U nang bao gân gấp
Patients › Hand
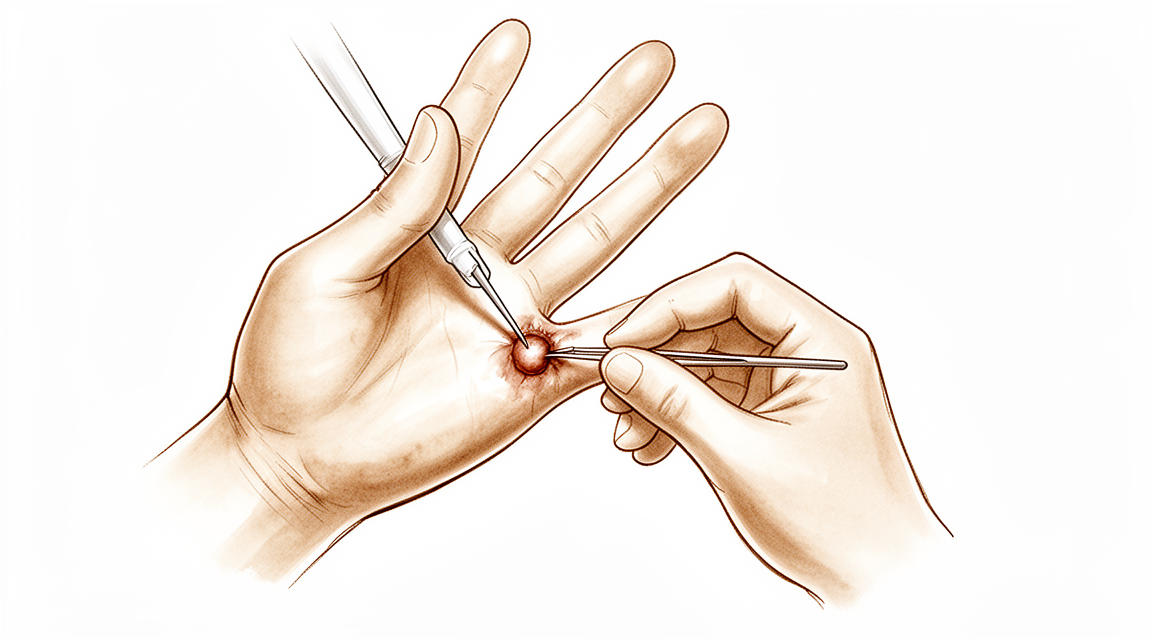
A benign, fluid-filled cyst arising from the flexor tendon sheath – often painless, but can cause clicking or limited finger movement.
Những gì bạn đang cảm nhận
Bạn có thể nhận thấy một khối u hoặc sưng ở mặt lòng cổ tay hoặc bàn tay. Đây là một u nang hoạt dịch, một túi chứa dịch lành tính thường gặp. Nó nằm gần các gân chịu trách nhiệm gập các ngón tay của bạn. Bạn có thể cảm thấy đau âm ỉ ở khu vực này. Cơn đau thường xuất hiện rồi biến mất. Nó có xu hướng bùng phát sau khi bạn sử dụng tay trong thời gian dài. Bạn cũng có thể cảm thấy khó chịu khi vừa thức dậy vào buổi sáng.
Khi tình trạng tiến triển, bạn có thể gặp phải hiện tượng kẹt ngón (triggering). Điều này xảy ra khi gân bị dày lên và bị mắc kẹt khi di chuyển qua bao gân của nó. Ngón tay của bạn có thể bị khóa ở tư thế cong. Bạn có thể cần dùng tay kia để duỗi thẳng nó. Cảm giác kẹt này có thể gây giật mình và khó chịu. Trong một số trường hợp, chính khối u nang chèn ép lên gân tại cổ tay, gây ra các vấn đề khóa tương tự tại đó.
Các hoạt động hàng ngày có thể trở nên khó khăn. Những cử động đơn giản như với tay ra sau lưng để cài áo ngực có thể gây đau. Việc nhét áo vào quần hoặc nắm chặt vô-lăng có thể cảm thấy cứng và đau. Bạn có thể tránh nâng các vật nặng vì điều này làm trầm trọng thêm khu vực bị ảnh hưởng. Ngủ nghiêng về phía bàn tay bị ảnh hưởng có thể đặc biệt khó chịu do áp lực lên khối u.
Điều quan trọng là phải biết rằng các triệu chứng này có thể được kiểm soát. Bác sĩ phẫu thuật của bạn có thể giúp bạn hiểu chính xác những gì đang xảy ra bên trong bàn tay của bạn. Mặc dù sự dày lên của gân thường xảy ra trước khi bạn cảm thấy hiện tượng kẹt ngón, nhưng cơn đau và sự cứng khớp là có thật và hợp lý. Bạn không hề tưởng tượng ra sự khó khăn với những chuyển động hàng ngày này. Các lựa chọn điều trị, chẳng hạn như phẫu thuật cắt bỏ khối u nang, là đơn giản và hiệu quả. Phương pháp này nhằm mục đích giảm đau và khôi phục chuyển động trơn tru cho các gân của bạn.
Những gì thực sự đang xảy ra
U nang (ganglion) là một khối chứa dịch hình thành gần các gân của bạn. Trong trường hợp này, khối u nằm bên trong bao hoạt dịch bao bọc gân gấp. Bao hoạt dịch này là một đường hầm trơn tru cho phép gân của bạn trượt mượt mà khi bạn gập các ngón tay. Hãy tưởng tượng gân giống như một sợi dây thừng và bao hoạt dịch giống như ống bọc bên ngoài nó. U nang là một bong bóng nhỏ chứa dịch phồng lên vào trong ống bọc này.
Khối u này có thể gây đau và khiến việc cử động ngón tay trở nên khó khăn. Bạn có thể cảm thấy ngón tay bị kẹt hoặc khóa cứng. Bác sĩ phẫu thuật của bạn có thể loại bỏ khối u nang này một cách an toàn. Cắt bỏ bằng phẫu thuật là một phương pháp đơn giản, an toàn và hiệu quả để điều trị u nang gây đau ở bao gân gấp ngón tay. Mục tiêu là giảm đau và khôi phục khả năng vận động bình thường.
Khi điều trị một khối u nang phát triển bên trong chính gân, bác sĩ phẫu thuật sẽ thận trọng hơn. Khối u nang có thể làm suy yếu các sợi gân. Do đó, việc điều trị phải bao gồm việc bảo tồn gân. Bác sĩ phẫu thuật sẽ loại bỏ nang trong khi vẫn giữ cho gân chắc khỏe và nguyên vẹn. Phương pháp này đảm bảo bạn có thể tiếp tục sử dụng bàn tay mà không bị suy yếu về lâu dài.
Hiểu cách các cấu trúc này hoạt động giúp giải thích các triệu chứng của bạn. Gân và các mô xung quanh được thiết kế để thực hiện các chuyển động lặp đi lặp lại một cách mượt mà. Khi có u nang, nó làm gián đoạn dòng chảy này. Nó tạo ra ma sát và áp lực trong không gian chật hẹp của ngón tay hoặc ngón cái. Đây là lý do tại sao bạn cảm thấy khó chịu hoặc cứng khớp. Bằng cách giải quyết nguồn gốc gây kích ứng, bác sĩ phẫu thuật giúp bàn tay của bạn trở lại chức năng tự nhiên.
Những gì chúng tôi có thể làm về vấn đề này
Bạn có thể bắt đầu bằng việc tự chăm sóc và vật lý trị liệu. Bác sĩ phẫu thuật của bạn có thể đề xuất nẹp cố định để nghỉ ngơi cho bàn tay và cổ tay. Điều này giúp giảm kích ứng trong bao gân. Vật lý trị liệu nhằm mục đích duy trì cho khớp vận động trơn tru. Bạn cũng có thể thử các bài tập nhẹ nhàng để cải thiện sức mạnh. Những bước không phẫu thuật này thường đủ để kiểm soát các triệu chứng. Hãy dành cho phương pháp này một thử nghiệm công bằng trước khi xem xét các lựa chọn xâm lấn hơn.
Nếu nghỉ ngơi và trị liệu không mang lại đủ sự giảm đau, bác sĩ phẫu thuật của bạn có thể thảo luận về quản lý y tế. Thuốc giảm đau và thuốc chống viêm có thể giúp kiểm soát sự khó chịu. Tiêm là một lựa chọn phổ biến khác. Tiêm cortisone làm giảm sưng và làm dịu viêm trong bao gân. Tiêm axit hyaluronic có thể giúp bôi trơn không gian khớp. Tiêm huyết tương giàu tiểu cầu (PRP) sử dụng các thành phần máu của chính bạn để hỗ trợ chữa lành. Những phương pháp điều trị này nhắm trực tiếp vào cơn đau và cứng khớp. Hiệu quả của những mũi tiêm này có thể khác nhau, nhưng chúng thường mang lại sự giảm đau đáng kể trong vài tháng. Bác sĩ phẫu thuật của bạn sẽ chọn loại tiêm tốt nhất cho trường hợp cụ thể của bạn. Đối với ngón tay cái bập bênh do u nang ganlion lòng bàn tay, các biện pháp can thiệp qua hình ảnh học can thiệp có thể là một lựa chọn thay thế cho phẫu thuật mở. Kỹ thuật dao kim ít xâm lấn này đã cho thấy tỷ lệ kết quả hài lòng 99% mà không gây tổn thương cho các gân gấp, động mạch hoặc dây thần kinh. Khi cần tiêm, kỹ thuật tiêm trục giữa là cách chính xác nhất để đưa thuốc vào bao gân mà không gây nguy hiểm cho chính gân.
Phẫu thuật chỉ được xem xét khi chăm sóc bảo tồn đã đạt đến giới hạn. Điều này có nghĩa là bạn đã thử nghỉ ngơi, trị liệu và tiêm mà không có cải thiện lâu dài. Bác sĩ phẫu thuật của bạn sẽ thảo luận về việc cắt bỏ phẫu thuật nếu u nang ganlion vẫn gây đau hoặc hạn chế chuyển động của bạn. Đây là một phương pháp đơn giản, an toàn và hiệu quả để điều trị u nang ganlion gây đau của bao gân gấp ngón tay. Mục tiêu là loại bỏ u nang trong khi bảo tồn gân. Vì u nang ganlion có thể làm yếu gân, bác sĩ phẫu thuật của bạn sẽ cẩn thận bảo vệ nó trong quá trình phẫu thuật. Phẫu thuật này được mô tả chi tiết trên trang riêng của nó, nhưng mục đích chính là giảm đau và khôi phục chức năng bình thường.
Những điều cần biết
U nang hoạt dịch trong bao gân gấp của ngón tay là một khối u lành tính, thường gặp. Đây không phải là ung thư và sẽ không di căn. Bạn có thể nhận thấy khối u xuất hiện và biến mất theo thời gian. Một số người thấy khối u không gây đau, trong khi những người khác trải qua cảm giác khó chịu hoặc cứng khớp.
Nếu bạn chọn không can thiệp, u nang có thể giữ nguyên kích thước, thu nhỏ hoặc tự biến mất. Tuy nhiên, nó cũng có thể phát triển lớn hơn hoặc trở nên đau đớn hơn. Nếu u nang chèn ép vào gân, nó có thể gây ra hiện tượng kẹt ngón, khiến ngón tay bị mắc kẹt hoặc khóa lại khi bạn gập nó. Sự dày lên của gân thường xảy ra trước khi bạn cảm thấy bất kỳ cảm giác khóa nào, ngoại trừ ở ngón tay cái.
Phẫu thuật cắt bỏ là một phương pháp đơn giản, an toàn và hiệu quả để điều trị u nang hoạt dịch gây đau. Bác sĩ phẫu thuật của bạn sẽ cắt bỏ u nang trong khi bảo tồn cẩn thận gân. Gân có thể bị suy yếu do u nang, vì vậy việc bảo vệ nó là một phần quan trọng của thủ thuật. Nhiều bệnh nhân nhận thấy rằng việc cắt bỏ u nang giúp giảm đau và cải thiện chức năng của bàn tay.
Quá trình hồi phục bao gồm việc làm lành da và cho phép gân cử động tự do trở lại. Bạn có thể trải qua một số cảm giác cứng ở ngón tay sau thủ thuật. Điều này là bình thường. Ngay cả với việc điều trị cẩn thận, một số độ cứng còn sót lại có thể tồn tại trong một thời gian khi các mô ổn định. Bác sĩ phẫu thuật của bạn sẽ hướng dẫn bạn về các chuyển động nhẹ nhàng để giữ cho ngón tay linh hoạt mà không gây căng thẳng cho vết sửa chữa.
Hầu hết mọi người trở lại các hoạt động hàng ngày bình thường khi tình trạng sưng giảm và sức mạnh trở lại. Mục tiêu là có một ngón tay không đau và cử động mượt mà. Trong khi kết quả nói chung là tốt, kết quả cá nhân có thể khác nhau tùy thuộc vào cách cơ thể bạn lành bệnh. Bác sĩ phẫu thuật của bạn sẽ thảo luận về những gì là thực tế cho tình huống cụ thể của bạn trong buổi tư vấn.
Khi nào cần gặp bác sĩ
Yêu cầu đánh giá bởi chuyên gia nếu bạn nhận thấy một khối u ở bàn tay hoặc cổ tay. U nang hoạt dịch là những tổn thương lành tính phổ biến, có thể biểu hiện dưới dạng các khối u này. Hãy tìm kiếm sự chăm sóc y tế nếu bạn gặp phải tình trạng kẹt ngón tại cổ tay, vì u nang hoạt dịch ở mặt lòng cổ tay có thể biểu hiện như vậy. Hãy gặp bác sĩ đa khoa nếu bạn có cơn đau dai dẳng không cải thiện khi nghỉ ngơi. Yêu cầu đánh giá bởi chuyên gia nếu bạn cảm thấy yếu hoặc mất vững. Hãy gặp bác sĩ nếu ngón tay của bạn bị kẹt hoặc đột ngột mất lực. Hãy tìm kiếm sự trợ giúp nếu các triệu chứng ảnh hưởng đến giấc ngủ hoặc công việc. Sự tiến triển nhanh chóng của các dấu hiệu này cũng cần được đánh giá sớm. Khám lâm sàng là một công cụ hữu ích để phát hiện bệnh lý gân gấp, do đó, đánh giá chuyên khoa là yếu tố then chốt để có được chẩn đoán và điều trị đúng đắn.
Evidence & references
Overview
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath [2].
- Treatment of an intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion [3].
Anatomy & Pathophysiology
- The flexor tendon thickens significantly before patients experience triggering, except in the thumb [1].
- The A1 pulley confluence varies on a digit-to-digit basis, with no observed confluence in the thumb and the most common confluence observed in the middle finger [36].
- Hand surface landmarks clarify the localization of the thumb A1 pulley and digital neurovascular structures [28].
- Relative motion between a tendon and subsynovial connective tissue (SSCT) in the carpal tunnel is maximal at extremes of wrist motion, particularly 60° extension, which may predispose the SSCT to shear injury [32].
- The active finger protocol requires the strongest tension of the flexor digitorum profundus tendon and results in the longest excursion [33].
- The relative motion concept harnesses normal functional anatomic relationships of the extensor digitorum communis (EDC) and flexor digitorum profundus (FDP) muscles to vary forces on finger joints, allowing immediate controlled active motion while reducing undesirable tension [29].
- Injury to the extensor mechanism, specifically the central slip, can lead to snapping or catching at the proximal interphalangeal (PIP) joint [35].
- Understanding dynamic and passive stabilizing mechanisms is essential for diagnosing imbalance and for planning reconstructive strategies that restore movement [27].
- Hand surgery and hand therapy practice interventions, including the use of relative motion flexion (RMF) orthoses for management of non-surgical and surgical extensor mechanism (EM) injuries, may benefit from an in-depth look at EM zone III and IV anatomy and biomechanics [26].
Classification
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Adherence around the flexor tendons contributes to the pathology of trigger finger and may be present in all grades of triggering [6].
Clinical Presentation
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Adherence around the flexor tendons contributes to the pathology of trigger finger and may be present in all grades of triggering [6].
- The A0 pulley is implicated as the primary cause of 31% to 47% of trigger fingers [18].
- Ganglion cysts are common benign lesions that may present as masses in the hand and wrist [11].
- A volar wrist ganglion can present with triggering pathology at the wrist [10].
- An intratendinous ganglion in the extensor pollicis longus tendon can cause tenosynovitis [3].
- Clinical examination is a valuable tool for detecting flexor disease due to its high specificity and positive predictive values, although a negative examination does not exclude inflammation [37].
- Tendinopathies involving the hand and wrist are common and often diagnosed easily [9].
- Unilateral absence of the ring finger flexor digitorum profundus musculotendinous structure can pose a diagnostic challenge when history and examination suggest an acute avulsion injury [23].
Investigations
- Sonographic evaluation can assess the flexor tendon, volar plate, and A1 pulley with respect to trigger finger severity [1].
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Adherence around the flexor tendons contributes to trigger finger pathology and may be present in all grades of triggering [6].
Treatment
- Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath [2].
- Ganglion cysts may be managed with reassurance, nonoperative treatment such as aspiration, or surgical excision [11].
- Treatment of an intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion [3].
- A volar wrist ganglion presenting as trigger finger can be treated with interventional radiological measures rather than open surgery [10].
- The minimally invasive needle-knife technique for trigger finger achieved a 99% satisfactory result rate with no injuries to flexor tendons, arteries, or nerves [15].
- Compared to other common non-image guided flexor tendon sheath injection techniques, the mid-axial injection technique was found to be the most accurate in producing all intra-sheath injection and least likely to result in intra-tendinous injection [13].
- Tendinopathies involving the hand and wrist are managed straightforwardly with nonsurgical treatments such as splinting, injection, or therapy, or surgical techniques such as tendon release [9].
Complications
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Adherence around the flexor tendons contributes to the pathology of trigger finger and may be present in all grades of triggering [6].
- The A0 pulley is implicated as the primary cause of 31% to 47% of trigger fingers [18].
- Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath [2].
- Treatment of an intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion [3].
- Ganglion cysts are common benign lesions that may be managed with reassurance, nonoperative treatment such as aspiration, or surgical excision [11].
- A volar wrist ganglion can present as trigger finger [10].
- Even otherwise healthy patients can expect some residual digital stiffness following flexor tendon sheath infection despite aggressive and prompt antibiotic therapy and surgical intervention [7].
- The outcome of a flexor tendon repair is influenced by many factors that cannot be controlled intraoperatively [4].
- Whether or not to repair the flexor digitorum superficialis in acute Zone 2B injuries is an intraoperative decision based on the ease of gliding of the repaired tendon(s) [5].
- Six-strand repair technique is an effective procedure to assure early active motion after flexor pollicis longus tendon injuries, and good results can also be achieved by omitting the circumferential suture [12].
- Minimally invasive needle-knife release achieved a 99% satisfactory result rate with no injuries to flexor tendons, arteries, or nerves [15].
Recovery
- Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath [2].
- Treatment of an intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion [3].
- The outcome of a flexor tendon repair is influenced by many factors that cannot be controlled intraoperatively [4].
- Whether or not to repair the flexor digitorum superficialis in acute Zone 2B injuries is an intraoperative decision based on the ease of gliding of the repaired tendon(s) [5].
- Despite aggressive and prompt antibiotic therapy and surgical intervention, even otherwise healthy patients can expect some residual digital stiffness following flexor tendon sheath infection [7].
- The use of patient-reported outcomes, in addition to clinician-reported outcomes, provided deeper insight into patients' perceptions of their recovery after flexor tendon injury [8].
- A six-strand repair technique is an effective procedure to assure early active motion after flexor pollicis longus tendon injuries [12].
- Good results can be achieved by omitting the circumferential suture in six-strand flexor pollicis longus tendon repairs [12].
- The wide-awake approach to flexor tendon repair has decreased rupture and tenolysis rates and permitted consistently good results in cooperative patients [17].
- The hand requires a stable wrist and at least two sensate digits that can oppose with some power for functional prehension [20].
- A patient with congenital hypoplasia of the extensor tendons of the fingers regained nearly full extension of the affected fingers at 6 months and was able to return to work [25].
Key Evidence
- [L4] The flexor tendon thickened significantly before patients experienced triggering except in the thumb. [1] (10.1016/j.jhsa.2012.06.027)
- [L4] Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath. [2] (10.1007/s11552-007-9028-4)
- [Case_report] Treatment of the intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion. [3] (10.1177/1753193412453428)
- [L4] The outcome of a flexor tendon repair is influenced by many factors that cannot be controlled intraoperatively. [4] (10.1016/j.jhsa.2022.01.015)
- [L3] Whether or not to repair flexor digitorum superficialis is an intraoperative decision based on the ease of gliding of the repaired tendon(s). [5] (10.1177/1753193420932446)
- [L2] Adherence around the flexor tendons contributes to the pathology of trigger finger and may be present in all grades of triggering. [6] (10.1177/1753193420969293)
- [L5] Despite aggressive and prompt antibiotic therapy and surgical intervention, even otherwise healthy patients can expect some residual digital stiffness following flexor tendon sheath infection. [7] (10.5435/jaaos-20-06-373)
- [L3] The use of patient-reported outcomes, in addition to clinician-reported outcomes, provided deeper insight into patients' perceptions of their recovery after flexor tendon injury. [8] (10.1016/j.jht.2024.12.011)
- [L5] Tendinopathies involving the hand and wrist are common, often diagnosed easily, and managed straightforwardly with nonsurgical treatments such as splinting, injection, or therapy, or surgical techniques such as tendon release. [9] (10.5435/jaaos-d-14-00216)
- [L4] This is the first reported case of triggering pathology at the wrist to be treated with interventional radiological measures rather than open surgery and demonstrates the efficacy of the technique. [10] (10.1177/1753193412453699)
- [L5] Ganglion cysts are common benign lesions that may be managed with reassurance, nonoperative treatment such as aspiration, or surgical excision. [11] (10.1016/j.hcl.2004.03.015)
- [L3] Six-strand repair technique is an effective procedure to assure early active motion after flexor pollicis longus tendon injuries and good results can also be achieved by omitting the circumferential suture. [12] (10.1177/15589447211057295)
- [L5] Compared to other common non-image guided flexor tendon sheath injection techniques, the mid-axial injection technique was found to be the most accurate in producing all intra-sheath injection and least likely to result in intra-tendinous injection. [13] (10.1177/15589447221093676)
- [L4] The minimally invasive needle-knife overcomes disadvantages of previously reported knives and achieved a 99% satisfactory result rate with no injuries to flexor tendons, arteries, or nerves. [15] (10.1177/1753193411436294)
- [L5] The wide-awake approach to flexor tendon repair has decreased rupture and tenolysis rates and permitted consistently good results in cooperative patients. [17] (10.1016/j.hcl.2013.02.009)
- [L1] These data implicate the A0 pulley as the primary cause of 31% to 47% of trigger fingers in this study. [18] (10.1177/1558944721994231)
- [L5] The hand requires a stable wrist and at least two sensate digits that can oppose with some power for functional prehension. [20] (10.1016/s0749-0712(02)00130-0)
- [L4] This case illustrates a patient with unilateral absence of the ring finger FDP musculotendinous structure, which can pose a diagnostic challenge when the history and examination suggest an acute avulsion of the ring finger FDP tendon. [23] (10.1016/j.jhsa.2016.02.003)
- [Case_report] The patient regained nearly full extension of the affected fingers at 6 months and was able to return to work. [25] (10.1016/j.jhsa.2019.03.018)
- [L5] Hand surgery and hand therapy practice interventions, including use of RMF orthoses for management of non-surgical and surgical EM injuries may benefit from an in-depth look at the EM zone III and IV anatomy and biomechanics. [26] (10.1016/j.jht.2023.01.002)
- [L5] Understanding the dynamic and passive stabilizing mechanisms is essential for diagnosing imbalance and for planning reconstructive strategies that restore movement. [27] (10.1177/17531934261427638)
- [L5] The findings from our study clarify hand surface landmarks in localizing the thumb A1 pulley and digital neurovascular structures. [28] (10.1016/j.jhsa.2013.02.028)
- [L5] The relative motion concept harnesses normal functional anatomic relationships of the EDC and FDP muscles to vary forces on finger joints, allowing immediate controlled active motion while reducing undesirable tension. [29] (10.1016/j.jht.2022.12.006)
- [L5] Relative motion between a tendon and SSCT in the carpal tunnel is maximal at extremes of wrist motion, particularly 60° extension, which may predispose the SSCT to shear injury. [32] (10.1016/j.jhsa.2008.09.021)
- [L4] The active finger protocol was found to require the strongest tension of the tendon and with the longest excursion. [33] (10.1016/j.jht.2021.01.006)
- [Case_report] Hand surgeons should be aware that injury to the extensor mechanism and specifically the central slip can lead to snapping or catching at the PIP joint in the finger. [35] (10.1177/15589447221081876)
- [L5] A1 pulley confluence varies on a digit-to-digit basis, with no observed confluence in the thumb and the most common confluence observed in the middle finger. [36] (10.1016/j.jhsa.2022.02.011)
- [L3] Clinical examination can be a valuable tool for detecting flexor disease in view of its high specificity and positive predictive values, but a negative clinical examination does not exclude inflammation and an US should be considered. [37] (10.1186/1471-2474-12-91)
References
[1] Sonographic Appearance of the Flexor Tendon, Volar Plate, and A1 Pulley With Respect to the Severity of Trigger Finger. The Journal of Hand Surgery. 2012. DOI: 10.1016/j.jhsa.2012.06.027 [2] Flexor Tendon Sheath Ganglions: Results of Surgical Excision. HAND. 2007. DOI: 10.1007/s11552-007-9028-4 [3] Tenosynovitis of the extensor pollicis longus tendon caused by an intratendinous ganglion: a case report. Journal of Hand Surgery (European Volume). 2012. DOI: 10.1177/1753193412453428 [4] Outcomes of Wide-Awake Flexor Tendon Repairs in 58 Fingers and 9 Thumbs. The Journal of Hand Surgery. 2023. DOI: 10.1016/j.jhsa.2022.01.015 [5] Flexor digitorum profundus with or without flexor digitorum superficialis tendon repair in acute Zone 2B injuries. Journal of Hand Surgery (European Volume). 2020. DOI: 10.1177/1753193420932446 [6] Adhesions as a component of the trigger finger: a dynamic sonographic study. Journal of Hand Surgery (European Volume). 2020. DOI: 10.1177/1753193420969293 [7] Flexor Tendon Sheath Infections of the Hand. Journal of the American Academy of Orthopaedic Surgeons. 2012. DOI: 10.5435/jaaos-20-06-373 [8] Finger flexor tendon injuries repaired surgically followed by an early active motion program: A prospective cohort study of clinician- and patient-reported outcomes. Journal of Hand Therapy. 2026. DOI: 10.1016/j.jht.2024.12.011 [9] Tendinopathies of the Hand and Wrist. Journal of the American Academy of Orthopaedic Surgeons. 2015. DOI: 10.5435/jaaos-d-14-00216 [10] Volar wrist ganglion presenting as trigger finger. Journal of Hand Surgery (European Volume). 2012. DOI: 10.1177/1753193412453699 [11] Ganglion cysts and other tumor related conditions of the hand and wrist. Hand Clinics. 2004. DOI: 10.1016/j.hcl.2004.03.015 [12] Six-Strand Flexor Pollicis Longus Tendon Repairs With and Without Circumferential Sutures: A Multicenter Study. HAND. 2022. DOI: 10.1177/15589447211057295 [13] Accuracy and Safety of Non-Image Guided Trigger Finger Injections: A Cadaveric Study. HAND. 2022. DOI: 10.1177/15589447221093676 [15] A technique for accurately marking the A1 pulley on the skin. Journal of Hand Surgery (European Volume). 2012. DOI: 10.1177/1753193411436294 [17] Wide-awake Flexor Tendon Repair and Early Tendon Mobilization in Zones 1 and 2. Hand Clinics. 2013. DOI: 10.1016/j.hcl.2013.02.009 [18] Differential Pulley Release in Trigger Finger: A Prospective, Randomized Clinical Trial. HAND. 2021. DOI: 10.1177/1558944721994231 [20] Biomechanics and hand trauma: what you need. Hand Clinics. 2003. DOI: 10.1016/s0749-0712(02)00130-0 [23] Absent Ring Finger Flexor Digitorum Profundus Presenting as a Jersey Finger. The Journal of Hand Surgery. 2016. DOI: 10.1016/j.jhsa.2016.02.003 [25] Congenital Hypoplasia of the Extensor Tendons of the Fingers: A Case Report and Review of the Literature. The Journal of Hand Surgery. 2020. DOI: 10.1016/j.jhsa.2019.03.018 [26] An in-depth look at zone III and IV anatomy of the finger extensor mechanism and some clinical implications for use of the relative motion flexion orthosis. Journal of Hand Therapy. 2023. DOI: 10.1016/j.jht.2023.01.002 [27] The balanced finger: biomechanics of intrinsic and extrinsic systems and principles of reconstruction. Journal of Hand Surgery (European Volume). 2026. DOI: 10.1177/17531934261427638 [28] Hand Surface Landmarks and Measurements in the Treatment of Trigger Thumb. The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2013.02.028 [29] A commentary from the pioneers on the innovation of the relative motion concept: History, biologic considerations, and anatomic rationale. Journal of Hand Therapy. 2023. DOI: 10.1016/j.jht.2022.12.006 [32] Shear Strain and Motion of the Subsynovial Connective Tissue and Median Nerve During Single-Digit Motion. The Journal of Hand Surgery. 2009. DOI: 10.1016/j.jhsa.2008.09.021 [33] Ultrasonographic assessment in vivo of the excursion and tension of flexor digitorum profundus tendon on different rehabilitation protocols after tendon repair. Journal of Hand Therapy. 2022. DOI: 10.1016/j.jht.2021.01.006 [35] Longitudinal Tear of the Central Slip Causing Painful and Unusual Snapping of the Finger: A Case Report. HAND. 2022. DOI: 10.1177/15589447221081876 [36] Defining the Digit-Specific Confluence of the A1 Pulley. The Journal of Hand Surgery. 2023. DOI: 10.1016/j.jhsa.2022.02.011 [37] A comparison of ultrasound and clinical examination in the detection of flexor tenosynovitis in early arthritis. BMC Musculoskeletal Disorders. 2011. DOI: 10.1186/1471-2474-12-91





