Understanding Your Scans (X-ray, Ultrasound, MRI, CT) Info In-depth
Last reviewed
Patients › General-Health
What X-rays, ultrasound, MRI and CT each show, and why your surgeon chooses one over another.
When your surgeon orders a scan, it can feel like alphabet soup: X-ray, ultrasound, MRI, CT. Each one is a different tool that shows a different thing, a bit like the difference between a photograph, a video and a 3D model. None of them is simply "better" than the others; the right choice depends entirely on what we need to see. Knowing what each scan is good at takes a lot of the mystery out of the instructions you're given, and helps you understand why we sometimes ask for more than one.
Why different scans? Each one sees something different
The single most useful thing to understand is that every type of scan is suited to a particular kind of tissue. Bone, tendons, ligaments, cartilage and nerves all show up differently, and no single scan shows all of them perfectly. An X-ray is superb for bone but almost blind to a tendon; an ultrasound shows a tendon beautifully but can't see deep inside a joint. So when we pick a scan, we're really asking a question: is the problem in the bone, or in the soft tissues, or both? The answer decides the tool.
That's also why you might have one scan, then be sent for another. It usually doesn't mean anything was wrong with the first one; it means we've narrowed down the question and now need a different kind of picture to answer it.
X-ray — the picture for bone
An X-ray is the quickest and most familiar scan, and it remains the first test for most bone problems. It passes a small amount of radiation through the area and the dense bone shows up clearly white, which makes it excellent for spotting fractures (broken bones), arthritis, the alignment of bones, and dislocations. It's fast, inexpensive and widely available, and the radiation dose is small.
How it actually works. X-rays are made inside a small tube on one side of you: electricity boils electrons off a hot filament and fires them at a metal target, and as they slam to a stop that energy is released as X-rays, a form of very high-energy "light" that, unlike ordinary light, passes straight through soft tissue. (They belong to the same family of radiation as gamma rays, but are produced by these electrons rather than from inside the atom's nucleus.) As the beam crosses your body, dense bone absorbs much more of it than soft tissue or air. A flat detector on the far side records how much got through at each point: where lots of X-rays reach it the picture is black, where few do (behind bone) it is white, and that shadow map is the image.
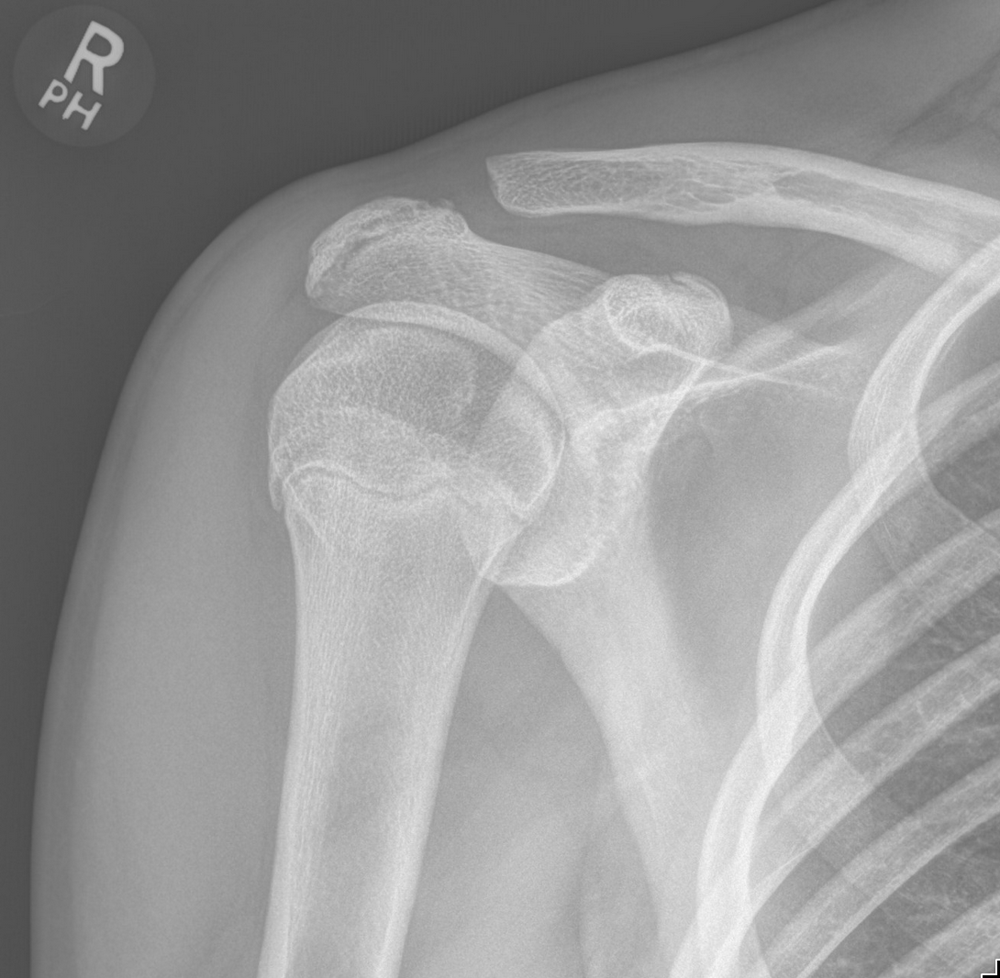
Its limitation is the flip side of its strength: X-rays see bone well but show soft tissues (tendons, ligaments and cartilage) only as vague grey shadows. So a normal X-ray doesn't rule out a soft-tissue injury; it simply tells us the bone looks intact, which is often exactly the reassurance we need first.
Ultrasound — a live view of soft tissues near the surface
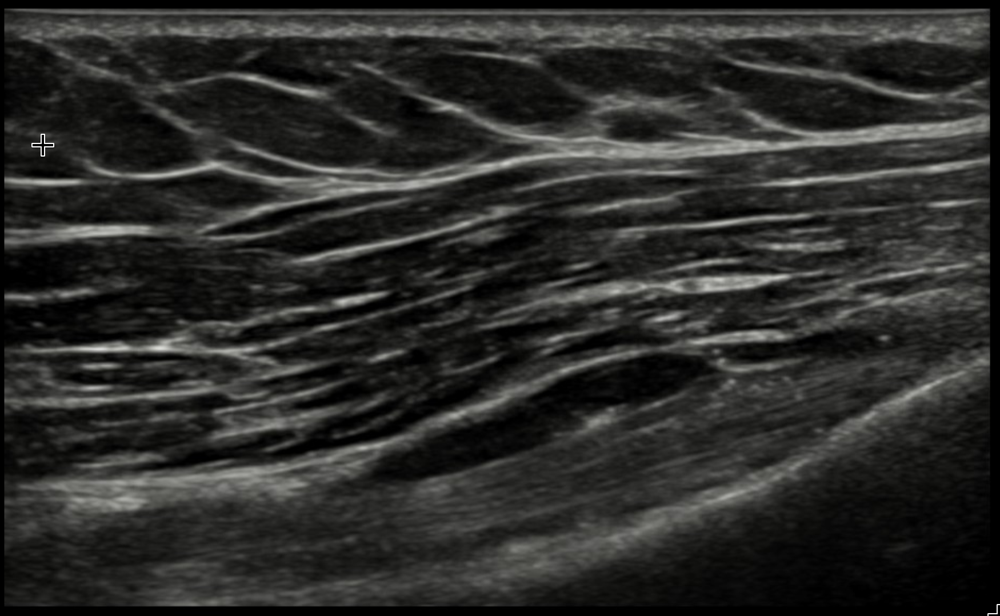
Ultrasound uses high-frequency sound waves rather than radiation, so there's no dose at all. A small probe is moved over the skin with a little gel, and it's particularly good at showing soft tissues that sit fairly close to the surface: tendons, ganglion cysts, pockets of fluid, and inflammation.
How it actually works. The probe contains crystals that buzz when a tiny electric pulse is applied to them (the piezoelectric effect), firing pulses of sound far too high-pitched to hear into the body. Each time a pulse crosses a boundary between two different tissues, part of it echoes back. The probe then switches to "listening" and detects those echoes. The machine measures how long each echo takes to return (which tells it how deep that boundary is) and how strong the echo is (which sets how bright it appears), and assembles thousands of these readings every second into the live picture. Aimed at flowing blood, it can also read the change in pitch of the returning echoes (the Doppler effect) to show, and even measure, blood flow.
Its special trick is that it works in real time. Because we can watch the picture live, we can ask you to move your hand or shoulder and watch a tendon glide as it happens, something a still image can't show. This makes it very useful for tendon problems around the wrist, hand and shoulder. The main thing to know is that ultrasound is operator-dependent: the quality depends on the skill of the person holding the probe, and it can't see deep inside a joint or through bone.
MRI — the detailed all-rounder for soft tissue and bone
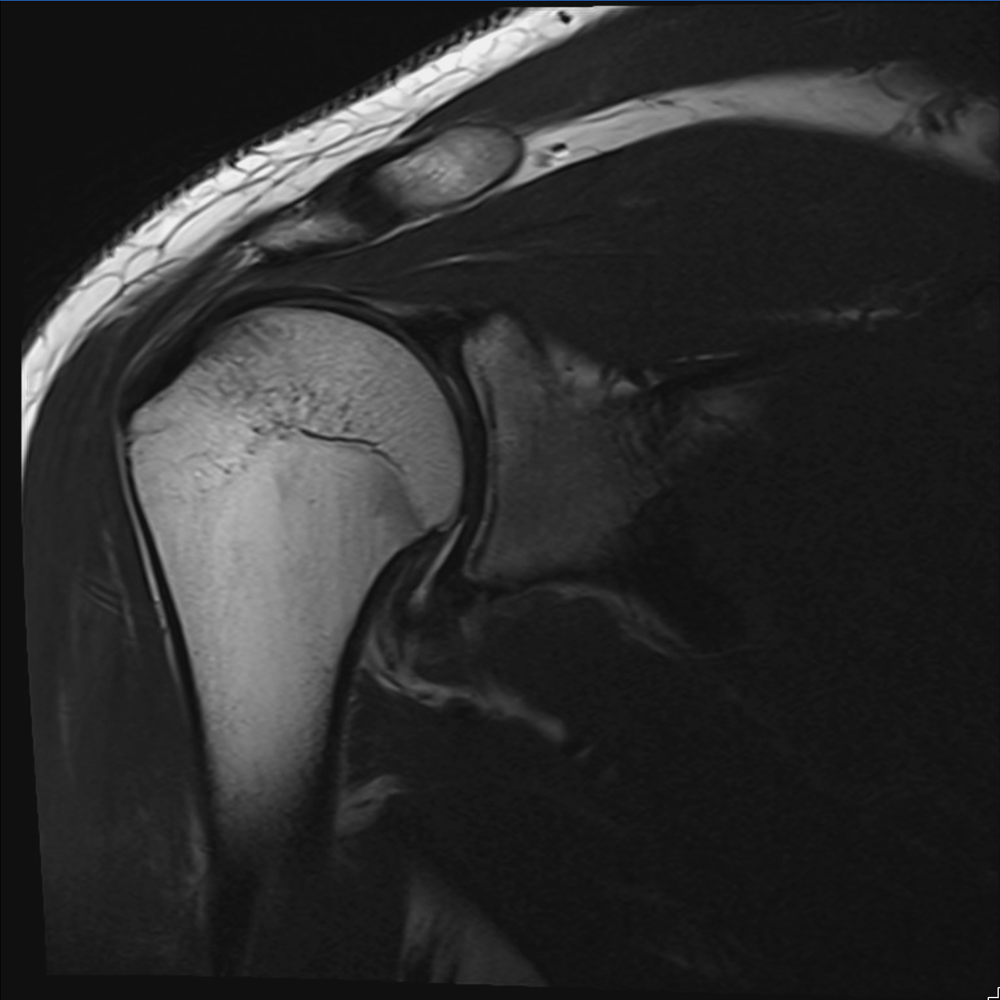
An MRI uses a strong magnet (no radiation) to build remarkably detailed pictures. It is the all-rounder, because it shows both soft tissue and bone in fine detail: ligaments, cartilage, nerves, bone marrow, and even hidden fractures that don't show on a plain X-ray. When we're planning surgery or chasing a problem that the other scans can't quite pin down, MRI is often the deciding test.
How it actually works. Your body is mostly water and fat, which means it is full of hydrogen, and the nucleus of a hydrogen atom is a single proton that spins like a tiny magnet. Normally these point in every direction, but inside the scanner's powerful magnetic field they line up with it and wobble, or precess, at a precise rate set by the field's strength. The scanner then sends in a radio-wave pulse tuned to exactly that rate, which tips the protons out of line and feeds energy into them. When the pulse stops, they relax back into line and hand that energy back as a faint radio signal, which receiver coils pick up. Different tissues release their signal at different speeds, and that is what creates the contrast between, say, cartilage, fluid and bone. Magnetic-field gradients tag where in the body each signal came from, and a piece of mathematics called a Fourier transform turns the mass of collected signals into the detailed image.
A few practical things are worth knowing so it isn't a surprise:
- It takes longer, usually around 20 to 40 minutes, and you need to lie fairly still for clear images.
- You lie inside a tunnel, and the machine is noisy, making knocking and banging sounds while it works. You'll be given earplugs or headphones.
- If you're very claustrophobic, please tell us beforehand; there are ways to make it easier, and sometimes a different machine or a mild sedative can help.
- If you have certain metal implants (such as a pacemaker, or older metalwork), let us know. Many implants such as plates and screws are perfectly safe, but we always check first, so mention anything you have.
CT — 3D detail for complicated bone
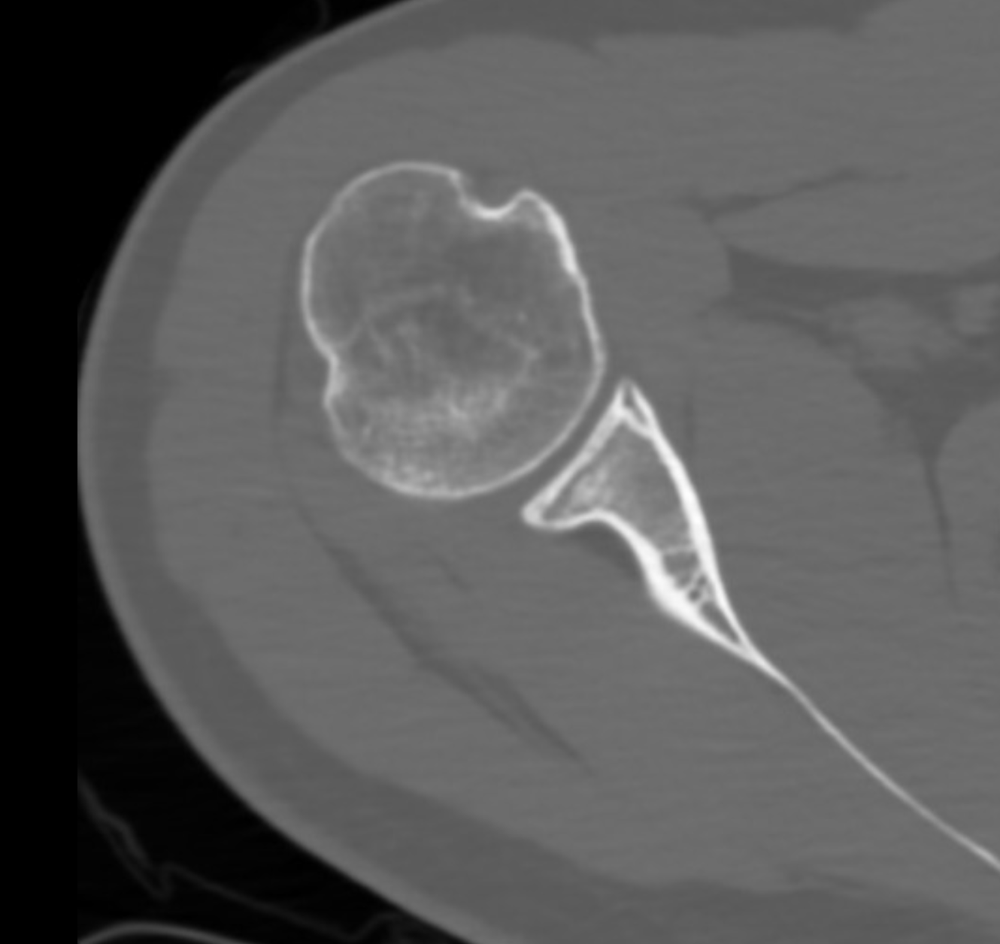
A CT scan takes many X-rays from different angles and a computer builds them into detailed cross-sections, and even a 3D model. Like a plain X-ray it is built around bone, but with far more detail, which makes it superb for complex fractures (where bone is broken into several pieces) and for planning surgery in three dimensions. For tricky breaks around the wrist, elbow or shoulder, a CT can show exactly how the fragments sit so we can plan the repair precisely.
How it actually works. A CT scanner is essentially a spinning X-ray machine: an X-ray tube and a ring of detectors rotate around you while you move slowly through the doughnut-shaped opening, capturing X-ray views from hundreds of angles. On its own each view is just a flat shadow, but a computer combines them all, working out exactly how dense the tissue is at every point, to reconstruct cross-sectional "slices" that can be stacked into a 3D model.
The trade-off is that it uses more radiation than a plain X-ray, so we order it when that extra detail genuinely changes the plan.
A different kind of test — nerve studies
Not every test is a picture. If the concern is a nerve (numbness, tingling or weakness), we may arrange nerve conduction studies or an EMG. Rather than photographing the body, these measure how well the nerves and muscles are actually working, by sending tiny electrical signals along a nerve and recording the response. It answers a different question entirely. You can read more on our nerve tests and conduction studies page.
Putting it together — what to expect
The reassuring bottom line is that the team chooses the scan based on exactly what we need to see, and most scans are quick and painless. An X-ray or ultrasound is often all that's needed; an MRI or CT comes in when we need finer detail or a surgical plan. Whatever you have, the results will be explained to you in plain language, alongside what they mean for your treatment.
If you'd like, these are good questions to ask:
- What is this scan looking for, and which tissue does it show?
- Will I need anything else after it, and roughly how long will it take?
- Is there anything I should mention first: claustrophobia, metal implants, or being pregnant?
- When and how will I get the results explained?
There are no silly questions here. Understanding why a particular scan was chosen often makes the whole process feel a good deal less daunting.
Advanced reading: the deeper science (optional)
This section steps up to a more detailed, student-level explanation. It isn't needed to understand your results, but if you're curious about how each machine actually makes its picture, read on.
X-ray and CT: shadows of density
An X-ray is a beam that passes through the body and is absorbed more by dense tissue (bone) than by soft tissue or air. What reaches the detector is effectively a shadow: bone shows white, air black, soft tissue grey. A CT scan is simply many X-rays taken from all angles and computed into cross-sectional "slices," giving 3D bony detail. Both use ionising radiation (a CT far more than a single X-ray), which is why they're used judiciously.
Ultrasound: listening to echoes
An ultrasound probe sends pulses of very high-frequency sound into the body and listens for the echoes that bounce back off tissue boundaries. A computer turns the timing and strength of those echoes into a live, moving image. It uses no radiation, and because it's real-time it's excellent for soft tissues near the surface and for watching structures move, for example a tendon gliding or a tendon tear opening up as you move.
MRI: spinning hydrogen atoms
An MRI uses a powerful magnet and radio waves to nudge the hydrogen atoms in the body (mostly in water and fat) and then listens to the faint signal they give back as they settle. Different tissues release that signal at different rates, and by timing the measurement the scan can be "weighted" to make different things bright: a T2-weighted scan makes fluid bright, which is why swelling, inflammation and many injuries light up; a T1-weighted scan shows anatomy and fat. The result is exquisite soft-tissue detail (ligaments, cartilage, discs, bone marrow) with no radiation.
Why the choice of scan matters
Each method "sees" something different, so the best scan depends on the question being asked: bone alignment or a fracture (X-ray), a moving tendon near the surface (ultrasound), complicated bony anatomy (CT), or detailed soft tissue and bone marrow (MRI). The right answer often comes from picking the right tool, not from doing every scan.





