Osteoartrite da Articulação Acromioclavicular
Patients › Shoulder
AC joint osteoarthritis causes localized shoulder pain with cross-body movements; treatment ranges from activity modification to surgery.
O que você está sentindo
Provavelmente você sente dor na parte superior do ombro, onde a clavícula encontra a escápula. Esta é a sua articulação acromioclavicular. A dor pode permanecer leve por anos. De fato, 90% das pessoas com sinais iniciais nos raios-X não sentem nenhuma dor durante um período de 7 anos. No entanto, se os sintomas começarem, eles frequentemente seguem um padrão previsível.
A dor geralmente piora quando você move o braço através do corpo. Você pode senti-la ao alcançar uma prateleira alta ou atrás das costas para fechar um sutiã. Encaixar a camisa também pode desencadear uma pontada aguda. Levantar objetos, especialmente acima da cabeça, exerce pressão direta sobre essa articulação. Muitos pacientes descobrem que descansar o braço ao lado do corpo traz alívio. O movimento suave geralmente parece melhor do que permanecer completamente imóvel.
A dor noturna é uma queixa comum. Você pode acordar se rolar sobre o ombro afetado. O peso do seu corpo pressiona a articulação inflamada, dificultando encontrar uma posição confortável. Algumas pessoas notam que a dor é pior quando acordam pela manhã. Pode parecer rigidez até que você se movimente por um tempo.
É importante saber que os achados de imagem nem sempre correspondem aos seus sintomas. Uma distinção entre a osteoartrite radiográfica da articulação acromioclavicular sintomática e assintomática é desnecessária. Todos os pacientes tiveram satisfação igual com o resultado da injeção acromioclavicular pré-operatória, independentemente do que os raios-X mostraram. Isso significa que seu nível de desconforto é o verdadeiro guia para o tratamento, não apenas a aparência da articulação em uma imagem.
Se você teve cirurgia anterior no ombro, como uma reparação do manguito rotador, a artrite não tratada nesta articulação está associada a uma baixa taxa de falha. Raramente causa problemas graves por si só. No entanto, se você experimentar dor persistente que interfere nas tarefas diárias, como se vestir ou dormir, seu cirurgião pode discutir opções como injeções ou cirurgia menor para remover as extremidades ósseas desgastadas. Esses procedimentos fornecem alívio da dor previsível para casos sintomáticos.
O que está realmente acontecendo
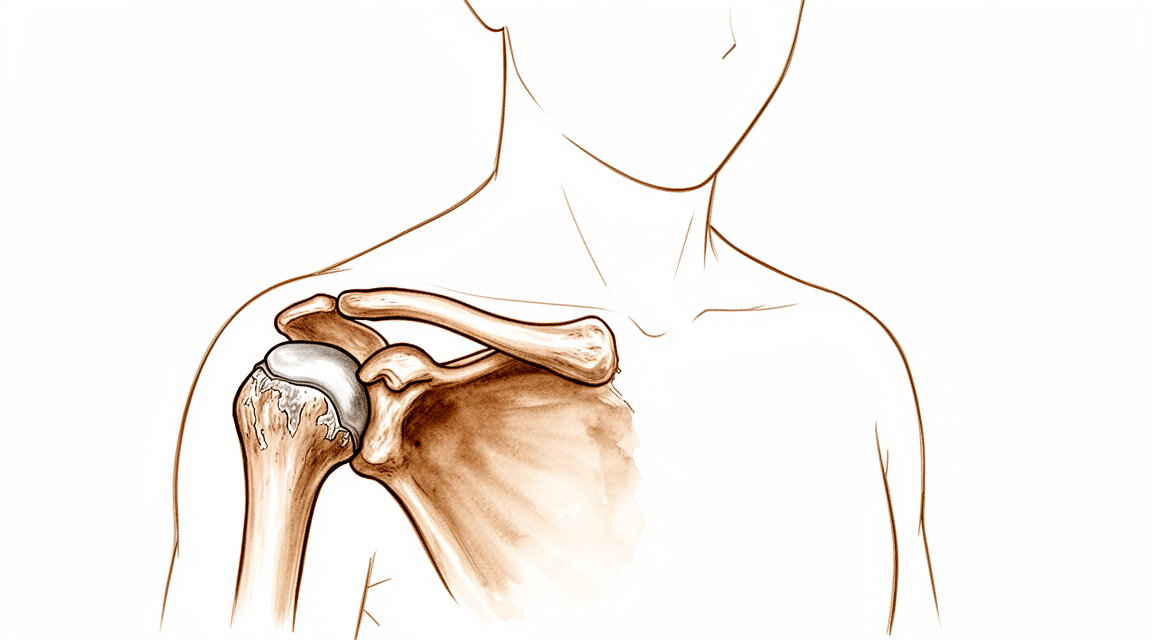
Sua articulação acromioclavicular (AC) situa-se no topo do ombro, onde a clavícula encontra a escápula. Pense nesta articulação como uma pequena dobradiça que permite que o braço se mova suavemente acima da cabeça. No interior, a cartilagem lisa atua como um amortecedor, acolchoando os ossos para que não se atritem uns contra os outros.
Na osteoartrite da articulação AC, esta cartilagem protetora desgasta-se ao longo do tempo. Trata-se essencialmente de uma artrite por desgaste. À medida que o acolchoamento se afina, os ossos roçam diretamente uns contra os outros. Esta fricção causa inflamação e dor, especialmente quando se atravessa o corpo com o braço ou se o levanta acima da cabeça. A cápsula articular, que é a bainha que envolve a articulação, também pode tornar-se rígida ou irritada, aumentando o desconforto.
Por vezes, os ligamentos que mantêm a clavícula no lugar estiram-se ou rompem-se. Isto pode fazer com que a clavícula fique mais elevada do que o normal, criando um inchaço visível. Quando isto acontece, o movimento normal da escápula altera-se. Estas alterações cinemáticas podem ser uma fonte potencial de dor e disfunção no ombro. Mesmo que a articulação pareça normal numa radiografia, o movimento alterado ainda pode causar sintomas.
É importante saber que nem todas as alterações numa radiografia significam que terá dor. A osteoartrite assintomática da articulação AC permaneceu assintomática em 90% dos pacientes ao longo de um período de 7 anos. Isto significa que muitas pessoas têm desgaste visível nas imagens, mas não sentem qualquer dor. A osteoartrite da articulação AC não tratada, seja sintomática ou não, encontrada durante a reparação artroscópica do manguito rotador está associada a uma baixa percentagem de falhas.
No entanto, se a artrite se tornar grave, pode levar a outros problemas. A osteoartrite grave da articulação acromioclavicular está associada a fraturas por stress do acrómio após artroplastia total do ombro reversa. O seu cirurgião irá analisar tanto os seus sintomas como as suas imagens para decidir se a articulação é realmente a fonte da sua dor.
O objetivo do tratamento é reduzir esta fricção e restaurar o movimento suave. Tanto as técnicas de artroplastia por ressecção aberta como as artroscópicas proporcionam um alívio da dor previsível na osteoartrite sintomática da articulação AC. Estes procedimentos envolvem a remoção de uma pequena parte da clavícula para criar mais espaço, permitindo que os ossos deslizem sem se atritarem. Esta simples alteração pode melhorar significativamente a função do ombro e reduzir a dor.
O que podemos fazer a respeito
Você pode iniciar com o autocuidado e a fisioterapia. Essa abordagem conservadora é um tratamento inicial válido para muitas lesões do ombro e condições articulares. Seu cirurgião pode sugerir a modificação das atividades se você tiver osteólise, que é o desgaste do osso. A fisioterapia visa fortalecer os músculos ao redor do seu ombro para apoiar a articulação. Os tratamentos conservadores e cirúrgicos são ambos eficazes no manejo da osteoartrite da articulação acromioclavicular. Dê uma chance justa a este tratamento não operatório, pois ele é benéfico para a maioria dos pacientes com condições dolorosas nessa área.
Se a dor persistir, seu cirurgião pode discutir o manejo médico. Isso geralmente inclui medicamentos para dor e anti-inflamatórios para reduzir o inchaço e o desconforto. Você também pode considerar injeções na articulação acromioclavicular. Essas injeções oferecem uma taxa de sucesso de 1 ano de 47% em pacientes com osteoartrite acromioclavicular. A injeção ajuda a reduzir a inflamação e a dor diretamente no local da articulação. A pesquisa ainda está comparando diferentes tipos de injeções de esteroides para ver qual funciona melhor para a dor isolada na articulação. Embora alguns pacientes encontrem alívio duradouro, outros podem precisar explorar outras opções se o efeito da injeção desaparecer.
A cirurgia é considerada quando o tratamento conservador atingiu seu limite e a dor continua a afetar sua vida diária. Ambas as técnicas de artroplastia por ressecção aberta e artroscópica fornecem alívio da dor previsível para a osteoartrite sintomática da articulação acromioclavicular. Este procedimento envolve a remoção de uma pequena parte da clavícula para criar mais espaço e reduzir o atrito. A excisão limitada da clavícula distal reduz a dor e melhora a função do ombro no acompanhamento intermediário em pacientes resistentes ao tratamento conservador. Seu cirurgião determinará se você é um bom candidato com base em seus sintomas específicos e nos resultados das imagens. Para alguns, essa simples remoção de tecido ósseo é suficiente para restaurar o conforto e o movimento sem a necessidade de reconstrução mais complexa.
O que esperar
Se você for diagnosticado com artrite por desgaste na articulação acromioclavicular (AC), mas não tiver dor, é provável que permaneça assim. Em 90% dos pacientes, a osteoartrite assintomática da articulação AC permaneceu assintomática durante um período de 7 anos. Você não precisa se preocupar com esse achado se ele não estiver causando incômodo. É comum observar sinais de artrite em exames de imagem mesmo na ausência de sintomas.
Se você tiver dor, o prognóstico depende de como você a gerencia. As injeções na articulação oferecem uma taxa de sucesso de 1 ano de 47%. Isso significa que quase metade dos pacientes encontra alívio duradouro com esse tratamento. Se as injeções não ajudarem, seu cirurgião pode recomendar um procedimento para remover uma pequena parte da clavícula. Essa excisão limitada da clavícula distal reduz a dor e melhora a função do ombro no acompanhamento intermediário para pacientes que não respondem ao tratamento conservador.
Você pode esperar alívio previsível da dor se optar pela cirurgia. Tanto as técnicas de ressecção aberta quanto as artroscópicas proporcionam esse alívio. No entanto, cada abordagem tem um conjunto único de complicações potenciais. Seu cirurgião discutirá qual método é o melhor para sua anatomia e estilo de vida específicos.
Se você deixar a artrite sintomática sem tratamento, ela pode persistir. Alguns pacientes experimentam desconforto contínuo que limita as atividades diárias. Se você se submeter a outras cirurgias no ombro, como o reparo do manguito rotador, a osteoartrite não tratada da articulação AC está associada a uma baixa taxa de falha. No entanto, a osteoartrite está geralmente associada a resultados clínicos finais piores após o reparo do manguito rotador. Um manguito rotador não cicatrizado ou que se rompe novamente também aumenta o risco de desenvolver essa artrite.
Nos casos graves, particularmente se você estiver recebendo uma prótese de ombro reversa, a osteoartrite grave da articulação AC está associada a fraturas por estresse do acrômio. A osteoartrite radiográfica da articulação AC é comum em pacientes que se submetem a esse tipo de cirurgia. Seu cirurgião monitorará esses riscos de perto.
No geral, o curso da artrite da articulação AC varia. Ela pode se resolver com o tratamento conservador, persistir apesar do tratamento ou progredir lentamente. A maioria dos pacientes observa que os tratamentos direcionados proporcionam melhora significativa na função e no conforto.
Quando procurar ajuda
Consulte o seu médico de família se tiver dor persistente que não melhora com o repouso. Solicite uma avaliação especializada se notar fraqueza ou instabilidade no ombro. Procure atendimento se a articulação bloquear ou ceder. Contacte o seu cirurgião se os sintomas interferirem no seu sono ou trabalho. O piora súbita da dor também é um motivo para procurar ajuda. Note que a artrose assintomática por desgaste frequentemente permanece indolor durante sete anos. No entanto, problemas não tratados podem, por vezes, afetar outras reparações do ombro. O seu médico irá avaliar a sensibilidade à palpação e discutir se uma injeção pode ser benéfica. Uma avaliação precoce garante que receba o tratamento adequado antes que a condição progrida.
Evidence & references
Overview
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Radiographic ACJ osteoarthritis is common in patients undergoing reverse shoulder arthroplasty [7].
- Severe acromioclavicular joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic AC osteoarthritis [8].
- Open and arthroscopic resection arthroplasty techniques have unique sets of potential complications that may be minimized with improved understanding of anatomy, biomechanics, and meticulous surgical technique [8].
- Limited distal clavicle excision reduced pain and improved shoulder function at midterm follow-up in patients with AC joint osteoarthritis resistant to conservative treatment [9].
- A distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary as all patients were equally satisfied with the outcome of preoperative acromioclavicular injection [6].
- Further characterisation of patients in whom mild arthroscopic findings of OA of the AC joint are clinically significant and warrant resection is needed [1].
- Acromioclavicular joint arthritis is not an indication for routine distal clavicle excision in arthroscopic rotator cuff repair [3].
- Clinicians should consider overreduction of the AC joint because it may lead to favorable radiological results [5].
- The authors recommend anatomic reconstruction procedures for the treatment of chronic complete AC dislocations [21].
Anatomy & Pathophysiology
- Anatomic techniques that address both coracoclavicular ligaments and the AC capsule are recommended to restore horizontal and vertical stability while allowing physiological rotation [10].
- None of the reconstruction strategies completely restored the shoulder girdle to its preinjured state [26].
- Kinematic changes resulting from AC joint dislocation could be a potential source of pain and dysfunction in the shoulder [27].
- Scapular and clavicular kinematics were affected in AC separation models [28].
- The position of the hook portion of a clavicle hook plate can predispose anatomic structures to post-operative complications of subacromial impingement and bony erosion [29].
- Future research should focus on addressing horizontal and rotational instability to restore native physiological and biomechanical properties of the AC joint [35].
- Coracoclavicular reconstruction with augmentation of the acromioclavicular joint provides improved horizontal stability compared to isolated coracoclavicular reconstruction [41].
- Adding a fixation of the AC joint minimizes lateral tilting of the scapula and maintains a more anatomic reposition result over time [45].
Classification
- Asymptomatic acromioclavicular osteoarthritis diagnosed by MRI remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated acromioclavicular joint osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Mild arthroscopic findings of acromioclavicular joint osteoarthritis may be clinically significant and warrant resection, but further characterization of such patients is needed [1].
- Severe acromioclavicular joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Radiographic acromioclavicular joint osteoarthritis is common in patients undergoing reverse shoulder arthroplasty [7].
- Osteolytic changes in the acromioclavicular joint seemed to be associated with incongruity of the joint but did not correlate with clinical results [11].
- The acromial center line to dorsal clavicle radiographic measurement and the use of the Alexander view provide a more realistic appreciation of true acromioclavicular joint displacement, especially in defining watershed cases (Rockwood types IIIA, IIB, and IV) [12].
- Evaluating the integrity of the capsuloligamentous structures stabilizing the acromioclavicular joint is reproducible and provides additional information on the severity of the injury [24].
- Injuries to the sternoclavicular joint are uncommon, and recognition and classification are critical to proper management to minimize long-term sequelae [16].
- Some persistent pain and osteoarthritis progression remain concerns in the arthroscopic revision of failed open anterior stabilization of the shoulder [4].
Clinical Presentation
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Preventive arthroscopic distal clavicle resection is not recommended in patients with radiological but asymptomatic ACJ arthritis [19].
- Further characterisation of patients in whom mild arthroscopic findings of OA of the AC joint are clinically significant and warrant resection is needed [1].
- A distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary, as all patients were equally satisfied with the outcome of preoperative acromioclavicular injection [6].
- Osteolytic changes seemed to be associated with incongruity of the AC joint, but did not correlate with clinical results [11].
- Additional research is needed to determine the main cause of pain in isolated acromioclavicular osteoarthritis and to compare clinical outcomes of intra-articular versus extra-articular injections [13].
- Risk factors for subsequent distal clavicle excision after rotator cuff repair include tenderness to palpation at the AC joint, female sex, and surgery on the dominant side [18].
- Subsequent distal clavicle excision was performed in 40% of cases with a combination of the three identified risk factors (tenderness to palpation, female sex, dominant side surgery) [18].
- Recurrence of the initial dislocation after arthroscopically assisted reduction appears to be related to the onset of degenerative ACJ arthropathy [14].
- Some persistent pain and osteoarthritis progression remain concerns in the revision of failed open anterior stabilization of the shoulder [4].
Investigations
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Preventive arthroscopic distal clavicle resection (DCR) is not recommended in patients with radiological but asymptomatic ACJ arthritis [19].
- Further characterization is needed to determine which patients with mild arthroscopic findings of AC joint OA are clinically significant and warrant resection [1].
- Radiographic ACJ osteoarthritis is common in patients undergoing reverse shoulder arthroplasty (RSA) [7].
- Severe ACJ osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Osteolytic changes in the AC joint seemed to be associated with incongruity but did not correlate with clinical results [11].
- Patients with edema on MRI were more likely to present with pain than patients without edema [43].
- Subchondral bone edema on histologic examination was more frequent in patients with pain [43].
- The outcomes of a preoperative AC injection suggest that a distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary, as all patients were equally satisfied with the outcome [6].
- Additional research is needed to determine the main cause of pain and to compare clinical outcomes of intra-articular versus extra-articular steroid injections for isolated AC osteoarthritis [13].
- Risk factors for subsequent distal clavicle excision after rotator cuff repair include tenderness to palpation at the AC joint, female sex, and surgery on the dominant side [18].
- Subsequent distal clavicle excision was performed in 40% of cases with a combination of the three identified risk factors (tenderness, female sex, dominant side) [18].
- The arthroscopic approach offers an advantage in diagnosing and treating occult intra-articular pathology during distal clavicle excision [20].
- Some persistent pain and osteoarthritis progression remain concerns in the revision of failed open anterior stabilization of the shoulder using arthroscopy [4].
- Evaluating the integrity of the capsuloligamentous structures stabilizing the AC joint is reproducible and provides additional information on injury severity, which may influence treatment decisions [24].
- The AC-DC measurement and use of the Alexander view provide a more realistic appreciation of true AC joint displacement, particularly in defining watershed cases (IIIA/IIB/IV) [12].
- Radiological failures were observed in 41% of cases in a prospective multicenter study of arthroscopic acute AC dislocation fixation [50].
Treatment
Non-Operative Management
- Conservative therapy is a valid initial treatment option for Rockwood Type V acromioclavicular dislocations [15].
- Non-operative reduction and stabilization is a valuable treatment option for acute high-grade acromioclavicular joint separations [33].
- Nonoperative treatment is helpful for most patients with painful conditions of the acromioclavicular joint, although those with osteolysis may need to modify their activities [44].
- Conservative and surgical treatments are both effective in the management of acromioclavicular joint osteoarthritis [17].
- Acromioclavicular injections offer a 1-year success rate of 47% in patients with acromioclavicular osteoarthritis [22].
- Additional research is needed to determine the main cause of pain and to compare clinical outcomes of intra-articular versus extra-articular steroid injections for isolated acromioclavicular osteoarthritis [13].
Operative Management
- Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic acromioclavicular osteoarthritis [8].
- Limited distal clavicle excision reduces pain and improves shoulder function at midterm follow-up in patients with acromioclavicular joint osteoarthritis resistant to conservative treatment [9].
- Untreated acromioclavicular joint osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Further characterization is needed to identify patients in whom mild arthroscopic findings of acromioclavicular joint osteoarthritis are clinically significant and warrant resection [1].
- Conversion to anatomic coracoclavicular ligament reconstruction shows similar clinical outcomes compared to successful non-operative treatment in chronic primary type III to V acromioclavicular joint injuries at a minimum 5-year follow-up [49].
- The authors recommend anatomic reconstruction procedures for the treatment of chronic complete acromioclavicular dislocations [21].
- Osteoarthritis is associated with poorer final clinical outcomes after rotator cuff repair, and an unhealed or re-torn cuff increases the risk of osteoarthritis [23].
Diagnostic Considerations
- A distinction between symptomatic and asymptomatic radiographic acromioclavicular osteoarthritis appears unnecessary, as all patients were equally satisfied with the outcome of preoperative acromioclavicular injection [6].
- Asymptomatic acromioclavicular osteoarthritis diagnosed by MRI remained asymptomatic in 90% of patients over a 7-year course [2].
- Some persistent pain and osteoarthritis progression remain concerns following arthroscopy in the revision of failed open anterior stabilization of the shoulder [4].
Complications
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Osteoarthritis is associated with poorer final clinical outcomes after rotator cuff repair [23].
- An unhealed or re-torn rotator cuff increases the risk of developing osteoarthritis [23].
- Severe AC joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Radiographic ACJ osteoarthritis is common in patients undergoing reverse shoulder arthroplasty [7].
- Some persistent pain and osteoarthritis progression remain concerns following arthroscopy in revision of failed open anterior stabilization of the shoulder [4].
- Recurrence of the initial dislocation after arthroscopically assisted reduction of acute AC joint dislocation appears to be related to the onset of degenerative ACJ arthropathy [14].
- Treatment of acute grade III and IV AC dislocations by synthetic ligament reconstruction carries a risk of significant early osteolysis [25].
- Open and arthroscopic AC joint reconstruction techniques have no differences in loss of reduction, complication rate, or revision rate [38].
- Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic AC osteoarthritis but each has a unique set of potential complications [8].
Recovery
- Asymptomatic acromioclavicular osteoarthritis diagnosed by MRI remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated acromioclavicular joint osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Limited distal clavicle excision for acromioclavicular joint osteoarthritis resistant to conservative treatment reduced pain and improved shoulder function at midterm follow-up [9].
- Acromioclavicular injections offer a 1-year success rate of 47% in patients with acromioclavicular osteoarthritis [22].
- A preoperative acromioclavicular injection study suggested that distinguishing between symptomatic and asymptomatic radiographic acromioclavicular osteoarthritis is unnecessary, as all patients were equally satisfied with the outcome [6].
- Osteolytic changes in the acromioclavicular joint seemed to be associated with incongruity but did not correlate with clinical results [11].
- Recurrence of initial acromioclavicular joint dislocation appears to be related to the onset of degenerative acromioclavicular joint arthropathy [14].
- Treatment of acute grade III and IV acromioclavicular dislocations using synthetic ligament reconstruction gave satisfactory results in terms of recovery of strength, but evolution is not risk-free due to the onset of significant early osteolysis [25].
- Arthroscopic coracoclavicular ligament reconstruction with double-bundle soft tissue allograft for chronic type V acromioclavicular dislocations showed sustained and statistically significant improvements in functional outcomes, high rates of return to sport, and maintenance of active-duty military status at minimum 10-year follow-up [39].
- Minimally invasive coracoclavicular ligament augmentation with a flip button/polydioxanone repair for total acromioclavicular joint dislocation revealed excellent radiologic and clinical results with no subluxations or dislocations noted in short-term follow-up [48].
- Some persistent pain and osteoarthritis progression remain concerns in the arthroscopic revision of failed open anterior stabilization of the shoulder [4].
- Type V acromioclavicular dislocations may be given a trial of conservative therapy [15].
Key Evidence
- [L2] Further characterisation of patients in whom mild arthroscopic findings of OA of AC joint are clinically significant and warrant resection is needed. [1] (10.1007/s00167-014-3114-2)
- [L2] Asymptomatic AC-OA remained asymptomatic in 90% over 7 years. [2] (10.1016/j.jse.2019.04.004)
- [L2] Untreated ACJ osteoarthritis, symptomatic or not, encountered during arthroscopic RCR is associated with a low percentage of failure. [3] (10.1007/s00167-020-06098-y)
- [L4] Some persistent pain and osteoarthritis progression remain concerns. [4] (10.1016/j.arthro.2009.04.073)
- [L3] Clinicians should consider overreduction of the AC joint because it may lead to favorable radiological results. [5] (10.1177/0363546519862850)
- [L4] The outcomes of this study seem to suggest that a distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary, as all patients were equally satisfied with the outcome. [6] (10.5397/cise.2023.00073)
- [L3] Radiographic ACJ osteoarthritis is common in patients undergoing RSA. [7] (10.1016/j.jseint.2021.11.008)
- [L5] Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic AC osteoarthritis, though each has a unique set of potential complications that may be minimized with improved understanding of anatomy, biomechanics, and meticulous surgical technique. [8] (10.1177/0363546513485359)
- [L4] Limited distal clavicle excision of patients with AC joint osteoarthritis resistant to conservative treatment reduced pain and improved shoulder function at midterm follow-up. [9] (10.1016/j.otsr.2016.01.008)
- [L5] Anatomic techniques that address both coracoclavicular ligaments and the AC capsule are recommended to restore horizontal and vertical stability while allowing physiological rotation. [10] (10.1016/j.arthro.2019.01.038)
- [L4] The AC-DC measurement and use of the Alexander view provides the clinician with a more realistic appreciation of true AC joint displacement, especially in defining watershed cases (ie, IIIA/IIB/IV) and may better inform the decision-making process regarding management options and recommendations. [12] (10.1016/j.jse.2019.12.014)
- [L4] Additional research is needed to determine the main cause of pain and compare clinical outcomes of intra-articular versus extra-articular injections. [13] (10.5397/cise.2023.00311)
- [L4] Recurrence of the initial dislocation appears to be related to onset of degenerative ACJ arthropathy. [14] (10.1016/j.otsr.2017.11.001)
- [L4] This suggests that Type V AC dislocations may be given a trial of conservative therapy. [15] (10.1177/2325967115s00017)
- [L1] Injuries to the SC joint are uncommon, and recognition and classification are critical to proper management to minimize long-term sequelae. [16] (10.1177/0363546513498990)
- [L4] Conservative and surgical treatments are both effective in acromioclavicular joint osteoarthritis management. [17] (10.1007/s00167-020-06377-8)
- [L3] Risk factors for subsequent DCE included tenderness to palpation at the AC joint, female sex, and surgery on the dominant side, with subsequent DCE performed in 40% of cases with a combination of these 3 factors. [18] (10.1177/2325967119844295)
- [L1] Preventive arthroscopic DCR is not recommended in patients with radiological but asymptomatic ACJ arthritis. [19] (10.1177/0363546514547254)
- [L1] The arthroscopic approach offers a unique advantage in diagnosing and treating occult intra-articular pathology. [20] (10.1016/j.jse.2006.10.006)
- [L4] The authors recommend this procedure for the treatment of chronic complete AC dislocations. [21] (10.1016/j.injury.2010.09.023)
- [L4] AC injections offer a 1-year success rate of 47%. [22] (10.5397/cise.2023.00031)
- [L4] Osteoarthritis is associated with poorer final clinical outcomes, and an unhealed or re-torn cuff increases the risk of osteoarthritis. [23] (10.1016/j.otsr.2017.03.007)
- [L1] Evaluating the integrity of the capsuloligamentous structures stabilizing the AC joint is reproducible and gives additional information on the severity of the injury, which might also influence the treatment decision. [24] (10.1016/j.jse.2020.10.026)
- [L4] Treatment of ACD by synthetic ligament reconstruction gave satisfactory results, notably in terms of recovery of strength, but evolution is not risk-free with onset of significant early osteolysis. [25] (10.1016/j.otsr.2010.06.004)
- [L5] Although each technique was able to restore different elements of the joint kinematics, none of the strategies completely restored the shoulder girdle to its preinjured state. [26] (10.1177/03635465221095231)
- [L5] The kinematic changes could be a potential source of pain and dysfunction in the shoulder with AC joint dislocation. [27] (10.1177/0363546512458571)
- [L5] Scapular and clavicular kinematics were affected in AC separation models. [28] (10.1016/j.jse.2013.01.004)
- [L5] The observed frequency of hook contact with surrounding subacromial structures in a static shoulder confirms that the position of the hook portion of the implant can predispose anatomic structures to the post-operative complications of subacromial impingement and bony erosion. [29] (10.1016/j.injury.2009.12.012)
- [L4] Non-operative reduction and stabilization of high-grade AC joint separations seems to be a valuable treatment option. [33] (10.1007/s00402-020-03630-0)
- [L5] Future research should focus on addressing horizontal and rotational instability, to restore native physiological and biomechanical properties of the AC joint. [35] (10.1186/s12891-022-05935-0)
- [L1] Open and arthroscopic AC joint reconstruction techniques have no differences in loss of reduction, the complication rate, and the revision rate based on the available literature. [38] (10.1177/0363546518795147)
- [L4] Outcomes after arthroscopic CC reconstruction for chronic, type V AC dislocations in an active-duty military patient population show sustained and statistically significant improvements in functional outcomes as well as high rates of return to sport and maintenance of active-duty military status at long-term follow-up. [39] (10.1016/j.arthro.2025.05.008)
- [L1] Coracoclavicular reconstruction with augmentation of the acromioclavicular joint has been shown to provide improved horizontal stability in both biomechanical and clinical studies compared to isolated coracoclavicular reconstruction. [41] (10.1007/s00167-018-5152-7)
- [L4] Patients with edema on MRI were more likely to present pain than patients without edema, and subchondral bone edema on histologic examination was more frequent in patients with pain. [43] (10.1016/j.jseint.2020.03.007)
- [L5] Nonoperative treatment is helpful for most patients, although those with osteolysis may have to modify their activities. [44] (10.5435/00124635-199905000-00004)
- [L3] The presented data suggest adding a fixation of the AC joint to minimize lateral tilting of the scapula and maintain a more anatomic reposition result over time. [45] (10.1007/s00402-021-03761-y)
- [L4] The short-term follow-up of 15 recently operated patients reveals excellent radiologic and clinical results, with no subluxations or dislocations of the acromioclavicular joint noted. [48] (10.1016/j.arthro.2006.12.015)
- [L4] At a minimum 5-year follow-up, patients with successful non-operative treatment for type III-V ACJ injuries achieved similar clinical outcomes compared to those who were converted to ACCR. [49] (10.1007/s00167-020-06159-2)
- [L4] Surgery for AC dislocations is difficult with radiological results that must still be improved, as radiological failures were observed in 41% of cases. [50] (10.1016/j.otsr.2015.09.012)
References
[1] Outcome of distal clavicle resection in patients with acromioclavicular joint osteoarthritis and full‐thickness rotator cuff tear. Knee Surgery, Sports Traumatology, Arthroscopy. 2014. DOI: 10.1007/s00167-014-3114-2 [2] Seven-year course of asymptomatic acromioclavicular osteoarthritis diagnosed by MRI. Journal of Shoulder and Elbow Surgery. 2019. DOI: 10.1016/j.jse.2019.04.004 [3] Acromioclavicular joint arthritis is not an indication for routine distal clavicle excision in arthroscopic rotator cuff repair. Knee Surgery, Sports Traumatology, Arthroscopy. 2020. DOI: 10.1007/s00167-020-06098-y [4] The Role of Arthroscopy in Revision of Failed Open Anterior Stabilization of the Shoulder. Arthroscopy. 2009. DOI: 10.1016/j.arthro.2009.04.073 [5] Factors Predicting the Outcome After Arthroscopically Assisted Stabilization of Acute High-Grade Acromioclavicular Joint Dislocations. The American Journal of Sports Medicine. 2019. DOI: 10.1177/0363546519862850 [6] Diagnostic value of a preoperative acromioclavicular injection for symptomatic acromioclavicular osteoarthritis: a retrospective study of cross-sectional midterm outcomes. Clinics in Shoulder and Elbow. 2024. DOI: 10.5397/cise.2023.00073 [7] Severe acromioclavicular joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty. JSES International. 2022. DOI: 10.1016/j.jseint.2021.11.008 [8] Degenerative Joint Disease of the Acromioclavicular Joint. The American Journal of Sports Medicine. 2013. DOI: 10.1177/0363546513485359 [9] Limited distal clavicle excision of acromioclavicular joint osteoarthritis. Orthopaedics & Traumatology: Surgery & Research. 2016. DOI: 10.1016/j.otsr.2016.01.008 [10] Editorial Commentary: Why We Have To Respect The Anatomy In Acromioclavicular Joint Surgery And Why Clinical Shoulder Scores Might Not Give Us The Information We Need!. Arthroscopy. 2019. DOI: 10.1016/j.arthro.2019.01.038 [11] 10.1016-0020-1383-83-90092-x. n.d.. [12] Improved identification of unstable acromioclavicular joint injuries in a clinical population using the acromial center line to dorsal clavicle radiographic measurement. Journal of Shoulder and Elbow Surgery. 2020. DOI: 10.1016/j.jse.2019.12.014 [13] Isolated acromioclavicular osteoarthritis and steroid injection. Clinics in Shoulder and Elbow. 2023. DOI: 10.5397/cise.2023.00311 [14] Arthroscopically assisted reduction of acute acromioclavicular joint dislocation using a single double-button device: Medium-term clinical and radiological outcomes. Orthopaedics & Traumatology: Surgery & Research. 2018. DOI: 10.1016/j.otsr.2017.11.001 [15] Successful Conservative Therapy in Rockwood Type V Acromioclavicular Dislocations. Orthopaedic Journal of Sports Medicine. 2015. DOI: 10.1177/2325967115s00017 [16] Instability and Degenerative Arthritis of the Sternoclavicular Joint. The American Journal of Sports Medicine. 2013. DOI: 10.1177/0363546513498990 [17] No differences between conservative and surgical management of acromioclavicular joint osteoarthritis: a scoping review. Knee Surgery, Sports Traumatology, Arthroscopy. 2021. DOI: 10.1007/s00167-020-06377-8 [18] Preoperative Factors Associated With Subsequent Distal Clavicle Resection After Rotator Cuff Repair. Orthopaedic Journal of Sports Medicine. 2019. DOI: 10.1177/2325967119844295 [19] Is Arthroscopic Distal Clavicle Resection Necessary for Patients With Radiological Acromioclavicular Joint Arthritis and Rotator Cuff Tears?. The American Journal of Sports Medicine. 2014. DOI: 10.1177/0363546514547254 [20] Arthroscopic versus open distal clavicle excision: Comparative results at six months and one year from a randomized, prospective clinical trial. Journal of Shoulder and Elbow Surgery. 2007. DOI: 10.1016/j.jse.2006.10.006 [21] Surgical treatment of chronic acromioclavicular dislocation: Comparison between two surgical procedures for anatomic reconstruction. Injury. 2010. DOI: 10.1016/j.injury.2010.09.023 [22] Mid- to long-term success rate and functional outcomes of acromioclavicular injections in patients with acromioclavicular osteoarthritis. Clinics in Shoulder and Elbow. 2023. DOI: 10.5397/cise.2023.00031 [23] Osteoarthritis after rotator cuff repair: A 10-year follow-up study. Orthopaedics & Traumatology: Surgery & Research. 2017. DOI: 10.1016/j.otsr.2017.03.007 [24] The ligamentous injury pattern in acute acromioclavicular dislocations and its impact on clinical and radiographic parameters. Journal of Shoulder and Elbow Surgery. 2021. DOI: 10.1016/j.jse.2020.10.026 [25] Acute grade III and IV acromioclavicular dislocations: Outcomes and pitfalls of reconstruction procedures using a synthetic ligament. Orthopaedics & Traumatology: Surgery & Research. 2010. DOI: 10.1016/j.otsr.2010.06.004 [26] Differences between Coracoclavicular, Acromioclavicular, or Combined Reconstruction Techniques on the Kinematics of the Shoulder Girdle. The American Journal of Sports Medicine. 2022. DOI: 10.1177/03635465221095231 [27] The Function of the Acromioclavicular and Coracoclavicular Ligaments in Shoulder Motion. The American Journal of Sports Medicine. 2012. DOI: 10.1177/0363546512458571 [28] Acromioclavicular joint ligamentous system contributing to clavicular strut function: a cadaveric study. Journal of Shoulder and Elbow Surgery. 2013. DOI: 10.1016/j.jse.2013.01.004 [29] Subacromial morphometric assessment of the clavicle hook plate. Injury. 2010. DOI: 10.1016/j.injury.2009.12.012 [33] Can an acute high-grade acromioclavicular joint separation be reduced and stabilized without surgery? A surgeon’s experience. Archives of Orthopaedic and Trauma Surgery. 2020. DOI: 10.1007/s00402-020-03630-0 [35] Current concepts in acromioclavicular joint (AC) instability – a proposed treatment algorithm for acute and chronic AC-joint surgery. BMC Musculoskeletal Disorders. 2022. DOI: 10.1186/s12891-022-05935-0 [38] Current Concepts in the Operative Management of Acromioclavicular Dislocations: A Systematic Review and Meta-analysis of Operative Techniques. The American Journal of Sports Medicine. 2018. DOI: 10.1177/0363546518795147 [39] Arthroscopic Coracoclavicular Ligament Reconstruction With Double‐Bundle Soft Tissue Allograft for Chronic Type V Acromioclavicular Dislocations Shows Excellent Patient Outcomes and Return to Duty and Sport at Minimum 10‐Year Follow‐Up. Arthroscopy. 2025. DOI: 10.1016/j.arthro.2025.05.008 [41] Acromioclavicular joint augmentation at the time of coracoclavicular ligament reconstruction fails to improve functional outcomes despite significantly improved horizontal stability. Knee Surgery, Sports Traumatology, Arthroscopy. 2018. DOI: 10.1007/s00167-018-5152-7 [43] Histologic and magnetic resonance image evaluation in acromioclavicular joint osteoarthritis. JSES International. 2020. DOI: 10.1016/j.jseint.2020.03.007 [44] Painful Conditions of the Acromioclavicular Joint. Journal of the American Academy of Orthopaedic Surgeons. 1999. DOI: 10.5435/00124635-199905000-00004 [45] Additional acromioclavicular cerclage limits lateral tilt of the scapula in patients with arthroscopically assisted coracoclavicular ligament reconstruction. Archives of Orthopaedic and Trauma Surgery. 2021. DOI: 10.1007/s00402-021-03761-y [48] Minimally Invasive Coracoclavicular Ligament Augmentation With a Flip Button/Polydioxanone Repair for Treatment of Total Acromioclavicular Joint Dislocation. Arthroscopy. 2007. DOI: 10.1016/j.arthro.2006.12.015 [49] Conversion to anatomic coracoclavicular ligament reconstruction (ACCR) shows similar clinical outcomes compared to successful non‐operative treatment in chronic primary type III to V acromioclavicular joint injuries. Knee Surgery, Sports Traumatology, Arthroscopy. 2020. DOI: 10.1007/s00167-020-06159-2 [50] Complication rates and types of failure after arthroscopic acute acromioclavicular dislocation fixation. Prospective multicenter study of 116 cases. Orthopaedics & Traumatology: Surgery & Research. 2015. DOI: 10.1016/j.otsr.2015.09.012





