Ganglion da bainha dos tendões flexores
Patients › Hand
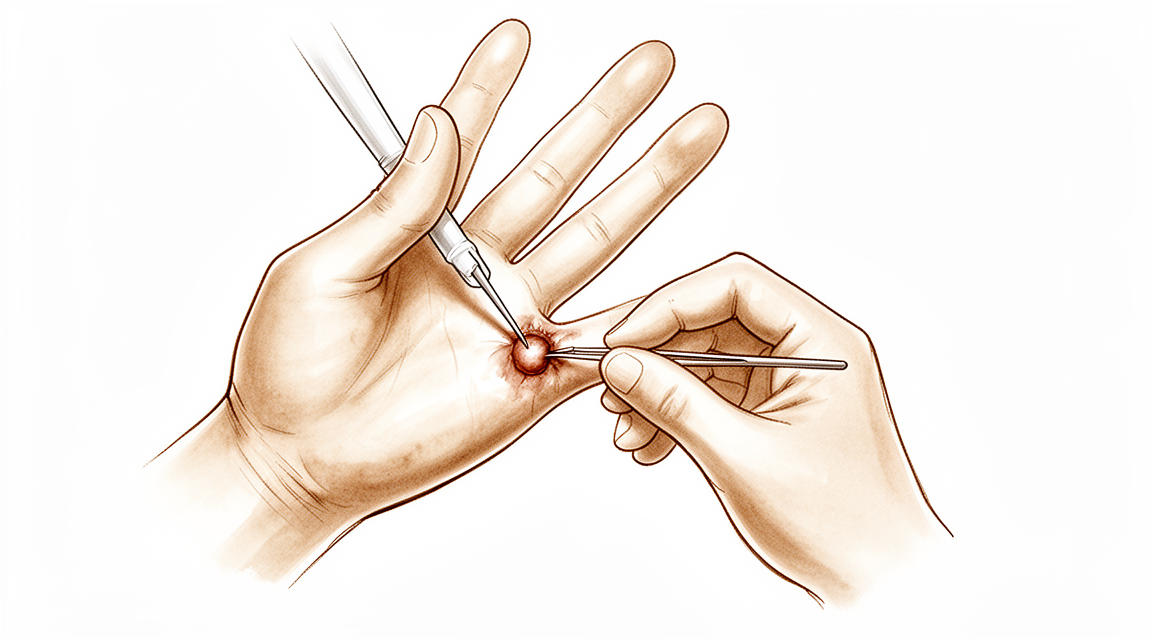
A benign, fluid-filled cyst arising from the flexor tendon sheath – often painless, but can cause clicking or limited finger movement.
O que você está sentindo
Você pode notar um caroço ou inchaço na face palmar do punho ou da mão. Trata-se de um cisto sinovial, que é uma bolsa comum, benigna e preenchida por líquido. Ele se localiza próximo aos tendões que flexionam os dedos. Você pode sentir uma dor sura nessa região. A dor geralmente é intermitente. Tende a piorar após o uso prolongado da mão. Você também pode sentir desconforto ao acordar pela manhã.
À medida que a condição progride, você pode experimentar o gatilho (triggering). Isso ocorre quando o tendão engrossa e prende-se ao se mover através de sua bainha. Seu dedo pode travar em posição flexionada. Você pode precisar usar a outra mão para estendê-lo. Essa sensação de travamento pode ser assustadora e desconfortável. Em alguns casos, o próprio cisto pressiona o tendão no punho, causando problemas semelhantes de travamento nessa região.
As tarefas diárias podem se tornar difíceis. Movimentos simples, como alcançar as costas para fechar um sutiã, podem doer. Enfiar a camisa ou segurar o volante pode parecer rígido e doloroso. Você pode evitar levantar objetos pesados porque isso agrava a área. Dormir do lado da mão afetada pode ser particularmente desconfortável devido à pressão sobre o caroço.
É importante saber que esses sintomas são manejáveis. Seu cirurgião pode ajudá-lo a entender exatamente o que está ocorrendo dentro da sua mão. Embora o espessamento do tendão frequentemente ocorra antes que você sinta o gatilho, a dor e a rigidez são reais e válidas. Você não está imaginando a dificuldade com esses movimentos cotidianos. As opções de tratamento, como a remoção cirúrgica do cisto, são simples e eficazes. Essa abordagem visa aliviar sua dor e restaurar o movimento suave dos seus tendões.
O que está realmente acontecendo
Um cisto ganglionar é uma massa preenchida por líquido que se forma perto dos seus tendões. Neste caso, ele está localizado dentro da bainha que reveste o tendão flexor. Essa bainha é o túnel deslizante que permite que o tendão deslize suavemente quando você dobra os dedos. Pense no tendão como uma corda e na bainha como a manga ao redor dela. O cisto ganglionar é um pequeno balão de líquido que se projeta para dentro dessa manga.
Essa massa pode causar dor e dificultar o movimento do dedo. Pode parecer que o dedo está travando ou engasgando. Seu cirurgião pode remover esse cisto ganglionar com segurança. A excisão cirúrgica é um método simples, seguro e eficaz para tratar um cisto ganglionar doloroso na bainha do tendão flexor digital. O objetivo é aliviar sua dor e restaurar o movimento normal.
Ao tratar um cisto ganglionar que cresce dentro do próprio tendão, seu cirurgião toma cuidados adicionais. O cisto ganglionar pode enfraquecer as fibras do tendão. Portanto, o tratamento deve incluir a preservação do tendão. Seu cirurgião removerá o cisto, mantendo o tendão forte e íntegro. Essa abordagem garante que você possa continuar usando a mão sem fraqueza a longo prazo.
Compreender como essas estruturas funcionam ajuda a explicar seus sintomas. O tendão e seus tecidos circundantes são projetados para um movimento suave e repetitivo. Quando um cisto ganglionar está presente, ele interrompe esse fluxo. Ele cria atrito e pressão dentro do espaço apertado do dedo ou do polegar. É por isso que você sente desconforto ou rigidez. Ao abordar a fonte da irritação, seu cirurgião ajuda sua mão a retornar à sua função natural.
O que podemos fazer a respeito
Você pode começar com o autocuidado e a fisioterapia. Seu cirurgião pode sugerir o uso de talas para repousar a mão e o pulso. Isso ajuda a reduzir a irritação na bainha do tendão. A fisioterapia tem como objetivo manter a articulação se movendo suavemente. Você também pode tentar exercícios suaves para melhorar a força. Essas etapas não cirúrgicas são frequentemente suficientes para controlar os sintomas. Dê uma chance justa a essa abordagem antes de considerar opções mais invasivas.
Se o repouso e a terapia não proporcionarem alívio suficiente, seu cirurgião pode discutir o manejo médico. Medicamentos para dor e anti-inflamatórios podem ajudar a controlar o desconforto. Injeções são outra opção comum. Injeções de cortisona reduzem o inchaço e acalmam a inflamação na bainha. Injeções de ácido hialurônico podem ajudar a lubrificar o espaço articular. Injeções de plasma rico em plaquetas (PRP) usam componentes do próprio sangue para apoiar a cicatrização. Esses tratamentos visam diretamente a dor e a rigidez. O efeito dessas injeções pode variar, mas frequentemente proporcionam alívio significativo por vários meses. Seu cirurgião escolherá o tipo de injeção mais adequado para o seu caso específico. Para a mão em gatilho causada por um cisto sinovial volar do pulso, medidas de radiologia intervencionista podem ser uma opção em vez da cirurgia aberta. Essa técnica minimamente invasiva de agulha-faca demonstrou uma taxa de resultados satisfatórios de 99%, sem lesões nos tendões flexores, artérias ou nervos. Quando as injeções são necessárias, a técnica de injeção médio-axial é a maneira mais precisa de administrar o medicamento na bainha sem arriscar danos ao próprio tendão.
A cirurgia é considerada apenas quando o tratamento conservador atingiu seu limite. Isso significa que você tentou repouso, terapia e injeções sem melhora duradoura. Seu cirurgião discutirá a excisão cirúrgica se o cisto sinovial permanecer doloroso ou limitar seu movimento. Este é um método simples, seguro e eficaz para tratar um cisto sinovial doloroso da bainha do tendão flexor digital. O objetivo é remover o cisto enquanto preserva o tendão. Como os cistos sinoviais podem enfraquecer o tendão, seu cirurgião tomará cuidado para protegê-lo durante o procedimento. A operação em si está detalhada em sua própria página, mas o objetivo principal é aliviar sua dor e restaurar a função normal.
O que esperar
Um cisto ganglion na bainha do tendão flexor do seu dedo é um caroço comum e benigno. Não é câncer e não se espalha. Você pode notar o aparecimento e o desaparecimento do caroço ao longo do tempo. Algumas pessoas o consideram indolor, enquanto outras sentem desconforto ou rigidez.
Se você optar por deixá-lo em repouso, o cisto pode permanecer do mesmo tamanho, encolher ou desaparecer espontaneamente. No entanto, também pode aumentar de tamanho ou tornar-se mais doloroso. Se o cisto comprimir o tendão, pode causar bloqueio (triggering), no qual seu dedo trava ou bloqueia ao dobrá-lo. Essa espessamento do tendão geralmente ocorre antes de você sentir qualquer sensação de bloqueio, exceto no polegar.
A remoção cirúrgica é uma maneira simples, segura e eficaz de tratar um cisto ganglion doloroso. Seu cirurgião removerá o cisto preservando cuidadosamente o tendão. O tendão pode estar enfraquecido pelo cisto, portanto, protegê-lo é uma parte fundamental do procedimento. Muitos pacientes relatam que a remoção do cisto alivia a dor e melhora a função da mão.
A recuperação envolve a cicatrização da pele e a restauração do movimento livre do tendão. Você pode experimentar alguma rigidez no dedo após o procedimento. Isso é normal. Mesmo com tratamento cuidadoso, pode permanecer alguma rigidez residual por um período enquanto os tecidos se acomodam. Seu cirurgião orientará sobre movimentos suaves para manter o dedo flexível sem sobrecarregar a reparação.
A maioria das pessoas retorna às suas atividades diárias normais à medida que o inchaço diminui e a força retorna. O objetivo é ter um dedo sem dor que se mova suavemente. Embora os resultados sejam geralmente bons, os resultados individuais podem variar com base na forma como seu corpo cicatriza. Seu cirurgião discutirá o que é realista para sua situação específica durante a consulta.
Quando procurar um profissional
Procure uma avaliação especializada se notar uma massa na mão ou no pulso. Os cistos sinoviais são lesões benignas comuns que podem se apresentar como essas massas. Procure atendimento se apresentar patologia de gatilho no pulso, pois um cisto sinovial volar do pulso pode se apresentar dessa forma. Consulte seu médico de família se tiver dor persistente que não melhora com o repouso. Procure uma avaliação especializada se sentir fraqueza ou instabilidade. Consulte seu médico se o dedo travar ou ceder. Procure ajuda se os sintomas interferirem no sono ou no trabalho. A piora súbita desses sinais também justifica uma avaliação imediata. O exame clínico é uma ferramenta valiosa para detectar doenças do flexor, portanto, a avaliação profissional é fundamental para obter o diagnóstico e o tratamento adequados.
Evidence & references
Overview
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath [2].
- Treatment of an intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion [3].
Anatomy & Pathophysiology
- The flexor tendon thickens significantly before patients experience triggering, except in the thumb [1].
- The A1 pulley confluence varies on a digit-to-digit basis, with no observed confluence in the thumb and the most common confluence observed in the middle finger [36].
- Hand surface landmarks clarify the localization of the thumb A1 pulley and digital neurovascular structures [28].
- Relative motion between a tendon and subsynovial connective tissue (SSCT) in the carpal tunnel is maximal at extremes of wrist motion, particularly 60° extension, which may predispose the SSCT to shear injury [32].
- The active finger protocol requires the strongest tension of the flexor digitorum profundus tendon and results in the longest excursion [33].
- The relative motion concept harnesses normal functional anatomic relationships of the extensor digitorum communis (EDC) and flexor digitorum profundus (FDP) muscles to vary forces on finger joints, allowing immediate controlled active motion while reducing undesirable tension [29].
- Injury to the extensor mechanism, specifically the central slip, can lead to snapping or catching at the proximal interphalangeal (PIP) joint [35].
- Understanding dynamic and passive stabilizing mechanisms is essential for diagnosing imbalance and for planning reconstructive strategies that restore movement [27].
- Hand surgery and hand therapy practice interventions, including the use of relative motion flexion (RMF) orthoses for management of non-surgical and surgical extensor mechanism (EM) injuries, may benefit from an in-depth look at EM zone III and IV anatomy and biomechanics [26].
Classification
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Adherence around the flexor tendons contributes to the pathology of trigger finger and may be present in all grades of triggering [6].
Clinical Presentation
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Adherence around the flexor tendons contributes to the pathology of trigger finger and may be present in all grades of triggering [6].
- The A0 pulley is implicated as the primary cause of 31% to 47% of trigger fingers [18].
- Ganglion cysts are common benign lesions that may present as masses in the hand and wrist [11].
- A volar wrist ganglion can present with triggering pathology at the wrist [10].
- An intratendinous ganglion in the extensor pollicis longus tendon can cause tenosynovitis [3].
- Clinical examination is a valuable tool for detecting flexor disease due to its high specificity and positive predictive values, although a negative examination does not exclude inflammation [37].
- Tendinopathies involving the hand and wrist are common and often diagnosed easily [9].
- Unilateral absence of the ring finger flexor digitorum profundus musculotendinous structure can pose a diagnostic challenge when history and examination suggest an acute avulsion injury [23].
Investigations
- Sonographic evaluation can assess the flexor tendon, volar plate, and A1 pulley with respect to trigger finger severity [1].
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Adherence around the flexor tendons contributes to trigger finger pathology and may be present in all grades of triggering [6].
Treatment
- Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath [2].
- Ganglion cysts may be managed with reassurance, nonoperative treatment such as aspiration, or surgical excision [11].
- Treatment of an intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion [3].
- A volar wrist ganglion presenting as trigger finger can be treated with interventional radiological measures rather than open surgery [10].
- The minimally invasive needle-knife technique for trigger finger achieved a 99% satisfactory result rate with no injuries to flexor tendons, arteries, or nerves [15].
- Compared to other common non-image guided flexor tendon sheath injection techniques, the mid-axial injection technique was found to be the most accurate in producing all intra-sheath injection and least likely to result in intra-tendinous injection [13].
- Tendinopathies involving the hand and wrist are managed straightforwardly with nonsurgical treatments such as splinting, injection, or therapy, or surgical techniques such as tendon release [9].
Complications
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Adherence around the flexor tendons contributes to the pathology of trigger finger and may be present in all grades of triggering [6].
- The A0 pulley is implicated as the primary cause of 31% to 47% of trigger fingers [18].
- Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath [2].
- Treatment of an intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion [3].
- Ganglion cysts are common benign lesions that may be managed with reassurance, nonoperative treatment such as aspiration, or surgical excision [11].
- A volar wrist ganglion can present as trigger finger [10].
- Even otherwise healthy patients can expect some residual digital stiffness following flexor tendon sheath infection despite aggressive and prompt antibiotic therapy and surgical intervention [7].
- The outcome of a flexor tendon repair is influenced by many factors that cannot be controlled intraoperatively [4].
- Whether or not to repair the flexor digitorum superficialis in acute Zone 2B injuries is an intraoperative decision based on the ease of gliding of the repaired tendon(s) [5].
- Six-strand repair technique is an effective procedure to assure early active motion after flexor pollicis longus tendon injuries, and good results can also be achieved by omitting the circumferential suture [12].
- Minimally invasive needle-knife release achieved a 99% satisfactory result rate with no injuries to flexor tendons, arteries, or nerves [15].
Recovery
- Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath [2].
- Treatment of an intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion [3].
- The outcome of a flexor tendon repair is influenced by many factors that cannot be controlled intraoperatively [4].
- Whether or not to repair the flexor digitorum superficialis in acute Zone 2B injuries is an intraoperative decision based on the ease of gliding of the repaired tendon(s) [5].
- Despite aggressive and prompt antibiotic therapy and surgical intervention, even otherwise healthy patients can expect some residual digital stiffness following flexor tendon sheath infection [7].
- The use of patient-reported outcomes, in addition to clinician-reported outcomes, provided deeper insight into patients' perceptions of their recovery after flexor tendon injury [8].
- A six-strand repair technique is an effective procedure to assure early active motion after flexor pollicis longus tendon injuries [12].
- Good results can be achieved by omitting the circumferential suture in six-strand flexor pollicis longus tendon repairs [12].
- The wide-awake approach to flexor tendon repair has decreased rupture and tenolysis rates and permitted consistently good results in cooperative patients [17].
- The hand requires a stable wrist and at least two sensate digits that can oppose with some power for functional prehension [20].
- A patient with congenital hypoplasia of the extensor tendons of the fingers regained nearly full extension of the affected fingers at 6 months and was able to return to work [25].
Key Evidence
- [L4] The flexor tendon thickened significantly before patients experienced triggering except in the thumb. [1] (10.1016/j.jhsa.2012.06.027)
- [L4] Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath. [2] (10.1007/s11552-007-9028-4)
- [Case_report] Treatment of the intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion. [3] (10.1177/1753193412453428)
- [L4] The outcome of a flexor tendon repair is influenced by many factors that cannot be controlled intraoperatively. [4] (10.1016/j.jhsa.2022.01.015)
- [L3] Whether or not to repair flexor digitorum superficialis is an intraoperative decision based on the ease of gliding of the repaired tendon(s). [5] (10.1177/1753193420932446)
- [L2] Adherence around the flexor tendons contributes to the pathology of trigger finger and may be present in all grades of triggering. [6] (10.1177/1753193420969293)
- [L5] Despite aggressive and prompt antibiotic therapy and surgical intervention, even otherwise healthy patients can expect some residual digital stiffness following flexor tendon sheath infection. [7] (10.5435/jaaos-20-06-373)
- [L3] The use of patient-reported outcomes, in addition to clinician-reported outcomes, provided deeper insight into patients' perceptions of their recovery after flexor tendon injury. [8] (10.1016/j.jht.2024.12.011)
- [L5] Tendinopathies involving the hand and wrist are common, often diagnosed easily, and managed straightforwardly with nonsurgical treatments such as splinting, injection, or therapy, or surgical techniques such as tendon release. [9] (10.5435/jaaos-d-14-00216)
- [L4] This is the first reported case of triggering pathology at the wrist to be treated with interventional radiological measures rather than open surgery and demonstrates the efficacy of the technique. [10] (10.1177/1753193412453699)
- [L5] Ganglion cysts are common benign lesions that may be managed with reassurance, nonoperative treatment such as aspiration, or surgical excision. [11] (10.1016/j.hcl.2004.03.015)
- [L3] Six-strand repair technique is an effective procedure to assure early active motion after flexor pollicis longus tendon injuries and good results can also be achieved by omitting the circumferential suture. [12] (10.1177/15589447211057295)
- [L5] Compared to other common non-image guided flexor tendon sheath injection techniques, the mid-axial injection technique was found to be the most accurate in producing all intra-sheath injection and least likely to result in intra-tendinous injection. [13] (10.1177/15589447221093676)
- [L4] The minimally invasive needle-knife overcomes disadvantages of previously reported knives and achieved a 99% satisfactory result rate with no injuries to flexor tendons, arteries, or nerves. [15] (10.1177/1753193411436294)
- [L5] The wide-awake approach to flexor tendon repair has decreased rupture and tenolysis rates and permitted consistently good results in cooperative patients. [17] (10.1016/j.hcl.2013.02.009)
- [L1] These data implicate the A0 pulley as the primary cause of 31% to 47% of trigger fingers in this study. [18] (10.1177/1558944721994231)
- [L5] The hand requires a stable wrist and at least two sensate digits that can oppose with some power for functional prehension. [20] (10.1016/s0749-0712(02)00130-0)
- [L4] This case illustrates a patient with unilateral absence of the ring finger FDP musculotendinous structure, which can pose a diagnostic challenge when the history and examination suggest an acute avulsion of the ring finger FDP tendon. [23] (10.1016/j.jhsa.2016.02.003)
- [Case_report] The patient regained nearly full extension of the affected fingers at 6 months and was able to return to work. [25] (10.1016/j.jhsa.2019.03.018)
- [L5] Hand surgery and hand therapy practice interventions, including use of RMF orthoses for management of non-surgical and surgical EM injuries may benefit from an in-depth look at the EM zone III and IV anatomy and biomechanics. [26] (10.1016/j.jht.2023.01.002)
- [L5] Understanding the dynamic and passive stabilizing mechanisms is essential for diagnosing imbalance and for planning reconstructive strategies that restore movement. [27] (10.1177/17531934261427638)
- [L5] The findings from our study clarify hand surface landmarks in localizing the thumb A1 pulley and digital neurovascular structures. [28] (10.1016/j.jhsa.2013.02.028)
- [L5] The relative motion concept harnesses normal functional anatomic relationships of the EDC and FDP muscles to vary forces on finger joints, allowing immediate controlled active motion while reducing undesirable tension. [29] (10.1016/j.jht.2022.12.006)
- [L5] Relative motion between a tendon and SSCT in the carpal tunnel is maximal at extremes of wrist motion, particularly 60° extension, which may predispose the SSCT to shear injury. [32] (10.1016/j.jhsa.2008.09.021)
- [L4] The active finger protocol was found to require the strongest tension of the tendon and with the longest excursion. [33] (10.1016/j.jht.2021.01.006)
- [Case_report] Hand surgeons should be aware that injury to the extensor mechanism and specifically the central slip can lead to snapping or catching at the PIP joint in the finger. [35] (10.1177/15589447221081876)
- [L5] A1 pulley confluence varies on a digit-to-digit basis, with no observed confluence in the thumb and the most common confluence observed in the middle finger. [36] (10.1016/j.jhsa.2022.02.011)
- [L3] Clinical examination can be a valuable tool for detecting flexor disease in view of its high specificity and positive predictive values, but a negative clinical examination does not exclude inflammation and an US should be considered. [37] (10.1186/1471-2474-12-91)
References
[1] Sonographic Appearance of the Flexor Tendon, Volar Plate, and A1 Pulley With Respect to the Severity of Trigger Finger. The Journal of Hand Surgery. 2012. DOI: 10.1016/j.jhsa.2012.06.027 [2] Flexor Tendon Sheath Ganglions: Results of Surgical Excision. HAND. 2007. DOI: 10.1007/s11552-007-9028-4 [3] Tenosynovitis of the extensor pollicis longus tendon caused by an intratendinous ganglion: a case report. Journal of Hand Surgery (European Volume). 2012. DOI: 10.1177/1753193412453428 [4] Outcomes of Wide-Awake Flexor Tendon Repairs in 58 Fingers and 9 Thumbs. The Journal of Hand Surgery. 2023. DOI: 10.1016/j.jhsa.2022.01.015 [5] Flexor digitorum profundus with or without flexor digitorum superficialis tendon repair in acute Zone 2B injuries. Journal of Hand Surgery (European Volume). 2020. DOI: 10.1177/1753193420932446 [6] Adhesions as a component of the trigger finger: a dynamic sonographic study. Journal of Hand Surgery (European Volume). 2020. DOI: 10.1177/1753193420969293 [7] Flexor Tendon Sheath Infections of the Hand. Journal of the American Academy of Orthopaedic Surgeons. 2012. DOI: 10.5435/jaaos-20-06-373 [8] Finger flexor tendon injuries repaired surgically followed by an early active motion program: A prospective cohort study of clinician- and patient-reported outcomes. Journal of Hand Therapy. 2026. DOI: 10.1016/j.jht.2024.12.011 [9] Tendinopathies of the Hand and Wrist. Journal of the American Academy of Orthopaedic Surgeons. 2015. DOI: 10.5435/jaaos-d-14-00216 [10] Volar wrist ganglion presenting as trigger finger. Journal of Hand Surgery (European Volume). 2012. DOI: 10.1177/1753193412453699 [11] Ganglion cysts and other tumor related conditions of the hand and wrist. Hand Clinics. 2004. DOI: 10.1016/j.hcl.2004.03.015 [12] Six-Strand Flexor Pollicis Longus Tendon Repairs With and Without Circumferential Sutures: A Multicenter Study. HAND. 2022. DOI: 10.1177/15589447211057295 [13] Accuracy and Safety of Non-Image Guided Trigger Finger Injections: A Cadaveric Study. HAND. 2022. DOI: 10.1177/15589447221093676 [15] A technique for accurately marking the A1 pulley on the skin. Journal of Hand Surgery (European Volume). 2012. DOI: 10.1177/1753193411436294 [17] Wide-awake Flexor Tendon Repair and Early Tendon Mobilization in Zones 1 and 2. Hand Clinics. 2013. DOI: 10.1016/j.hcl.2013.02.009 [18] Differential Pulley Release in Trigger Finger: A Prospective, Randomized Clinical Trial. HAND. 2021. DOI: 10.1177/1558944721994231 [20] Biomechanics and hand trauma: what you need. Hand Clinics. 2003. DOI: 10.1016/s0749-0712(02)00130-0 [23] Absent Ring Finger Flexor Digitorum Profundus Presenting as a Jersey Finger. The Journal of Hand Surgery. 2016. DOI: 10.1016/j.jhsa.2016.02.003 [25] Congenital Hypoplasia of the Extensor Tendons of the Fingers: A Case Report and Review of the Literature. The Journal of Hand Surgery. 2020. DOI: 10.1016/j.jhsa.2019.03.018 [26] An in-depth look at zone III and IV anatomy of the finger extensor mechanism and some clinical implications for use of the relative motion flexion orthosis. Journal of Hand Therapy. 2023. DOI: 10.1016/j.jht.2023.01.002 [27] The balanced finger: biomechanics of intrinsic and extrinsic systems and principles of reconstruction. Journal of Hand Surgery (European Volume). 2026. DOI: 10.1177/17531934261427638 [28] Hand Surface Landmarks and Measurements in the Treatment of Trigger Thumb. The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2013.02.028 [29] A commentary from the pioneers on the innovation of the relative motion concept: History, biologic considerations, and anatomic rationale. Journal of Hand Therapy. 2023. DOI: 10.1016/j.jht.2022.12.006 [32] Shear Strain and Motion of the Subsynovial Connective Tissue and Median Nerve During Single-Digit Motion. The Journal of Hand Surgery. 2009. DOI: 10.1016/j.jhsa.2008.09.021 [33] Ultrasonographic assessment in vivo of the excursion and tension of flexor digitorum profundus tendon on different rehabilitation protocols after tendon repair. Journal of Hand Therapy. 2022. DOI: 10.1016/j.jht.2021.01.006 [35] Longitudinal Tear of the Central Slip Causing Painful and Unusual Snapping of the Finger: A Case Report. HAND. 2022. DOI: 10.1177/15589447221081876 [36] Defining the Digit-Specific Confluence of the A1 Pulley. The Journal of Hand Surgery. 2023. DOI: 10.1016/j.jhsa.2022.02.011 [37] A comparison of ultrasound and clinical examination in the detection of flexor tenosynovitis in early arthritis. BMC Musculoskeletal Disorders. 2011. DOI: 10.1186/1471-2474-12-91





