屈肌腱鞘腱鞘囊肿
Patients › Hand
A benign, fluid-filled cyst arising from the flexor tendon sheath – often painless, but can cause clicking or limited finger movement.
您的感受
您可能会注意到手腕或手掌侧出现肿块或肿胀。这是一种腱鞘囊肿,是一种常见的、非癌性的充满液体的囊袋。它位于使手指弯曲的肌腱附近。您可能会感到该区域有钝痛。疼痛通常时有时无。长时间使用手部后,疼痛往往会加剧。早晨刚醒来时,您也可能感到不适。
随着病情进展,您可能会出现扳机指现象。这是由于肌腱增厚并在通过腱鞘时发生卡顿所致。您的手指可能会锁定在弯曲位置。您可能需要用另一只手将其伸直。这种卡顿感可能令人震惊且不适。在某些情况下,囊肿本身会在手腕处压迫肌腱,导致类似的锁定问题。
日常活动可能会变得困难。简单的动作,如伸手到背后扣内衣,可能会引起疼痛。塞衬衫或握住方向盘时,可能会感到僵硬和疼痛。您可能会避免提重物,因为这会加重该区域的症状。侧卧在受影响的手一侧睡觉可能会特别不舒服,因为会对肿块产生压力。
重要的是要知道这些症状是可以管理的。您的外科医生可以帮助您准确了解手部内部发生的情况。虽然肌腱增厚通常发生在您感到扳机指之前,但疼痛和僵硬是真实且合理的。您并非在想象这些日常动作中的困难。治疗选项,如手术切除囊肿,简单且有效。这种方法旨在缓解您的疼痛并恢复肌腱的平滑运动。
实际发生了什么
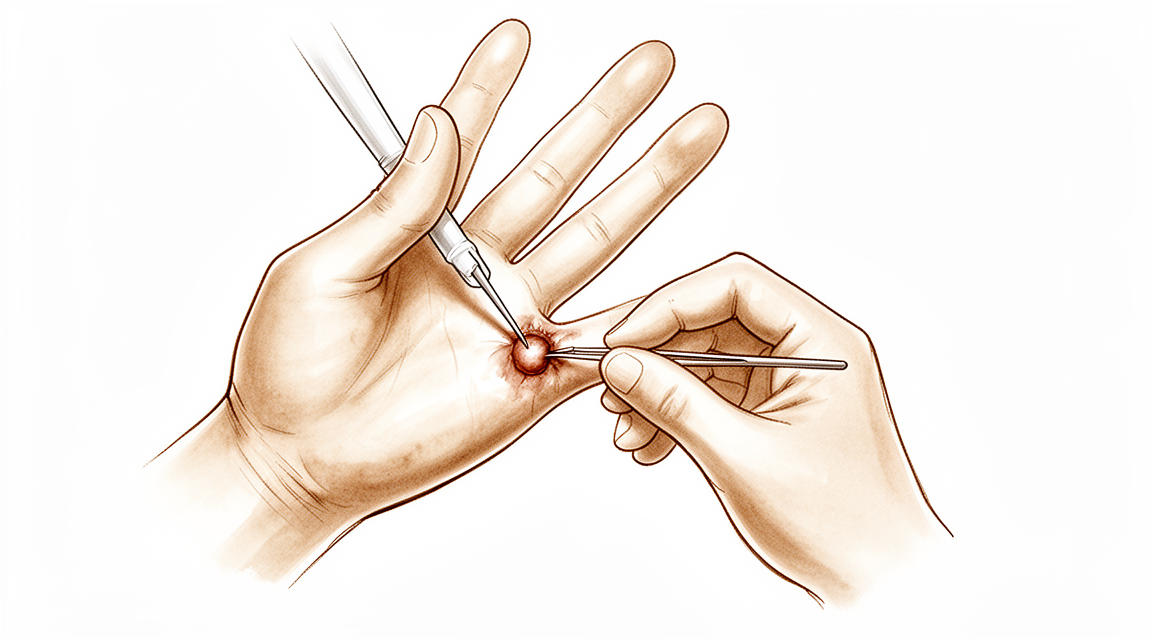
腱鞘囊肿是一种形成于肌腱附近的充满液体的肿块。在本例中,它位于覆盖屈肌腱的腱鞘内部。腱鞘是一个光滑的隧道,使肌腱在屈曲手指时能够顺畅滑动。可以将肌腱想象成一根绳子,而腱鞘则是包裹在绳子外面的套管。腱鞘囊肿就像是一个充满液体的小气球,向这个套管内突出。
这个肿块会引起疼痛,并使手指活动困难。患者可能会感觉手指有卡顿或锁定的现象。您的外科医生可以安全地切除该腱鞘囊肿。手术切除是治疗数字屈肌腱鞘疼痛性腱鞘囊肿的一种简单、安全且有效的方法。其目的是缓解疼痛并恢复正常的活动功能。
当治疗生长在肌腱内部的腱鞘囊肿时,您的外科医生会格外小心。腱鞘囊肿可能会削弱肌腱纤维。因此,治疗必须包括保护肌腱。外科医生将在保持肌腱强壮和完整的同时切除囊肿。这种方法确保您能够继续正常使用手部,而不会出现长期无力。
了解这些结构的工作原理有助于解释您的症状。肌腱及其周围组织是为平滑、重复的运动而设计的。当存在腱鞘囊肿时,它会破坏这种流畅性。它会在手指或拇指的狭小空间内产生摩擦和压力。这就是您感到不适或僵硬的原因。通过解决刺激的根源,您的外科医生帮助您的手部恢复其自然功能。
我们能采取的措施
您可以从自我管理和物理治疗开始。您的外科医生可能会建议佩戴夹板以让手和手腕休息。这有助于减少腱鞘内的刺激。物理治疗旨在保持关节活动顺畅。您可能还会尝试轻柔的锻炼以增强力量。这些非手术步骤通常足以控制症状。在考虑更具侵入性的选项之前,请给这种方法一个公平的尝试。
如果休息和疗法未能带来足够的缓解,您的外科医生可能会讨论药物治疗。止痛药和抗炎药可以帮助控制不适。注射是另一种常见的选择。皮质类固醇注射可减少肿胀并平息腱鞘内的炎症。透明质酸注射可能有助于润滑关节间隙。富血小板血浆(PRP)注射利用您自身的血液成分来支持愈合。这些治疗直接针对疼痛和僵硬。这些注射的效果可能有所不同,但通常能为数月提供显著的缓解。您的外科医生将根据您的具体情况选择最佳的注射类型。对于由掌侧腕腱鞘囊肿引起的扳机指,介入放射学措施可能是一种替代开放手术的选择。这种微创针刀技术已显示出 99% 的满意率,且未损伤屈肌腱、动脉或神经。当需要注射时,中轴注射技术是将药物准确送入腱鞘而不损伤肌腱本身的最准确方法。
仅在保守治疗达到极限时才考虑手术。这意味着您已经尝试了休息、疗法和注射,但未获得持久的改善。如果腱鞘囊肿仍然引起疼痛或限制您的活动,您的外科医生将讨论手术切除。这是治疗数字屈肌腱鞘囊肿引起的疼痛的简单、安全且有效的方法。目标是在保留肌腱的同时移除囊肿。由于腱鞘囊肿可能会削弱肌腱,您的外科医生将在手术过程中小心保护它。手术本身在其单独页面中有详细说明,但主要目的是缓解您的疼痛并恢复功能。
预期情况
手指屈肌腱鞘内的腱鞘囊肿是一种常见的良性肿块。它不是癌症,也不会扩散。您可能会注意到肿块随时间出现和消失。有些人觉得它不痛,而另一些人则会感到不适或僵硬。
如果您选择不予处理,囊肿可能会保持原样、缩小或自行消失。然而,它也可能变大或变得更加疼痛。如果囊肿压迫肌腱,可能会导致扳机指,即您在弯曲手指时手指会卡住或锁定。这种肌腱增厚通常发生在您感觉到任何锁定感之前,拇指除外。
手术切除是治疗疼痛性腱鞘囊肿的一种简单、安全且有效的方法。您的外科医生将在仔细保护肌腱的同时切除囊肿。囊肿可能会削弱肌腱,因此保护肌腱是手术的关键部分。许多患者发现,切除囊肿可以缓解疼痛并改善手部功能。
恢复过程包括皮肤愈合以及让肌腱重新自由活动。术后您可能会感到手指有些僵硬。这是正常的。即使经过精心治疗,随着组织逐渐稳定,仍可能会残留一段时间的僵硬。您的外科医生会指导您进行轻柔的活动,以保持手指灵活,同时避免牵拉修复部位。
随着肿胀消退和力量恢复,大多数人可以恢复正常日常活动。目标是拥有一个无痛且活动顺畅的手指。虽然总体预后良好,但个体结果会根据您身体的愈合情况而有所不同。在咨询期间,您的外科医生会讨论针对您具体情况而言现实可行的预期结果。
何时就诊
如果您发现手部或手腕处有肿块,请寻求专科医生评估。腱鞘囊肿是常见的良性病变,可能表现为此类肿块。如果您出现手腕处的扳机指症状,请及时就医,因为掌侧腕腱鞘囊肿可能表现为这种情况。如果休息后疼痛持续不缓解,请咨询您的全科医生。如果您感到无力或不稳定,请寻求专科医生评估。如果您的手指出现锁定或突然无力,请就医。如果症状影响睡眠或工作,请寻求帮助。这些体征突然加重也需要及时评估。临床检查是检测屈肌疾病的重要工具,因此专业评估对于获得正确的诊断和治疗至关重要。
Evidence & references
Overview
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath [2].
- Treatment of an intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion [3].
Anatomy & Pathophysiology
- The flexor tendon thickens significantly before patients experience triggering, except in the thumb [1].
- The A1 pulley confluence varies on a digit-to-digit basis, with no observed confluence in the thumb and the most common confluence observed in the middle finger [36].
- Hand surface landmarks clarify the localization of the thumb A1 pulley and digital neurovascular structures [28].
- Relative motion between a tendon and subsynovial connective tissue (SSCT) in the carpal tunnel is maximal at extremes of wrist motion, particularly 60° extension, which may predispose the SSCT to shear injury [32].
- The active finger protocol requires the strongest tension of the flexor digitorum profundus tendon and results in the longest excursion [33].
- The relative motion concept harnesses normal functional anatomic relationships of the extensor digitorum communis (EDC) and flexor digitorum profundus (FDP) muscles to vary forces on finger joints, allowing immediate controlled active motion while reducing undesirable tension [29].
- Injury to the extensor mechanism, specifically the central slip, can lead to snapping or catching at the proximal interphalangeal (PIP) joint [35].
- Understanding dynamic and passive stabilizing mechanisms is essential for diagnosing imbalance and for planning reconstructive strategies that restore movement [27].
- Hand surgery and hand therapy practice interventions, including the use of relative motion flexion (RMF) orthoses for management of non-surgical and surgical extensor mechanism (EM) injuries, may benefit from an in-depth look at EM zone III and IV anatomy and biomechanics [26].
Classification
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Adherence around the flexor tendons contributes to the pathology of trigger finger and may be present in all grades of triggering [6].
Clinical Presentation
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Adherence around the flexor tendons contributes to the pathology of trigger finger and may be present in all grades of triggering [6].
- The A0 pulley is implicated as the primary cause of 31% to 47% of trigger fingers [18].
- Ganglion cysts are common benign lesions that may present as masses in the hand and wrist [11].
- A volar wrist ganglion can present with triggering pathology at the wrist [10].
- An intratendinous ganglion in the extensor pollicis longus tendon can cause tenosynovitis [3].
- Clinical examination is a valuable tool for detecting flexor disease due to its high specificity and positive predictive values, although a negative examination does not exclude inflammation [37].
- Tendinopathies involving the hand and wrist are common and often diagnosed easily [9].
- Unilateral absence of the ring finger flexor digitorum profundus musculotendinous structure can pose a diagnostic challenge when history and examination suggest an acute avulsion injury [23].
Investigations
- Sonographic evaluation can assess the flexor tendon, volar plate, and A1 pulley with respect to trigger finger severity [1].
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Adherence around the flexor tendons contributes to trigger finger pathology and may be present in all grades of triggering [6].
Treatment
- Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath [2].
- Ganglion cysts may be managed with reassurance, nonoperative treatment such as aspiration, or surgical excision [11].
- Treatment of an intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion [3].
- A volar wrist ganglion presenting as trigger finger can be treated with interventional radiological measures rather than open surgery [10].
- The minimally invasive needle-knife technique for trigger finger achieved a 99% satisfactory result rate with no injuries to flexor tendons, arteries, or nerves [15].
- Compared to other common non-image guided flexor tendon sheath injection techniques, the mid-axial injection technique was found to be the most accurate in producing all intra-sheath injection and least likely to result in intra-tendinous injection [13].
- Tendinopathies involving the hand and wrist are managed straightforwardly with nonsurgical treatments such as splinting, injection, or therapy, or surgical techniques such as tendon release [9].
Complications
- Flexor tendon thickening occurs significantly before patients experience triggering, except in the thumb [1].
- Adherence around the flexor tendons contributes to the pathology of trigger finger and may be present in all grades of triggering [6].
- The A0 pulley is implicated as the primary cause of 31% to 47% of trigger fingers [18].
- Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath [2].
- Treatment of an intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion [3].
- Ganglion cysts are common benign lesions that may be managed with reassurance, nonoperative treatment such as aspiration, or surgical excision [11].
- A volar wrist ganglion can present as trigger finger [10].
- Even otherwise healthy patients can expect some residual digital stiffness following flexor tendon sheath infection despite aggressive and prompt antibiotic therapy and surgical intervention [7].
- The outcome of a flexor tendon repair is influenced by many factors that cannot be controlled intraoperatively [4].
- Whether or not to repair the flexor digitorum superficialis in acute Zone 2B injuries is an intraoperative decision based on the ease of gliding of the repaired tendon(s) [5].
- Six-strand repair technique is an effective procedure to assure early active motion after flexor pollicis longus tendon injuries, and good results can also be achieved by omitting the circumferential suture [12].
- Minimally invasive needle-knife release achieved a 99% satisfactory result rate with no injuries to flexor tendons, arteries, or nerves [15].
Recovery
- Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath [2].
- Treatment of an intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion [3].
- The outcome of a flexor tendon repair is influenced by many factors that cannot be controlled intraoperatively [4].
- Whether or not to repair the flexor digitorum superficialis in acute Zone 2B injuries is an intraoperative decision based on the ease of gliding of the repaired tendon(s) [5].
- Despite aggressive and prompt antibiotic therapy and surgical intervention, even otherwise healthy patients can expect some residual digital stiffness following flexor tendon sheath infection [7].
- The use of patient-reported outcomes, in addition to clinician-reported outcomes, provided deeper insight into patients' perceptions of their recovery after flexor tendon injury [8].
- A six-strand repair technique is an effective procedure to assure early active motion after flexor pollicis longus tendon injuries [12].
- Good results can be achieved by omitting the circumferential suture in six-strand flexor pollicis longus tendon repairs [12].
- The wide-awake approach to flexor tendon repair has decreased rupture and tenolysis rates and permitted consistently good results in cooperative patients [17].
- The hand requires a stable wrist and at least two sensate digits that can oppose with some power for functional prehension [20].
- A patient with congenital hypoplasia of the extensor tendons of the fingers regained nearly full extension of the affected fingers at 6 months and was able to return to work [25].
Key Evidence
- [L4] The flexor tendon thickened significantly before patients experienced triggering except in the thumb. [1] (10.1016/j.jhsa.2012.06.027)
- [L4] Surgical excision is a simple, safe, and effective method for treating a painful ganglion of the digital flexor tendon sheath. [2] (10.1007/s11552-007-9028-4)
- [Case_report] Treatment of the intratendinous ganglion should include preserving the tendon, which may be weakened by the ganglion. [3] (10.1177/1753193412453428)
- [L4] The outcome of a flexor tendon repair is influenced by many factors that cannot be controlled intraoperatively. [4] (10.1016/j.jhsa.2022.01.015)
- [L3] Whether or not to repair flexor digitorum superficialis is an intraoperative decision based on the ease of gliding of the repaired tendon(s). [5] (10.1177/1753193420932446)
- [L2] Adherence around the flexor tendons contributes to the pathology of trigger finger and may be present in all grades of triggering. [6] (10.1177/1753193420969293)
- [L5] Despite aggressive and prompt antibiotic therapy and surgical intervention, even otherwise healthy patients can expect some residual digital stiffness following flexor tendon sheath infection. [7] (10.5435/jaaos-20-06-373)
- [L3] The use of patient-reported outcomes, in addition to clinician-reported outcomes, provided deeper insight into patients' perceptions of their recovery after flexor tendon injury. [8] (10.1016/j.jht.2024.12.011)
- [L5] Tendinopathies involving the hand and wrist are common, often diagnosed easily, and managed straightforwardly with nonsurgical treatments such as splinting, injection, or therapy, or surgical techniques such as tendon release. [9] (10.5435/jaaos-d-14-00216)
- [L4] This is the first reported case of triggering pathology at the wrist to be treated with interventional radiological measures rather than open surgery and demonstrates the efficacy of the technique. [10] (10.1177/1753193412453699)
- [L5] Ganglion cysts are common benign lesions that may be managed with reassurance, nonoperative treatment such as aspiration, or surgical excision. [11] (10.1016/j.hcl.2004.03.015)
- [L3] Six-strand repair technique is an effective procedure to assure early active motion after flexor pollicis longus tendon injuries and good results can also be achieved by omitting the circumferential suture. [12] (10.1177/15589447211057295)
- [L5] Compared to other common non-image guided flexor tendon sheath injection techniques, the mid-axial injection technique was found to be the most accurate in producing all intra-sheath injection and least likely to result in intra-tendinous injection. [13] (10.1177/15589447221093676)
- [L4] The minimally invasive needle-knife overcomes disadvantages of previously reported knives and achieved a 99% satisfactory result rate with no injuries to flexor tendons, arteries, or nerves. [15] (10.1177/1753193411436294)
- [L5] The wide-awake approach to flexor tendon repair has decreased rupture and tenolysis rates and permitted consistently good results in cooperative patients. [17] (10.1016/j.hcl.2013.02.009)
- [L1] These data implicate the A0 pulley as the primary cause of 31% to 47% of trigger fingers in this study. [18] (10.1177/1558944721994231)
- [L5] The hand requires a stable wrist and at least two sensate digits that can oppose with some power for functional prehension. [20] (10.1016/s0749-0712(02)00130-0)
- [L4] This case illustrates a patient with unilateral absence of the ring finger FDP musculotendinous structure, which can pose a diagnostic challenge when the history and examination suggest an acute avulsion of the ring finger FDP tendon. [23] (10.1016/j.jhsa.2016.02.003)
- [Case_report] The patient regained nearly full extension of the affected fingers at 6 months and was able to return to work. [25] (10.1016/j.jhsa.2019.03.018)
- [L5] Hand surgery and hand therapy practice interventions, including use of RMF orthoses for management of non-surgical and surgical EM injuries may benefit from an in-depth look at the EM zone III and IV anatomy and biomechanics. [26] (10.1016/j.jht.2023.01.002)
- [L5] Understanding the dynamic and passive stabilizing mechanisms is essential for diagnosing imbalance and for planning reconstructive strategies that restore movement. [27] (10.1177/17531934261427638)
- [L5] The findings from our study clarify hand surface landmarks in localizing the thumb A1 pulley and digital neurovascular structures. [28] (10.1016/j.jhsa.2013.02.028)
- [L5] The relative motion concept harnesses normal functional anatomic relationships of the EDC and FDP muscles to vary forces on finger joints, allowing immediate controlled active motion while reducing undesirable tension. [29] (10.1016/j.jht.2022.12.006)
- [L5] Relative motion between a tendon and SSCT in the carpal tunnel is maximal at extremes of wrist motion, particularly 60° extension, which may predispose the SSCT to shear injury. [32] (10.1016/j.jhsa.2008.09.021)
- [L4] The active finger protocol was found to require the strongest tension of the tendon and with the longest excursion. [33] (10.1016/j.jht.2021.01.006)
- [Case_report] Hand surgeons should be aware that injury to the extensor mechanism and specifically the central slip can lead to snapping or catching at the PIP joint in the finger. [35] (10.1177/15589447221081876)
- [L5] A1 pulley confluence varies on a digit-to-digit basis, with no observed confluence in the thumb and the most common confluence observed in the middle finger. [36] (10.1016/j.jhsa.2022.02.011)
- [L3] Clinical examination can be a valuable tool for detecting flexor disease in view of its high specificity and positive predictive values, but a negative clinical examination does not exclude inflammation and an US should be considered. [37] (10.1186/1471-2474-12-91)
References
[1] Sonographic Appearance of the Flexor Tendon, Volar Plate, and A1 Pulley With Respect to the Severity of Trigger Finger. The Journal of Hand Surgery. 2012. DOI: 10.1016/j.jhsa.2012.06.027 [2] Flexor Tendon Sheath Ganglions: Results of Surgical Excision. HAND. 2007. DOI: 10.1007/s11552-007-9028-4 [3] Tenosynovitis of the extensor pollicis longus tendon caused by an intratendinous ganglion: a case report. Journal of Hand Surgery (European Volume). 2012. DOI: 10.1177/1753193412453428 [4] Outcomes of Wide-Awake Flexor Tendon Repairs in 58 Fingers and 9 Thumbs. The Journal of Hand Surgery. 2023. DOI: 10.1016/j.jhsa.2022.01.015 [5] Flexor digitorum profundus with or without flexor digitorum superficialis tendon repair in acute Zone 2B injuries. Journal of Hand Surgery (European Volume). 2020. DOI: 10.1177/1753193420932446 [6] Adhesions as a component of the trigger finger: a dynamic sonographic study. Journal of Hand Surgery (European Volume). 2020. DOI: 10.1177/1753193420969293 [7] Flexor Tendon Sheath Infections of the Hand. Journal of the American Academy of Orthopaedic Surgeons. 2012. DOI: 10.5435/jaaos-20-06-373 [8] Finger flexor tendon injuries repaired surgically followed by an early active motion program: A prospective cohort study of clinician- and patient-reported outcomes. Journal of Hand Therapy. 2026. DOI: 10.1016/j.jht.2024.12.011 [9] Tendinopathies of the Hand and Wrist. Journal of the American Academy of Orthopaedic Surgeons. 2015. DOI: 10.5435/jaaos-d-14-00216 [10] Volar wrist ganglion presenting as trigger finger. Journal of Hand Surgery (European Volume). 2012. DOI: 10.1177/1753193412453699 [11] Ganglion cysts and other tumor related conditions of the hand and wrist. Hand Clinics. 2004. DOI: 10.1016/j.hcl.2004.03.015 [12] Six-Strand Flexor Pollicis Longus Tendon Repairs With and Without Circumferential Sutures: A Multicenter Study. HAND. 2022. DOI: 10.1177/15589447211057295 [13] Accuracy and Safety of Non-Image Guided Trigger Finger Injections: A Cadaveric Study. HAND. 2022. DOI: 10.1177/15589447221093676 [15] A technique for accurately marking the A1 pulley on the skin. Journal of Hand Surgery (European Volume). 2012. DOI: 10.1177/1753193411436294 [17] Wide-awake Flexor Tendon Repair and Early Tendon Mobilization in Zones 1 and 2. Hand Clinics. 2013. DOI: 10.1016/j.hcl.2013.02.009 [18] Differential Pulley Release in Trigger Finger: A Prospective, Randomized Clinical Trial. HAND. 2021. DOI: 10.1177/1558944721994231 [20] Biomechanics and hand trauma: what you need. Hand Clinics. 2003. DOI: 10.1016/s0749-0712(02)00130-0 [23] Absent Ring Finger Flexor Digitorum Profundus Presenting as a Jersey Finger. The Journal of Hand Surgery. 2016. DOI: 10.1016/j.jhsa.2016.02.003 [25] Congenital Hypoplasia of the Extensor Tendons of the Fingers: A Case Report and Review of the Literature. The Journal of Hand Surgery. 2020. DOI: 10.1016/j.jhsa.2019.03.018 [26] An in-depth look at zone III and IV anatomy of the finger extensor mechanism and some clinical implications for use of the relative motion flexion orthosis. Journal of Hand Therapy. 2023. DOI: 10.1016/j.jht.2023.01.002 [27] The balanced finger: biomechanics of intrinsic and extrinsic systems and principles of reconstruction. Journal of Hand Surgery (European Volume). 2026. DOI: 10.1177/17531934261427638 [28] Hand Surface Landmarks and Measurements in the Treatment of Trigger Thumb. The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2013.02.028 [29] A commentary from the pioneers on the innovation of the relative motion concept: History, biologic considerations, and anatomic rationale. Journal of Hand Therapy. 2023. DOI: 10.1016/j.jht.2022.12.006 [32] Shear Strain and Motion of the Subsynovial Connective Tissue and Median Nerve During Single-Digit Motion. The Journal of Hand Surgery. 2009. DOI: 10.1016/j.jhsa.2008.09.021 [33] Ultrasonographic assessment in vivo of the excursion and tension of flexor digitorum profundus tendon on different rehabilitation protocols after tendon repair. Journal of Hand Therapy. 2022. DOI: 10.1016/j.jht.2021.01.006 [35] Longitudinal Tear of the Central Slip Causing Painful and Unusual Snapping of the Finger: A Case Report. HAND. 2022. DOI: 10.1177/15589447221081876 [36] Defining the Digit-Specific Confluence of the A1 Pulley. The Journal of Hand Surgery. 2023. DOI: 10.1016/j.jhsa.2022.02.011 [37] A comparison of ultrasound and clinical examination in the detection of flexor tenosynovitis in early arthritis. BMC Musculoskeletal Disorders. 2011. DOI: 10.1186/1471-2474-12-91





