ஃப்ளெக்சர் டெண்டன் ஷீட் காங்லியன்
Patients › Hand
A benign, fluid-filled cyst arising from the flexor tendon sheath – often painless, but can cause clicking or limited finger movement.
நீங்கள் என்ன உணர்கிறீர்கள்
உங்கள் மணிக்கட்டு அல்லது கையின் உள்ளங்கை பக்கத்தில் ஒரு கட்டி அல்லது வீக்கத்தை நீங்கள் கவனிக்கலாம். இது ஒரு கேங்க்லியன் சிஸ்ட் ஆகும், இது ஒரு பொதுவான, புற்றுநோய் அல்லாத திரவ நிரப்பப்பட்ட பை ஆகும். இது உங்கள் விரல்களை வளைக்கும் தசைகளுக்கு அருகில் அமர்ந்திருக்கிறது. இந்த பகுதியில் ஒரு மந்தமான வலியை நீங்கள் உணரலாம். வலி பெரும்பாலும் வந்து செல்கிறது. நீண்ட நேரம் உங்கள் கையைப் பயன்படுத்திய பிறகு அது எரியும். காலையில் நீங்கள் முதலில் எழுந்தவுடன் நீங்கள் அச om கரியத்தையும் உணரலாம்.
உங்கள் விரல் ஒரு வளைந்த நிலையில் பூட்டப்படலாம். அதை சரிசெய்ய உங்கள் மற்ற கையை நீங்கள் பயன்படுத்த வேண்டியிருக்கும். இந்த பிடிப்பு உணர்வு ஆச்சரியமாகவும் சங்கடமாகவும் இருக்கலாம். சில சந்தர்ப்பங்களில், கணுக்கால் தானே மணிக்கட்டில் உள்ள தசை மீது அழுத்துகிறது, அங்கு இதேபோன்ற பூட்டுதல் சிக்கல்களை ஏற்படுத்துகிறது.
தினசரி பணிகள் கடினமாகிவிடும். உங்கள் முதுகுக்குப் பின்னால் ஒரு பிராவைப் பிணைப்பது போன்ற எளிய இயக்கங்கள் வலிக்கக்கூடும். ஒரு சட்டைக்குள் நுழைவது அல்லது ஒரு ஸ்டீயரிங் வீலைப் பிடிப்பது இறுக்கமாகவும் வேதனையாகவும் உணரலாம். இது பகுதியை மோசமாக்குவதால் கனமான பொருட்களை தூக்குவதைத் தவிர்க்கலாம். உங்கள் பாதிக்கப்பட்ட கையின் பக்கத்தில் தூங்குவது குறிப்பாக கட்டி மீதான அழுத்தத்தின் காரணமாக அச om கரியமாக இருக்கும்.
இந்த அறிகுறிகள் நிர்வகிக்கக்கூடியவை என்பதை அறிவது முக்கியம். உங்கள் அறுவை சிகிச்சையாளர் உங்கள் கையில் என்ன நடக்கிறது என்பதை சரியாகப் புரிந்துகொள்ள உங்களுக்கு உதவ முடியும். இடுப்பு தடிமனாக இருப்பது பெரும்பாலும் நீங்கள் தூண்டுவதை உணருவதற்கு முன்பு நிகழ்கிறது என்றாலும், வலி மற்றும் இறுக்கம் உண்மையானது மற்றும் செல்லுபடியாகும். இந்த அன்றாட இயக்கங்களுடன் நீங்கள் சிரமத்தை கற்பனை செய்யவில்லை. சிகிச்சை விருப்பங்கள், சர்க்கரை நீக்கம் போன்றவை எளிமையானவை மற்றும் பயனுள்ளவை. இந்த அணுகுமுறையானது உங்கள் வலியைக் குறைத்து, உங்கள் இடுப்புகளுக்கு மென்மையான இயக்கத்தை மீட்டெடுப்பதை நோக்கமாகக் கொண்டுள்ளது.
உண்மையில் என்ன நடக்கிறது
ஒரு கங்க்லியன் என்பது உங்கள் தசைகளுக்கு அருகில் உருவாகும் திரவத்தால் நிரப்பப்பட்ட கட்டி. இந்த விஷயத்தில், இது வளைக்கும் தசைகளை உள்ளடக்கிய கவசத்தின் உள்ளே அமர்ந்திருக்கிறது. இந்த கவசம் உங்கள் விரல்களை வளைக்கும்போது உங்கள் தசை மென்மையாக நழுவ அனுமதிக்கும் நெகிழ்வான சுரங்கப்பாதையாகும். தசை ஒரு கயிறு போலவும், அதன் சுற்றியுள்ள ஸ்லீவ் போலவும் சிந்தியுங்கள். கங்க்லியன் இந்த ஸ்லீவ்ஸில் வெடிக்கும் திரவத்தின் ஒரு சிறிய பலூன் ஆகும்.
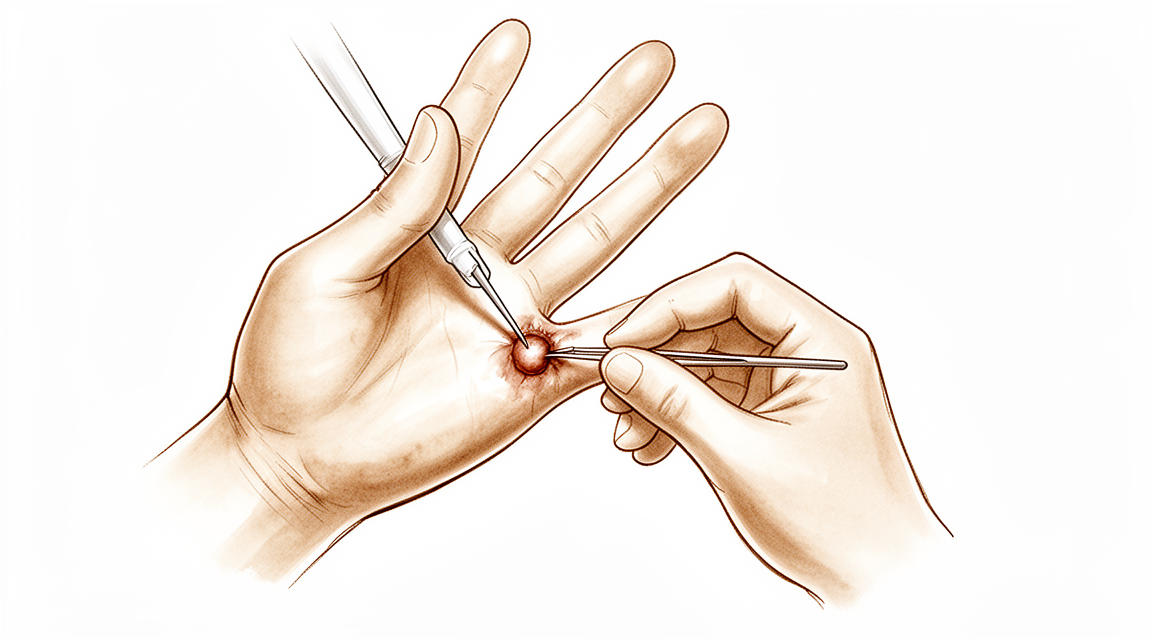
இந்த கட்டி வலியை ஏற்படுத்தலாம் மற்றும் உங்கள் விரலை நகர்த்துவது கடினம். விரல் பிடிப்பது அல்லது பூட்டுவது போல் உணரலாம். உங்கள் அறுவை சிகிச்சை நிபுணர் இந்த கோளத்தை பாதுகாப்பாக அகற்ற முடியும். அறுவை சிகிச்சை வெட்டுதல் என்பது டிஜிட்டல் ஃப்ளெக்ஸர் டெண்டன் ஷீட்டின் வலிமிகுந்த கோளத்தை சிகிச்சையளிப்பதற்கான எளிய, பாதுகாப்பான மற்றும் பயனுள்ள முறையாகும். நோக்கம் உங்கள் வலியைக் குறைத்து இயல்பான இயக்கத்தை மீட்டெடுப்பதாகும்.
இடுப்புக்குள் வளரும் ஒரு கும்பலை சிகிச்சையளிக்கும்போது, உங்கள் அறுவை சிகிச்சை நிபுணர் கூடுதல் கவனம் செலுத்துகிறார். கும்பல் இடுப்பு இழைகளை பலவீனப்படுத்தக்கூடும். எனவே, சிகிச்சையில் இடுப்பைப் பாதுகாப்பது அடங்கும். உங்கள் அறுவை சிகிச்சை நிபுணர் இடுப்பை வலுவாகவும் அப்படியே வைத்திருக்கும்போது சிஸ்டை அகற்றுவார். இந்த அணுகுமுறை உங்கள் கையை நீண்ட கால பலவீனமின்றி தொடர்ந்து பயன்படுத்த முடியும் என்பதை உறுதி செய்கிறது.
இந்த கட்டமைப்புகள் எவ்வாறு செயல்படுகின்றன என்பதைப் புரிந்துகொள்வது உங்கள் அறிகுறிகளை விளக்க உதவுகிறது. இடுப்பு மற்றும் அதைச் சுற்றியுள்ள திசுக்கள் மென்மையான, மீண்டும் மீண்டும் இயக்கத்திற்காக வடிவமைக்கப்பட்டுள்ளன. ஒரு கும்பல் இருக்கும்போது, அது இந்த ஓட்டத்தை சீர்குலைக்கிறது. இது விரல் அல்லது கட்டைவிரலின் இறுக்கமான இடத்திற்குள் உராய்வு மற்றும் அழுத்தத்தை உருவாக்குகிறது. இதனால்தான் நீங்கள் அச om கரியத்தை அல்லது இறுக்கத்தை உணர்கிறீர்கள். எரிச்சலின் மூலத்தை நிவர்த்தி செய்வதன் மூலம், உங்கள் அறுவை சிகிச்சையாளர் உங்கள் கை அதன் இயல்பான செயல்பாட்டிற்கு திரும்ப உதவுகிறது.
நாம் என்ன செய்ய முடியும்
நீங்கள் சுய மேலாண்மை மற்றும் உடலியல் சிகிச்சையுடன் தொடங்கலாம். உங்கள் அறுவை சிகிச்சையாளர் கை மற்றும் மணிக்கட்டில் ஓய்வெடுக்க அடுக்குகளை பரிந்துரைக்கலாம். இது இடுப்பு மூடியில் எரிச்சலைக் குறைக்க உதவுகிறது. உடலியல் சிகிச்சையின் நோக்கம் மூட்டு சீராக நகர்வதைப் பராமரிப்பதாகும். வலிமையை மேம்படுத்த மென்மையான பயிற்சிகளையும் நீங்கள் முயற்சி செய்யலாம். இந்த அறுவை சிகிச்சை அல்லாத படிகள் பெரும்பாலும் அறிகுறிகளை நிர்வகிக்க போதுமானவை. மேலும் ஆக்கிரமிப்பு விருப்பங்களைக் கருத்தில் கொள்வதற்கு முன்பு இந்த அணுகுமுறைக்கு ஒரு நியாயமான சோதனை கொடுங்கள்.
ஓய்வு மற்றும் சிகிச்சை போதுமான நிவாரணத்தை கொண்டு வரவில்லை என்றால், உங்கள் அறுவை சிகிச்சை நிபுணர் மருத்துவ மேலாண்மை பற்றி விவாதிக்கலாம். வலி மருந்துகள் மற்றும் அழற்சி எதிர்ப்பு மருந்துகள் அசௌகரியத்தை கட்டுப்படுத்த உதவும். ஊசிகள் மற்றொரு பொதுவான விருப்பமாகும். கோர்டிசோன் ஊசிகள் வீக்கத்தை குறைத்து மூடியில் அழற்சியை அமைதிப்படுத்தும். ஹைலூரோனிக் அமில ஊசிகள் மூட்டு இடத்தை உயவூட்ட உதவும். பிளேட்லெட் நிறைந்த பிளாஸ்மா (பிஆர்பி) ஊசிகள் குணமடைய உங்கள் சொந்த இரத்தக் கூறுகளைப் பயன்படுத்துகின்றன. இந்த சிகிச்சைகள் வலி மற்றும் இறுக்கத்தை நேரடியாக குறிவைக்கின்றன. இந்த ஊசிகளின் விளைவு மாறுபடலாம், ஆனால் அவை பெரும்பாலும் பல மாதங்களுக்கு கணிசமான நிவாரணத்தை அளிக்கின்றன. உங்கள் அறுவை சிகிச்சை நிபுணர் உங்கள் குறிப்பிட்ட வழக்கிற்கான சிறந்த ஊசி வகையைத் தேர்ந்தெடுவார். விரல் நரம்பு காரணமாக ஏற்படும் விரல் விரல், திறந்த அறுவை சிகி
தற்காப்பு பராமரிப்பு அதன் வரம்பை எட்டியவுடன் மட்டுமே அறுவை சிகிச்சை கருதப்படுகிறது. இதன் பொருள் நீங்கள் ஓய்வு, சிகிச்சை மற்றும் ஊசி மருந்துகளை நீடித்த முன்னேற்றம் இல்லாமல் முயற்சித்திருக்கிறீர்கள். உங்கள் அறுவை சிகிச்சையாளர் கும்பல் வலியுடன் இருந்தால் அல்லது உங்கள் இயக்கத்தை கட்டுப்படுத்துகிறது என்றால் அறுவை சிகிச்சை பிரித்தெடுப்பதைப் பற்றி விவாதிப்பார். இது டிஜிட்டல் ஃப்ளெக்ஸர் தசை மூடியின் வலிமிகுந்த கும்பலை சிகிச்சையளிப்பதற்கான எளிய, பாதுகாப்பான மற்றும் பயனுள்ள முறையாகும். தசை பாதுகாக்கப்படுவதன் மூலம் சிஸ்டை அகற்றுவதே இதன் நோக்கம். கும்பல்கள் தசை பலவீனமடையக்கூடும் என்பதால், உங்கள் அறுவை சிகிச்சையாளர் செயல்பாட்டின் போது அதைப் பாதுகாப்பதில் கவனமாக இருப்பார். அறுவை அதன் சொந்த பக்கத்தில் விரிவாக உள்ளது, ஆனால் முக்கிய நோக்கம் உங்கள் வலியைக் குறைத்து இயல்பான செயல்பாட்டை மீட்டெடுப்பதாகும்.
எதிர்பார்ப்பது என்ன
உங்கள் விரல்களின் நெகிழ் நரம்புப் பட்டைகளில் ஒரு கங்க்லியன் சிஸ்ட் என்பது ஒரு பொதுவான, தீங்கற்ற கட்டி ஆகும். இது புற்றுநோய் அல்ல, பரவாது. காலப்போக்கில் கட்டி தோன்றும் மற்றும் மறைந்துவிடும் என்பதை நீங்கள் கவனிக்கலாம். சிலருக்கு இது வலியற்றதாக இருக்கும், மற்றவர்கள் அச om கரியம் அல்லது கடினத்தன்மையை அனுபவிக்கிறார்கள்.
நீங்கள் அதைத் தனியாக விட்டுவிடத் தேர்வுசெய்தால், கணுக்கால் அதே அளவைக் கொண்டிருக்கலாம், சுருங்கலாம் அல்லது தானாகவே போய்விடலாம். இருப்பினும், அது பெரிதாகவும் அல்லது மிகவும் வேதனையாகவும் மாறக்கூடும். கணுக்கால் தண்டு மீது அழுத்தினால், அது தூண்டுதலுக்கு வழிவகுக்கும், அங்கு உங்கள் விரல் பிடிக்கும் அல்லது நீங்கள் அதை வளைக்கும்போது பூட்டுகிறது. கட்டைவிரலைத் தவிர, எந்தவொரு பூட்டுதல் உணர்வையும் நீங்கள் உணருவதற்கு முன்பு தண்டு தடிமனாகிறது.
அறுவை சிகிச்சை என்பது ஒரு வலிமிகு நரம்பை சிகிச்சையளிப்பதற்கான ஒரு எளிய, பாதுகாப்பான மற்றும் பயனுள்ள வழியாகும். உங்கள் அறுவை சிகிச்சை நிபுணர் நரம்பை கவனமாக பாதுகாக்கும்போது நரம்பை அகற்றுவார். நரம்பு நரம்பால் பலவீனமடையக்கூடும், எனவே அதைப் பாதுகாப்பது இந்த நடைமுறையின் ஒரு முக்கிய பகுதியாகும். நரம்பை அகற்றுவது வலியைக் குறைக்கிறது மற்றும் கை செயல்பாட்டை மேம்படுத்துகிறது என்று பல நோயாளிகள் கண்டறிந்துள்ளனர்.
அறுவை சிகிச்சைக்குப் பிறகு உங்கள் விரலில் சிறிது இறுக்கம் ஏற்படலாம். இது இயல்பானது. கவனமாக சிகிச்சையளித்தாலும், திசுக்கள் குடியேறும்போது சில மீதமுள்ள இறுக்கம் சிறிது நேரம் நீடிக்கும். உங்கள் அறுவை சிகிச்சையாளர் விரலை நெகிழ்வாக வைத்திருக்க மென்மையான இயக்கங்களில் உங்களுக்கு வழிகாட்டுவார்.
பெரும்பாலான மக்கள் தங்கள் வழக்கமான அன்றாட நடவடிக்கைகளுக்குத் திரும்புகிறார்கள். வீக்கம் குறைந்து, வலி மீண்டும் வரும்போது. நோக்கம் ஒரு வலி இல்லாத விரல் மென்மையாக நகரும். முடிவுகள் பொதுவாக நல்லவை என்றாலும், உங்கள் உடல் எவ்வாறு குணமடைகிறது என்பதன் அடிப்படையில் தனிப்பட்ட முடிவுகள் மாறுபடலாம். உங்கள் அறுவை சிகிச்சையாளர் உங்கள் குறிப்பிட்ட சூழ்நிலையில் யதார்த்தமானதை உங்கள் ஆலோசனையின் போது விவாதிப்பார்.
யாரையாவது எப்போது பார்க்க வேண்டும்
உங்கள் கையில் அல்லது மணிக்கட்டில் ஒரு வெகுஜனத்தை நீங்கள் கவனித்தால், ஒரு நிபுணர் மதிப்பாய்வைக் கேளுங்கள். இந்த வெகுஜனங்களாகக் காணக்கூடிய பொதுவான நன்மை பயக்கும் காயங்களாக கங்க்லியன் சிஸ்ட்கள் உள்ளன. மணிக்கட்டில் நோயியல் தூண்டுதலை நீங்கள் அனுபவித்தால், ஒரு வளைந்த மணிக்கட்டு கங்க்லியன் இந்த வழியில் தோன்றலாம். ஓய்வில் முன்னேறாத தொடர்ச்சியான வலி இருந்தால் உங்கள் GP ஐப் பார்க்கவும். நீங்கள் பலவீனம் அல்லது நிலையற்ற தன்மையை உணர்ந்தால் ஒரு நிபுணர் மதிப்பாய்வைக் கேளுங்கள். உங்கள் விரல் பூட்டுகள் அல்லது வழியைக் கொடுத்தால் உங்கள் மருத்துவரைப் பார்க்கவும். அறிகுறிகள் தூக்கம் அல்லது வேலைக்கு இடையூறு விளைவித்தால் உதவியை நாடுங்கள். இந்த அறிகுறிகளின் திடீர் மோசமடைதல் உடனடி மதிப்பீட்டிற்கு உத்தரவாதம் அளிக்கிறது. வளைக்கும் நோயைக் கண்டறிய மருத்துவ பரிசோதனை ஒரு மதிப்புமிக்க கருவியாகும், எனவே சரியான நோயறிதல் மற்றும் சிகிச்சையைப் பெறுவதற்கு தொழில்முறை மதிப்பீடு முக்கியமானது.
Evidence & references
Overview
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath [2].
- Treatment of an intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion [3].
Anatomy & Pathophysiology
- The flexor tendon thickens significantly before patients experience triggering, except in the thumb [1].
- The A1 pulley confluence varies on a digit-to-digit basis, with no observed confluence in the thumb and the most common confluence observed in the middle finger [36].
- Hand surface landmarks clarify the localization of the thumb A1 pulley and digital neurovascular structures [28].
- Relative motion between a tendon and subsynovial connective tissue (SSCT) in the carpal tunnel is maximal at extremes of wrist motion, particularly 60° extension, which may predispose the SSCT to shear injury [32].
- The active finger protocol requires the strongest tension of the flexor digitorum profundus tendon and results in the longest excursion [33].
- The relative motion concept harnesses normal functional anatomic relationships of the extensor digitorum communis (EDC) and flexor digitorum profundus (FDP) muscles to vary forces on finger joints, allowing immediate controlled active motion while reducing undesirable tension [29].
- Injury to the extensor mechanism, specifically the central slip, can lead to snapping or catching at the proximal interphalangeal (PIP) joint [35].
- Understanding dynamic and passive stabilizing mechanisms is essential for diagnosing imbalance and for planning reconstructive strategies that restore movement [27].
- Hand surgery and hand therapy practice interventions, including the use of relative motion flexion (RMF) orthoses for management of non-surgical and surgical extensor mechanism (EM) injuries, may benefit from an in-depth look at EM zone III and IV anatomy and biomechanics [26].
Classification
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Adherence around the flexor tendons contributes to the pathology of trigger finger and may be present in all grades of triggering [6].
Clinical Presentation
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Adherence around the flexor tendons contributes to the pathology of trigger finger and may be present in all grades of triggering [6].
- The A0 pulley is implicated as the primary cause of 31% to 47% of trigger fingers [18].
- Ganglion cysts are common benign lesions that may present as masses in the hand and wrist [11].
- A volar wrist ganglion can present with triggering pathology at the wrist [10].
- An intratendinous ganglion in the extensor pollicis longus tendon can cause tenosynovitis [3].
- Clinical examination is a valuable tool for detecting flexor disease due to its high specificity and positive predictive values, although a negative examination does not exclude inflammation [37].
- Tendinopathies involving the hand and wrist are common and often diagnosed easily [9].
- Unilateral absence of the ring finger flexor digitorum profundus musculotendinous structure can pose a diagnostic challenge when history and examination suggest an acute avulsion injury [23].
Investigations
- Sonographic evaluation can assess the flexor tendon, volar plate, and A1 pulley with respect to trigger finger severity [1].
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Adherence around the flexor tendons contributes to trigger finger pathology and may be present in all grades of triggering [6].
Treatment
- Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath [2].
- Ganglion cysts may be managed with reassurance, nonoperative treatment such as aspiration, or surgical excision [11].
- Treatment of an intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion [3].
- A volar wrist ganglion presenting as trigger finger can be treated with interventional radiological measures rather than open surgery [10].
- The minimally invasive needle-knife technique for trigger finger achieved a 99% satisfactory result rate with no injuries to flexor tendons, arteries, or nerves [15].
- Compared to other common non-image guided flexor tendon sheath injection techniques, the mid-axial injection technique was found to be the most accurate in producing all intra-sheath injection and least likely to result in intra-tendinous injection [13].
- Tendinopathies involving the hand and wrist are managed straightforwardly with nonsurgical treatments such as splinting, injection, or therapy, or surgical techniques such as tendon release [9].
Complications
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Adherence around the flexor tendons contributes to the pathology of trigger finger and may be present in all grades of triggering [6].
- The A0 pulley is implicated as the primary cause of 31% to 47% of trigger fingers [18].
- Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath [2].
- Treatment of an intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion [3].
- Ganglion cysts are common benign lesions that may be managed with reassurance, nonoperative treatment such as aspiration, or surgical excision [11].
- A volar wrist ganglion can present as trigger finger [10].
- Even otherwise healthy patients can expect some residual digital stiffness following flexor tendon sheath infection despite aggressive and prompt antibiotic therapy and surgical intervention [7].
- The outcome of a flexor tendon repair is influenced by many factors that cannot be controlled intraoperatively [4].
- Whether or not to repair the flexor digitorum superficialis in acute Zone 2B injuries is an intraoperative decision based on the ease of gliding of the repaired tendon(s) [5].
- Six-strand repair technique is an effective procedure to assure early active motion after flexor pollicis longus tendon injuries, and good results can also be achieved by omitting the circumferential suture [12].
- Minimally invasive needle-knife release achieved a 99% satisfactory result rate with no injuries to flexor tendons, arteries, or nerves [15].
Recovery
- Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath [2].
- Treatment of an intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion [3].
- The outcome of a flexor tendon repair is influenced by many factors that cannot be controlled intraoperatively [4].
- Whether or not to repair the flexor digitorum superficialis in acute Zone 2B injuries is an intraoperative decision based on the ease of gliding of the repaired tendon(s) [5].
- Despite aggressive and prompt antibiotic therapy and surgical intervention, even otherwise healthy patients can expect some residual digital stiffness following flexor tendon sheath infection [7].
- The use of patient-reported outcomes, in addition to clinician-reported outcomes, provided deeper insight into patients' perceptions of their recovery after flexor tendon injury [8].
- A six-strand repair technique is an effective procedure to assure early active motion after flexor pollicis longus tendon injuries [12].
- Good results can be achieved by omitting the circumferential suture in six-strand flexor pollicis longus tendon repairs [12].
- The wide-awake approach to flexor tendon repair has decreased rupture and tenolysis rates and permitted consistently good results in cooperative patients [17].
- The hand requires a stable wrist and at least two sensate digits that can oppose with some power for functional prehension [20].
- A patient with congenital hypoplasia of the extensor tendons of the fingers regained nearly full extension of the affected fingers at 6 months and was able to return to work [25].
Key Evidence
- [L4] The flexor tendon thickened significantly before patients experienced triggering except in the thumb. [1] (10.1016/j.jhsa.2012.06.027)
- [L4] Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath. [2] (10.1007/s11552-007-9028-4)
- [Case_report] Treatment of the intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion. [3] (10.1177/1753193412453428)
- [L4] The outcome of a flexor tendon repair is influenced by many factors that cannot be controlled intraoperatively. [4] (10.1016/j.jhsa.2022.01.015)
- [L3] Whether or not to repair flexor digitorum superficialis is an intraoperative decision based on the ease of gliding of the repaired tendon(s). [5] (10.1177/1753193420932446)
- [L2] Adherence around the flexor tendons contributes to the pathology of trigger finger and may be present in all grades of triggering. [6] (10.1177/1753193420969293)
- [L5] Despite aggressive and prompt antibiotic therapy and surgical intervention, even otherwise healthy patients can expect some residual digital stiffness following flexor tendon sheath infection. [7] (10.5435/jaaos-20-06-373)
- [L3] The use of patient-reported outcomes, in addition to clinician-reported outcomes, provided deeper insight into patients' perceptions of their recovery after flexor tendon injury. [8] (10.1016/j.jht.2024.12.011)
- [L5] Tendinopathies involving the hand and wrist are common, often diagnosed easily, and managed straightforwardly with nonsurgical treatments such as splinting, injection, or therapy, or surgical techniques such as tendon release. [9] (10.5435/jaaos-d-14-00216)
- [L4] This is the first reported case of triggering pathology at the wrist to be treated with interventional radiological measures rather than open surgery and demonstrates the efficacy of the technique. [10] (10.1177/1753193412453699)
- [L5] Ganglion cysts are common benign lesions that may be managed with reassurance, nonoperative treatment such as aspiration, or surgical excision. [11] (10.1016/j.hcl.2004.03.015)
- [L3] Six-strand repair technique is an effective procedure to assure early active motion after flexor pollicis longus tendon injuries and good results can also be achieved by omitting the circumferential suture. [12] (10.1177/15589447211057295)
- [L5] Compared to other common non-image guided flexor tendon sheath injection techniques, the mid-axial injection technique was found to be the most accurate in producing all intra-sheath injection and least likely to result in intra-tendinous injection. [13] (10.1177/15589447221093676)
- [L4] The minimally invasive needle-knife overcomes disadvantages of previously reported knives and achieved a 99% satisfactory result rate with no injuries to flexor tendons, arteries, or nerves. [15] (10.1177/1753193411436294)
- [L5] The wide-awake approach to flexor tendon repair has decreased rupture and tenolysis rates and permitted consistently good results in cooperative patients. [17] (10.1016/j.hcl.2013.02.009)
- [L1] These data implicate the A0 pulley as the primary cause of 31% to 47% of trigger fingers in this study. [18] (10.1177/1558944721994231)
- [L5] The hand requires a stable wrist and at least two sensate digits that can oppose with some power for functional prehension. [20] (10.1016/s0749-0712(02)00130-0)
- [L4] This case illustrates a patient with unilateral absence of the ring finger FDP musculotendinous structure, which can pose a diagnostic challenge when the history and examination suggest an acute avulsion of the ring finger FDP tendon. [23] (10.1016/j.jhsa.2016.02.003)
- [Case_report] The patient regained nearly full extension of the affected fingers at 6 months and was able to return to work. [25] (10.1016/j.jhsa.2019.03.018)
- [L5] Hand surgery and hand therapy practice interventions, including use of RMF orthoses for management of non-surgical and surgical EM injuries may benefit from an in-depth look at the EM zone III and IV anatomy and biomechanics. [26] (10.1016/j.jht.2023.01.002)
- [L5] Understanding the dynamic and passive stabilizing mechanisms is essential for diagnosing imbalance and for planning reconstructive strategies that restore movement. [27] (10.1177/17531934261427638)
- [L5] The findings from our study clarify hand surface landmarks in localizing the thumb A1 pulley and digital neurovascular structures. [28] (10.1016/j.jhsa.2013.02.028)
- [L5] The relative motion concept harnesses normal functional anatomic relationships of the EDC and FDP muscles to vary forces on finger joints, allowing immediate controlled active motion while reducing undesirable tension. [29] (10.1016/j.jht.2022.12.006)
- [L5] Relative motion between a tendon and SSCT in the carpal tunnel is maximal at extremes of wrist motion, particularly 60° extension, which may predispose the SSCT to shear injury. [32] (10.1016/j.jhsa.2008.09.021)
- [L4] The active finger protocol was found to require the strongest tension of the tendon and with the longest excursion. [33] (10.1016/j.jht.2021.01.006)
- [Case_report] Hand surgeons should be aware that injury to the extensor mechanism and specifically the central slip can lead to snapping or catching at the PIP joint in the finger. [35] (10.1177/15589447221081876)
- [L5] A1 pulley confluence varies on a digit-to-digit basis, with no observed confluence in the thumb and the most common confluence observed in the middle finger. [36] (10.1016/j.jhsa.2022.02.011)
- [L3] Clinical examination can be a valuable tool for detecting flexor disease in view of its high specificity and positive predictive values, but a negative clinical examination does not exclude inflammation and an US should be considered. [37] (10.1186/1471-2474-12-91)
References
[1] Sonographic Appearance of the Flexor Tendon, Volar Plate, and A1 Pulley With Respect to the Severity of Trigger Finger. The Journal of Hand Surgery. 2012. DOI: 10.1016/j.jhsa.2012.06.027 [2] Flexor Tendon Sheath Ganglions: Results of Surgical Excision. HAND. 2007. DOI: 10.1007/s11552-007-9028-4 [3] Tenosynovitis of the extensor pollicis longus tendon caused by an intratendinous ganglion: a case report. Journal of Hand Surgery (European Volume). 2012. DOI: 10.1177/1753193412453428 [4] Outcomes of Wide-Awake Flexor Tendon Repairs in 58 Fingers and 9 Thumbs. The Journal of Hand Surgery. 2023. DOI: 10.1016/j.jhsa.2022.01.015 [5] Flexor digitorum profundus with or without flexor digitorum superficialis tendon repair in acute Zone 2B injuries. Journal of Hand Surgery (European Volume). 2020. DOI: 10.1177/1753193420932446 [6] Adhesions as a component of the trigger finger: a dynamic sonographic study. Journal of Hand Surgery (European Volume). 2020. DOI: 10.1177/1753193420969293 [7] Flexor Tendon Sheath Infections of the Hand. Journal of the American Academy of Orthopaedic Surgeons. 2012. DOI: 10.5435/jaaos-20-06-373 [8] Finger flexor tendon injuries repaired surgically followed by an early active motion program: A prospective cohort study of clinician- and patient-reported outcomes. Journal of Hand Therapy. 2026. DOI: 10.1016/j.jht.2024.12.011 [9] Tendinopathies of the Hand and Wrist. Journal of the American Academy of Orthopaedic Surgeons. 2015. DOI: 10.5435/jaaos-d-14-00216 [10] Volar wrist ganglion presenting as trigger finger. Journal of Hand Surgery (European Volume). 2012. DOI: 10.1177/1753193412453699 [11] Ganglion cysts and other tumor related conditions of the hand and wrist. Hand Clinics. 2004. DOI: 10.1016/j.hcl.2004.03.015 [12] Six-Strand Flexor Pollicis Longus Tendon Repairs With and Without Circumferential Sutures: A Multicenter Study. HAND. 2022. DOI: 10.1177/15589447211057295 [13] Accuracy and Safety of Non-Image Guided Trigger Finger Injections: A Cadaveric Study. HAND. 2022. DOI: 10.1177/15589447221093676 [15] A technique for accurately marking the A1 pulley on the skin. Journal of Hand Surgery (European Volume). 2012. DOI: 10.1177/1753193411436294 [17] Wide-awake Flexor Tendon Repair and Early Tendon Mobilization in Zones 1 and 2. Hand Clinics. 2013. DOI: 10.1016/j.hcl.2013.02.009 [18] Differential Pulley Release in Trigger Finger: A Prospective, Randomized Clinical Trial. HAND. 2021. DOI: 10.1177/1558944721994231 [20] Biomechanics and hand trauma: what you need. Hand Clinics. 2003. DOI: 10.1016/s0749-0712(02)00130-0 [23] Absent Ring Finger Flexor Digitorum Profundus Presenting as a Jersey Finger. The Journal of Hand Surgery. 2016. DOI: 10.1016/j.jhsa.2016.02.003 [25] Congenital Hypoplasia of the Extensor Tendons of the Fingers: A Case Report and Review of the Literature. The Journal of Hand Surgery. 2020. DOI: 10.1016/j.jhsa.2019.03.018 [26] An in-depth look at zone III and IV anatomy of the finger extensor mechanism and some clinical implications for use of the relative motion flexion orthosis. Journal of Hand Therapy. 2023. DOI: 10.1016/j.jht.2023.01.002 [27] The balanced finger: biomechanics of intrinsic and extrinsic systems and principles of reconstruction. Journal of Hand Surgery (European Volume). 2026. DOI: 10.1177/17531934261427638 [28] Hand Surface Landmarks and Measurements in the Treatment of Trigger Thumb. The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2013.02.028 [29] A commentary from the pioneers on the innovation of the relative motion concept: History, biologic considerations, and anatomic rationale. Journal of Hand Therapy. 2023. DOI: 10.1016/j.jht.2022.12.006 [32] Shear Strain and Motion of the Subsynovial Connective Tissue and Median Nerve During Single-Digit Motion. The Journal of Hand Surgery. 2009. DOI: 10.1016/j.jhsa.2008.09.021 [33] Ultrasonographic assessment in vivo of the excursion and tension of flexor digitorum profundus tendon on different rehabilitation protocols after tendon repair. Journal of Hand Therapy. 2022. DOI: 10.1016/j.jht.2021.01.006 [35] Longitudinal Tear of the Central Slip Causing Painful and Unusual Snapping of the Finger: A Case Report. HAND. 2022. DOI: 10.1177/15589447221081876 [36] Defining the Digit-Specific Confluence of the A1 Pulley. The Journal of Hand Surgery. 2023. DOI: 10.1016/j.jhsa.2022.02.011 [37] A comparison of ultrasound and clinical examination in the detection of flexor tenosynovitis in early arthritis. BMC Musculoskeletal Disorders. 2011. DOI: 10.1186/1471-2474-12-91





