)
- [L5] Findings suggest that despite the SB construct having superior interface contact immediately after fixation, the DR construct offered better contact performance at all abduction angles with applied force. [48] (10.1186/s12891-019-2412-8)
- [L5] Varus and antecurvatum proximal humerus deformities as small as 15 degrees were associated with statistically significant alterations in glenohumeral joint mechanics. [49] (10.5435/jaaos-d-20-00555)
- [L4] Intramedullary stabilization of proximal humeral fractures with an angular and sliding stable antegrade locking nail represents a minimally invasive procedure that provides a high degree of primary stability even in osteoporotic bone and allows for immediate postoperative mobilization. [50] (10.2106/00004623-200300004-00019)
- [L3] Patients with proximal humeral fractures treated with early range of motion exercises do well, largely returning to baseline functional status by 1 year. [51] (10.1016/j.jse.2007.07.016)
- [L1] The treatment with CPM increases the range of motion after plate osteosynthesis of proximal humerus fractures in the first 6 weeks after surgery, but this effect is not sustained after 3 and 12 months. [52] (10.1186/s13018-024-04804-x)
- [L3] The use of the modified anterolateral approach and intra-osseous portal is safe and effective for minimally invasive reduction and plating treatment for three-part proximal humeral fractures. [53] (10.1186/s13018-017-0701-1)
- [L3] An anterior approach allows supine positioning of the patient and yields union and complication rates comparable to those of a posterior approach with plate fixation for the treatment of humeral shaft fractures. [54] (10.1186/s12891-019-2888-2)
- [L4] The combined application of medial anatomical locking plate fixation and minimally invasive lateral locking plate fixation is effective in maintaining operative reduction and preventing varus collapse and implant failure in proximal humerus fractures with an unstable medial column. [56] (10.1186/s13018-020-02094-7)
- [L1] This trial found no significant difference in clinical outcomes at 2 years between surgery and non-operative treatment in patients 60 years of age or older with displaced 2-part fractures of the proximal humerus. [59] (10.1371/journal.pmed.1002855)
- [L5] Treatment for proximal humerus fractures remains controversial, with nonsurgical management demonstrating successful outcomes and union rates greater than 90%. [60] (10.5435/jaaos-d-24-01073)
- [L3] External fixation is a preferred surgical treatment option for paediatric proximal humerus fractures because early mobilization of the affected limb can be realized. [62] (10.1186/s12891-023-07037-x)
- [L2] Short and long periods of immobilization yield similar results for nonoperatively treated proximal humeral fractures, independent of the fracture pattern. [63] (10.2106/jbjs.20.02137)
- [L5] Surgical treatment of proximal humerus fractures remains far from straightforward, with unpredictable outcomes where factors associated with poor results include being a woman, four-part fracture dislocation, and absence of metaphyseal head extension. [64] (10.1097/corr.0000000000002242)
- [L5] The locked plate may prove useful in earlier pain-free rehabilitation of proximal humeral fractures. [66] (10.1016/j.jse.2006.03.013)
- [L4] Ten years after locked plating of displaced proximal humeral fractures, patients show good to excellent outcomes in the majority of cases with no relevant decline compared with the shoulder function 1 year after surgery. [67] (10.1016/j.jse.2013.11.009)
- [L4] Dual plating is still indicated for certain cases, particularly old ununited fractures where intramedullary nailing is difficult, but is contraindicated in severely comminuted fractures requiring extensive dissection. [68] (10.2106/00004623-196345020-00026)
- [L4] Nonsurgical management of proximal humerus fractures decreased during the study period. [69] (10.1016/j.jhsa.2020.03.022)
- [L5] Modern proximal humeral nail designs and techniques have demonstrated promising outcomes and can provide stable fixation. [70] (10.1016/j.jse.2015.11.016)
- [L4] The long PHILOS plate fixation provides reliable secure fixation for the treatment of complex humeral fractures, especially long segment periarticular fractures, segmental fractures involving proximal humerus and shaft, periprosthetic fractures around well-fixed humeral resurfacing prosthesis and pathological fractures. [71] (10.1111/j.1758-5740.2010.00085.x)
- [L3] Nonsurgical treatment should have a more prominent role in the treatment of proximal humeral fractures. [72] (10.1016/j.jse.2011.01.025)
- [L5] Most proximal humeral fractures in elderly patients can be treated nonoperatively with good functional outcomes. [73] (10.2106/jbjs.l.01293)
- [L3] This implies that the inherent nature of medial comminution of proximal humeral fracture may lead to inferior radiographic outcomes. [76] (10.1186/s13018-022-03337-5)
- [L4] The Humerus Block technique is a very good and predictable, minimally invasive, percutaneous operative technique for treatment of various types of proximal humeral fractures that results in very good pain relief, mobility, and pull force in the arm with a low incidence of avascular necrosis. [78] (10.1016/j.jse.2011.07.029)
- [L3] The HGLS classification is a reliable method of describing fractures of the proximal humerus compared with the Neer and AO systems. [79] (10.1016/j.jse.2012.09.018)
- [L3] The most important risk factors for postoperative opioid dependence following proximal humerus fractures are preoperative dependence and fracture complexity. [80] (10.1186/s13018-019-1233-7)
- [L4] With locked plating of unstable proximal humeral fractures, older patients function as well as younger patients; improvement continues until 1 year postoperatively, the Neer fracture classification differentiates function, and polytrauma patients perform worse clinically. [82] (10.1007/s11999-011-1935-6)
- [L1] BMD changes appeared swiftly in the proximal humerus after treatment of displaced 3- or 4-part fractures with ORIF, particularly affecting the proximal diaphysis. [91] (10.1016/j.jse.2022.07.008)
- [L5] Intraoperative 3D imaging with a 160° orbital rotation yields sufficient image quality, enabling the reliable identification of intra-articular screws during plate osteosynthesis of the proximal humerus. [92] (10.1186/s13018-026-06800-9)
- [L4] Acute deep infection after ORIF of proximal humeral fractures is a devastating complication with high complication rates, poor functional outcomes, and a notably high nonunion rate. [93] (10.1016/j.jse.2006.09.021)
- [L1] Fixation of proximal humeral fractures in elderly patients using locked plates with or without cement augmentation has no significant difference in revision rate, but the implant failure and total complication rates may be lesser on using the cement-augmented locked plate for fixation than on using a locked plate alone. [96] (10.1186/s12891-024-07502-1)
- [L4] The overall complication rate of locking plate osteosynthesis for proximal humeral fractures has been decreasing considerably within the last years. [97] (10.1016/j.jse.2016.02.015)
- [L3] The increased in-hospital risk for major adverse events and surgical complications may moderate the enthusiasm associated with RTSA for proximal humeral fractures in patients 65 years and older. [98] (10.1097/corr.0000000000001776)
- [L2] The findings indicate that the risk of short-term complications is highest in patients undergoing surgery for a fracture compared with nonfracture indications. [101] (10.1016/j.jse.2010.11.005)
- [L3] Mortality at 1 year for fragility proximal humerus fractures is universally high regardless of risk factors. [103] (10.1016/j.jse.2022.03.006)
- [L5] Complications are not uncommon, including nonunion, malunion, fracture, and infection. [107] (10.5435/jaaos-d-21-00667)
References
[1] Locking plate fixation of proximal humerus fractures in patients older than 60 years continues to be associated with a high complication rate. Journal of Shoulder and Elbow Surgery. 2020. DOI: 10.1016/j.jse.2019.11.026 [2] What Are the Long-term Outcomes of Locking Plates for Nonosteoporotic Three-part and Four-part Proximal Humeral Fractures With a Minimum 10-year Follow-up Period?. Clinical Orthopaedics & Related Research. 2023. DOI: 10.1097/corr.0000000000002895 [3] Similar Outcomes for Nail versus Plate Fixation of Three-part Proximal Humeral Fractures. Clinical Orthopaedics & Related Research. 2012. DOI: 10.1007/s11999-011-2056-y [4] Complications and Long-Term Outcomes of Open Reduction and Plate Fixation of Proximal Humeral Fractures. Journal of Bone and Joint Surgery. 2019. DOI: 10.2106/jbjs.19.00595 [5] Outcomes after percutaneous reduction and fixation of proximal humeral fractures. Journal of Shoulder and Elbow Surgery. 2007. DOI: 10.1016/j.jse.2006.09.006 [6] Locking intramedullary nails compared with locking plates for two- and three-part proximal humeral surgical neck fractures: a randomized controlled trial. Journal of Shoulder and Elbow Surgery. 2016. DOI: 10.1016/j.jse.2016.02.003 [7] The results of ORIF of displaced unstable proximal humeral fractures using a locking plate. Journal of Shoulder and Elbow Surgery. 2010. DOI: 10.1016/j.jse.2009.08.008 [8] Reverse total shoulder arthroplasty for failed open reduction and internal fixation of fractures of the proximal humerus. Journal of Shoulder and Elbow Surgery. 2017. DOI: 10.1016/j.jse.2016.05.020 [9] Four-part valgus impacted proximal humeral fracture presenting three months after injury in a young patient: Open reduction and internal fixation with triple osteotomy and bone graft augmentation. Journal of Shoulder and Elbow Surgery. 2009. DOI: 10.1016/j.jse.2007.12.012 [10] Outcomes of AO/OTA C-type fractures of the distal humerus after open reduction and internal fixation with locking plate constructs in patients at least 65 years old. BMC Musculoskeletal Disorders. 2022. DOI: 10.1186/s12891-022-05431-5 [11] Quality of life and functional outcome after a 2-part proximal humeral fracture: A prospective cohort study on 50 patients treated with a locking plate. Journal of Shoulder and Elbow Surgery. 2010. DOI: 10.1016/j.jse.2009.11.046 [12] Treatment choice affects inpatient adverse events and mortality in older aged inpatients with an isolated fracture of the proximal humerus. Journal of Shoulder and Elbow Surgery. 2014. DOI: 10.1016/j.jse.2013.09.006 [13] Effect of intramedullary nail and locking plate in the treatment of proximal humerus fracture: an update systematic review and meta-analysis. Journal of Orthopaedic Surgery and Research. 2019. DOI: 10.1186/s13018-019-1345-0 [14] Fracture dislocations of the proximal humerus treated with open reduction and internal fixation: a systematic review. Journal of Shoulder and Elbow Surgery. 2022. DOI: 10.1016/j.jse.2022.04.018 [15] Double plating with autogenous bone grafting as a salvage procedure for recalcitrant humeral shaft nonunion. BMC Musculoskeletal Disorders. 2020. DOI: 10.1186/s12891-020-03743-y [16] Purchase of both proximal and distal fragments by the calcar screw is critical when using a locking plate in the treatment of proximal humeral fractures. The Bone & Joint Journal. 2025. DOI: 10.1302/0301-620x.107b9.bjj-2024-1649.r1 [17] Three- and Four-Part Proximal Humerus Fractures: Open Reduction and Internal Fixation Versus Arthroplasty. The Journal of Hand Surgery. 2010. DOI: 10.1016/j.jhsa.2010.07.019 [18] Intramedullary Fixation for Proximal Humeral Fractures. Journal of the American Academy of Orthopaedic Surgeons. 2020. DOI: 10.5435/jaaos-d-18-00360 [19] A New Locking Plate for Unstable Fractures of the Proximal Humerus. Clinical Orthopaedics & Related Research. 2005. DOI: 10.1097/01.blo.0000137554.91189.a9 [20] Readmissions, revisions, and mortality after treatment for proximal humeral fractures in three large states. BMC Musculoskeletal Disorders. 2019. DOI: 10.1186/s12891-019-2812-9 [21] Elective implant removal in symptomatic patients after internal fixation of proximal humerus fractures improves clinical outcome. BMC Musculoskeletal Disorders. 2016. DOI: 10.1186/s12891-016-0977-z [22] Delays beyond 5 days to surgery does not affect outcome following plate and screw fixation of proximal humerus fractures. Journal of Shoulder and Elbow Surgery. 2025. DOI: 10.1016/j.jse.2025.02.019 [23] Fixed-angle Locked Plating of Two-, Three-, and Four-part Proximal Humerus Fractures. Journal of the American Academy of Orthopaedic Surgeons. 2008. DOI: 10.5435/00124635-200805000-00008 [24] Locking plate fixation for proximal humeral fractures: Initial results with a new implant. Journal of Shoulder and Elbow Surgery. 2007. DOI: 10.1016/j.jse.2006.06.006 [27] Outcomes of open reduction and internal fixation of proximal humerus fracture dislocations. Journal of Shoulder and Elbow Surgery. 2021. DOI: 10.1016/j.jse.2021.01.025 [28] Wound complications after distal humerus fracture fixation: incidence, risk factors, and outcome. Journal of Shoulder and Elbow Surgery. 2014. DOI: 10.1016/j.jse.2013.09.014 [30] The role of greater tuberosity healing in reverse shoulder arthroplasty: a finite element analysis. Journal of Shoulder and Elbow Surgery. 2020. DOI: 10.1016/j.jse.2019.07.022 [31] Does objective shoulder impairment explain patient-reported functional outcome? A study of proximal humerus fractures. Journal of Shoulder and Elbow Surgery. 2011. DOI: 10.1016/j.jse.2010.06.005 [32] Neer Award 2006: Biomechanical assessment of inferior tuberosity placement during hemiarthroplasty for four-part proximal humeral fractures. Journal of Shoulder and Elbow Surgery. 2008. DOI: 10.1016/j.jse.2007.06.017 [33] A scoping review of biomechanical testing for proximal humerus fracture implants. BMC Musculoskeletal Disorders. 2015. DOI: 10.1186/s12891-015-0627-x [34] Mechanical study of the safe distance between humerus shaft fracture and distal locking screws in antegrade nailing. BMC Musculoskeletal Disorders. 2025. DOI: 10.1186/s12891-025-08711-y [35] Finite element analysis of the treatment of a minimally invasive approach combined with a novel anatomical locking plate for scapular body fractures. Journal of Orthopaedic Surgery and Research. 2024. DOI: 10.1186/s13018-024-04905-7 [36] Assessment of fracture stability following modified minimally invasive reduction osteosynthesis system (MIROS) fixation for Neer 2 and 3-Part proximal humeral fractures. BMC Musculoskeletal Disorders. 2025. DOI: 10.1186/s12891-025-08600-4 [38] Postoperative treatment of proximal humerus fractures with an early active motion protocol: a prospective randomized controlled trail. Journal of Shoulder and Elbow Surgery. 2025. DOI: 10.1016/j.jse.2025.01.042 [39] Improvement in shoulder rotation in complex shoulder fractures treated by reverse shoulder arthroplasty. Journal of Shoulder and Elbow Surgery. 2013. DOI: 10.1016/j.jse.2012.03.011 [42] Evaluation of the Constant score: which is the method to assess the objective strength?. BMC Musculoskeletal Disorders. 2019. DOI: 10.1186/s12891-019-2795-6 [44] Does fracture of the dominant shoulder have any effect on functional and quality of life outcome compared with the nondominant shoulder?. Journal of Shoulder and Elbow Surgery. 2015. DOI: 10.1016/j.jse.2014.10.006 [45] Management of clavicle nonunion and malunion. Journal of Shoulder and Elbow Surgery. 2013. DOI: 10.1016/j.jse.2013.01.022 [46] A clinical study on robot navigationassisted intramedullary nail treatment for humeral shaft fractures. BMC Musculoskeletal Disorders. 2024. DOI: 10.1186/s12891-024-07848-6 [47] The assessment of scapular radiographs. The Bone & Joint Journal. 2013. DOI: 10.1302/0301-620x.95b8.30631 [48] Different suture anchor fixation techniques affect contact properties in humeral greater tuberosity fracture: a biomechanical study. BMC Musculoskeletal Disorders. 2019. DOI: 10.1186/s12891-019-2412-8 [49] Altered Glenohumeral Biomechanics in Proximal Humeral Fracture Malunion. Journal of the American Academy of Orthopaedic Surgeons. 2020. DOI: 10.5435/jaaos-d-20-00555 [50] STABILIZATION OF PROXIMAL HUMERAL FRACTURES WITH AN ANGULAR AND SLIDING STABLE ANTEGRADE LOCKING NAIL (TARGON PH). The Journal of Bone and Joint Surgery-American Volume. 2003. DOI: 10.2106/00004623-200300004-00019 [51] Functional outcome following one-part proximal humeral fractures: A prospective study. Journal of Shoulder and Elbow Surgery. 2008. DOI: 10.1016/j.jse.2007.07.016 [52] Early functional improvements using continuous passive motion therapy after angular-stable plate osteosynthesis of proximal humerus fractures – results of a prospective, randomized trial. Journal of Orthopaedic Surgery and Research. 2024. DOI: 10.1186/s13018-024-04804-x [53] Modified minimally invasive approach and intra-osseous portal for three-part proximal humeral fractures: a comparative study. Journal of Orthopaedic Surgery and Research. 2018. DOI: 10.1186/s13018-017-0701-1 [54] Open reduction and internal fixation of humeral midshaft fractures: anterior versus posterior plate fixation. BMC Musculoskeletal Disorders. 2019. DOI: 10.1186/s12891-019-2888-2 [56] A novel surgical approach and technique and short-term clinical efficacy for the treatment of proximal humerus fractures with the combined use of medial anatomical locking plate fixation and minimally invasive lateral locking plate fixation. Journal of Orthopaedic Surgery and Research. 2021. DOI: 10.1186/s13018-020-02094-7 [59] Operative versus non-operative treatment for 2-part proximal humerus fracture: A multicenter randomized controlled trial. PLOS Medicine. 2019. DOI: 10.1371/journal.pmed.1002855 [60] Contemporary Management of Proximal Humeral Fractures. Journal of the American Academy of Orthopaedic Surgeons. 2025. DOI: 10.5435/jaaos-d-24-01073 [62] Kirschner wire versus external fixation in the treatment of proximal humeral fractures in older children and adolescents: a comparative study. BMC Musculoskeletal Disorders. 2023. DOI: 10.1186/s12891-023-07037-x [63] One Versus 3-Week Immobilization Period for Nonoperatively Treated Proximal Humeral Fractures. Journal of Bone and Joint Surgery. 2021. DOI: 10.2106/jbjs.20.02137 [64] CORR Insights®: What Factors Are Associated With Poor Shoulder Function and Serious Complications After Internal Fixation of Three-part and Four-part Proximal Humerus Fracture-dislocations?. Clinical Orthopaedics & Related Research. 2022. DOI: 10.1097/corr.0000000000002242 [66] Biomechanical evaluation of locked plating in proximal humeral fractures. Journal of Shoulder and Elbow Surgery. 2007. DOI: 10.1016/j.jse.2006.03.013 [67] Long-term functional outcomes (median 10 years) after locked plating for displaced fractures of the proximal humerus. Journal of Shoulder and Elbow Surgery. 2014. DOI: 10.1016/j.jse.2013.11.009 [68] DUAL SLOTTED PLATES IN FIXATION OF FRACTURES OF THE FEMORAL SHAFT. The Journal of Bone & Joint Surgery. 1963. DOI: 10.2106/00004623-196345020-00026 [69] Cost-Minimization Analysis and Treatment Trends of Surgical and Nonsurgical Treatment of Proximal Humerus Fractures. The Journal of Hand Surgery. 2020. DOI: 10.1016/j.jhsa.2020.03.022 [70] Intramedullary nailing of the proximal humerus: evolution, technique, and results. Journal of Shoulder and Elbow Surgery. 2016. DOI: 10.1016/j.jse.2015.11.016 [71] Long Philos Plate Fixation for Complex Humeral Fractures. Shoulder & Elbow. 2010. DOI: 10.1111/j.1758-5740.2010.00085.x [72] Locking plate versus nonsurgical treatment for proximal humeral fractures: better midterm outcome with nonsurgical treatment. Journal of Shoulder and Elbow Surgery. 2011. DOI: 10.1016/j.jse.2011.01.025 [73] Proximal Humeral Fracture Treatment in Adults. Journal of Bone and Joint Surgery. 2014. DOI: 10.2106/jbjs.l.01293 [76] The effect of medial calcar support on proximal humeral fractures treated with locking plates. Journal of Orthopaedic Surgery and Research. 2022. DOI: 10.1186/s13018-022-03337-5 [78] Functional and radiographic medium-term outcome evaluation of the Humerus Block, a minimally invasive operative technique for proximal humeral fractures. Journal of Shoulder and Elbow Surgery. 2012. DOI: 10.1016/j.jse.2011.07.029 [79] A comprehensive classification of proximal humeral fractures: HGLS system. Journal of Shoulder and Elbow Surgery. 2013. DOI: 10.1016/j.jse.2012.09.018 [80] Can patient and fracture factors predict opioid dependence following upper extremity fractures?: a retrospective review. Journal of Orthopaedic Surgery and Research. 2019. DOI: 10.1186/s13018-019-1233-7 [82] Locked Plating of Proximal Humeral Fractures: Is Function Affected by Age, Time, and Fracture Patterns?. Clinical Orthopaedics & Related Research. 2011. DOI: 10.1007/s11999-011-1935-6 [91] Osteoporosis does not affect bone mineral density change in the proximal humerus or the functional outcome after open reduction and internal fixation of unilateral displaced 3- or 4-part fractures at 12-month follow-up. Journal of Shoulder and Elbow Surgery. 2023. DOI: 10.1016/j.jse.2022.07.008 [92] Effect of reduced orbital rotation on image quality and intra-articular screw detection in intraoperative 3D imaging of proximal humerus plate fixation: a cadaveric study. Journal of Orthopaedic Surgery and Research. 2026. DOI: 10.1186/s13018-026-06800-9 [93] Acute deep infection after surgical fixation of proximal humeral fractures. Journal of Shoulder and Elbow Surgery. 2007. DOI: 10.1016/j.jse.2006.09.021 [96] Cement-augmented locked plate fixation proximal humerus fractures in elderly patient: a systematic review and meta-analysis. BMC Musculoskeletal Disorders. 2024. DOI: 10.1186/s12891-024-07502-1 [97] Complications of locked plating for proximal humeral fractures—are we getting any better?. Journal of Shoulder and Elbow Surgery. 2016. DOI: 10.1016/j.jse.2016.02.015 [98] In-hospital Complications Are More Likely to Occur After Reverse Shoulder Arthroplasty Than After Locked Plating for Proximal Humeral Fractures. Clinical Orthopaedics & Related Research. 2021. DOI: 10.1097/corr.0000000000001776 [101] Factors predicting complication rates after primary shoulder arthroplasty. Journal of Shoulder and Elbow Surgery. 2011. DOI: 10.1016/j.jse.2010.11.005 [103] Morbidity and mortality of fragility proximal humerus fractures: a retrospective cohort study of patients presenting to a level one trauma center. Journal of Shoulder and Elbow Surgery. 2022. DOI: 10.1016/j.jse.2022.03.006 [107] Shoulder Arthrodesis. Journal of the American Academy of Orthopaedic Surgeons. 2022. DOI: 10.5435/jaaos-d-21-00667





