Viêm xương khớp khớp cùng đòn
Patients › Shoulder
AC joint osteoarthritis causes localized shoulder pain with cross-body movements; treatment ranges from activity modification to surgery.
Những gì bạn đang cảm thấy
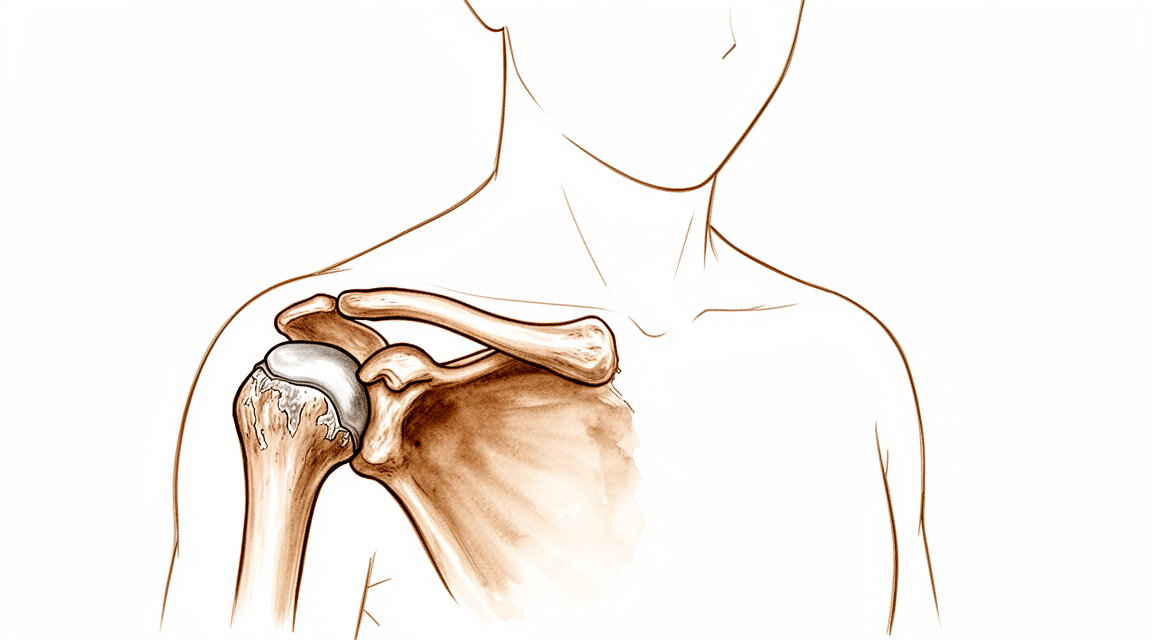
Bạn có thể cảm thấy đau ở phần trên cùng của vai, nơi xương đòn gặp xương bả vai. Đây là khớp đòn vai (acromioclavicular joint). Cơn đau có thể duy trì ở mức nhẹ trong nhiều năm. Thực tế, 90% những người có dấu hiệu sớm trên phim X-quang không cảm thấy đau trong vòng 7 năm. Tuy nhiên, nếu các triệu chứng bắt đầu xuất hiện, chúng thường tuân theo một diễn biến có thể dự đoán được.
Cơn đau thường trở nên nghiêm trọng hơn khi bạn di chuyển cánh tay qua ngang cơ thể. Bạn có thể cảm thấy đau khi với tay lên kệ cao hoặc đưa tay ra sau lưng để cài khuy áo ngực. Việc nhét áo vào quần cũng có thể kích hoạt cảm giác đau nhói. Việc nâng vật, đặc biệt là trên đầu, tạo áp lực trực tiếp lên khớp này. Nhiều bệnh nhân nhận thấy rằng nghỉ ngơi cánh tay ở bên hông cơ thể giúp giảm đau. Vận động nhẹ thường cảm thấy dễ chịu hơn là giữ nguyên hoàn toàn bất động.
Đau về đêm là một phàn nàn phổ biến. Bạn có thể thức giấc nếu lăn sang vai bị ảnh hưởng. Trọng lượng cơ thể đè lên khớp đang viêm, khiến bạn khó tìm được tư thế thoải mái. Một số người nhận thấy cơn đau nặng hơn khi vừa thức dậy vào buổi sáng. Cảm giác cứng khớp có thể tồn tại cho đến khi bạn di chuyển trong một thời gian.
Điều quan trọng cần biết là các kết quả hình ảnh học không phải lúc nào cũng khớp với các triệu chứng của bạn. Việc phân biệt giữa viêm xương khớp khớp đòn vai (AC) có triệu chứng và không có triệu chứng trên phim X-quang là không cần thiết. Tất cả bệnh nhân đều hài lòng như nhau với kết quả của việc tiêm khớp đòn vai trước phẫu thuật, bất kể phim X-quang cho thấy gì. Điều này có nghĩa là mức độ khó chịu của bạn mới là yếu tố hướng dẫn điều trị thực sự, chứ không chỉ là hình ảnh của khớp trên phim chụp.
Nếu bạn đã từng phẫu thuật vai trước đó, chẳng hạn như sửa chữa chóp xoay, viêm xương khớp chưa được điều trị ở khớp này có liên quan đến tỷ lệ thất bại thấp. Nó hiếm khi gây ra các vấn đề nghiêm trọng khi đứng một mình. Tuy nhiên, nếu bạn trải qua cơn đau dai dẳng cản trở các hoạt động hàng ngày như mặc quần áo hoặc ngủ, bác sĩ phẫu thuật của bạn có thể thảo luận về các lựa chọn như tiêm thuốc hoặc phẫu thuật nhỏ để loại bỏ các đầu xương bị mòn. Các thủ thuật này mang lại giảm đau dự đoán được cho các trường hợp có triệu chứng.
Những gì thực sự đang xảy ra
Khớp ức đòn (AC) nằm ở vị trí cao nhất của vai, nơi xương đòn gặp xương bả vai. Hãy tưởng tượng khớp này như một bản lề nhỏ cho phép cánh tay của bạn di chuyển mượt mà lên cao. Bên trong, sụn trơn hoạt động như một bộ giảm xóc, đệm giữa các xương để chúng không ma sát vào nhau.
Trong viêm xương khớp AC, lớp sụn bảo vệ này mòn đi theo thời gian. Về cơ bản, đây là viêm xương khớp do hao mòn. Khi lớp đệm mỏng đi, các xương cọ xát trực tiếp vào nhau hơn. Ma sát này gây viêm và đau, đặc biệt khi bạn đưa tay qua ngang cơ thể hoặc nâng cánh tay lên cao. Bao khớp, là lớp vỏ bao quanh khớp, cũng có thể trở nên cứng hoặc kích ứng, làm tăng thêm sự khó chịu.
Đôi khi, các dây chằng giữ xương đòn tại chỗ bị giãn hoặc rách. Điều này có thể khiến xương đòn nằm cao hơn bình thường, tạo ra một khối u nhìn thấy được. Khi điều này xảy ra, chuyển động bình thường của xương bả vai thay đổi. Những thay đổi về động học này có thể là nguồn gốc tiềm ẩn của đau và rối loạn chức năng ở vai. Ngay cả khi khớp trông bình thường trên phim X-quang, chuyển động bị thay đổi vẫn có thể gây ra các triệu chứng.
Điều quan trọng cần biết là không phải tất cả các thay đổi trên phim X-quang đều có nghĩa là bạn sẽ bị đau. Viêm xương khớp AC không triệu chứng vẫn không triệu chứng ở 90% bệnh nhân trong khoảng thời gian 7 năm. Điều này có nghĩa là nhiều người có dấu hiệu hao mòn rõ ràng trên hình ảnh chụp nhưng hoàn toàn không cảm thấy đau. Viêm xương khớp khớp AC không được điều trị, dù có triệu chứng hay không, được phát hiện trong quá trình sửa chữa chóp xoay nội soi có liên quan đến tỷ lệ thất bại thấp.
Tuy nhiên, nếu viêm xương khớp trở nên nghiêm trọng, nó có thể dẫn đến các vấn đề khác. Viêm xương khớp khớp ức đòn nghiêm trọng có liên quan đến gãy xương do căng thẳng ở mỏm cùng vai sau khi thay khớp vai ngược. Bác sĩ phẫu thuật của bạn sẽ xem xét cả triệu chứng và hình ảnh của bạn để quyết định xem khớp có thực sự là nguồn gốc cơn đau của bạn hay không.
Mục tiêu của điều trị là giảm ma sát này và khôi phục chuyển động mượt mà. Cả hai kỹ thuật cắt bỏ khớp nội soi và mổ mở đều cung cấp giảm đau dự đoán được cho viêm xương khớp AC có triệu chứng. Các thủ thuật này liên quan đến việc loại bỏ một phần nhỏ của xương đòn để tạo thêm không gian, cho phép các xương trượt mà không cọ xát. Thay đổi đơn giản này có thể cải thiện đáng kể chức năng vai và giảm đau của bạn.
Những gì chúng tôi có thể làm về vấn đề này
Bạn có thể bắt đầu bằng cách tự chăm sóc và vật lý trị liệu. Phương pháp điều trị bảo tồn này là một lựa chọn điều trị ban đầu hợp lý cho nhiều chấn thương vai và bệnh lý khớp. Bác sĩ phẫu thuật của bạn có thể đề xuất điều chỉnh các hoạt động nếu bạn bị tiêu xương (osteolysis), tức là sự mòn đi của xương. Vật lý trị liệu nhằm mục đích tăng cường các cơ xung quanh vai để hỗ trợ khớp. Cả điều trị bảo tồn và phẫu thuật đều hiệu quả trong việc quản lý viêm xương khớp khớp đòn vai. Hãy cho phương pháp điều trị không phẫu thuật này một cơ hội công bằng, vì nó hữu ích cho hầu hết bệnh nhân có các tình trạng đau đớn ở khu vực này.
Nếu cơn đau vẫn tiếp diễn, bác sĩ phẫu thuật của bạn có thể thảo luận về quản lý bằng thuốc. Điều này thường bao gồm thuốc giảm đau và thuốc chống viêm để giảm sưng và khó chịu. Bạn cũng có thể xem xét tiêm vào khớp đòn vai. Những mũi tiêm này có tỷ lệ thành công sau 1 năm là 47% ở bệnh nhân bị viêm xương khớp khớp đòn vai. Mũi tiêm giúp giảm viêm và đau trực tiếp tại vị trí khớp. Nghiên cứu vẫn đang so sánh các loại tiêm steroid khác nhau để xem loại nào hiệu quả nhất cho tình trạng đau khớp cô lập. Trong khi một số bệnh nhân tìm thấy sự giảm đau lâu dài, những người khác có thể cần khám phá các lựa chọn khác nếu hiệu quả của mũi tiêm giảm đi.
Phẫu thuật được xem xét khi chăm sóc bảo tồn đã đạt đến giới hạn và cơn đau tiếp tục ảnh hưởng đến cuộc sống hàng ngày của bạn. Cả hai kỹ thuật cắt bỏ khớp nội soi và mổ mở đều mang lại giảm đau dự đoán được cho viêm xương khớp khớp đòn vai có triệu chứng. Thủ thuật này liên quan đến việc loại bỏ một phần nhỏ của xương đòn để tạo thêm không gian và giảm ma sát. Cắt bỏ hạn chế đầu xa xương đòn giúp giảm đau và cải thiện chức năng vai ở giai đoạn theo dõi trung hạn ở những bệnh nhân kháng lại điều trị bảo tồn. Bác sĩ phẫu thuật của bạn sẽ xác định xem bạn có phải là ứng viên phù hợp hay không dựa trên các triệu chứng cụ thể và kết quả hình ảnh của bạn. Đối với một số người, việc loại bỏ mô xương đơn giản này là đủ để khôi phục sự thoải mái và vận động mà không cần đến các phương pháp tái tạo phức tạp hơn.
Những điều cần biết
Nếu bạn được chẩn đoán mắc viêm xương khớp do hao mòn ở khớp ức đòn (AC) nhưng không có triệu chứng đau, tình trạng này có khả năng sẽ duy trì như vậy. Ở 90% bệnh nhân, viêm xương khớp AC không triệu chứng vẫn không triệu chứng trong suốt 7 năm. Bạn không cần lo lắng về kết quả này nếu nó không gây phiền toái cho bạn. Việc thấy các dấu hiệu viêm khớp trên hình ảnh chẩn đoán ngay cả khi không có triệu chứng là điều phổ biến.
Nếu bạn có triệu chứng đau, tiên lượng phụ thuộc vào cách bạn quản lý triệu chứng này. Tiêm vào khớp mang lại tỷ lệ thành công sau 1 năm là 47%. Điều này có nghĩa là gần một nửa số bệnh nhân tìm thấy sự giảm đau kéo dài từ phương pháp điều trị này. Nếu việc tiêm không mang lại hiệu quả, bác sĩ phẫu thuật của bạn có thể khuyến nghị một thủ thuật loại bỏ một phần nhỏ của xương đòn. Việc cắt bỏ phần xa xương đòn hạn chế này giúp giảm đau và cải thiện chức năng vai ở giai đoạn theo dõi trung hạn đối với những bệnh nhân không đáp ứng với điều trị bảo tồn.
Bạn có thể mong đợi giảm đau ổn định nếu bạn chọn phẫu thuật. Cả hai kỹ thuật cắt bỏ mở và nội soi đều mang lại hiệu quả giảm đau này. Tuy nhiên, mỗi phương pháp đều có một bộ các biến chứng tiềm năng riêng biệt. Bác sĩ phẫu thuật của bạn sẽ thảo luận về phương pháp nào là tốt nhất cho giải phẫu và lối sống cụ thể của bạn.
Nếu bạn không điều trị viêm khớp AC có triệu chứng, nó có thể dai dẳng. Một số bệnh nhân trải qua tình trạng khó chịu kéo dài làm hạn chế các hoạt động hàng ngày. Nếu bạn trải qua các phẫu thuật vai khác, chẳng hạn như sửa chữa chóp xoay, viêm xương khớp AC không được điều trị có liên quan đến tỷ lệ thất bại thấp. Tuy nhiên, viêm xương khớp nói chung có liên quan đến kết quả lâm sàng cuối cùng kém hơn sau khi sửa chữa chóp xoay. Chóp xoay không liền hoặc bị rách lại cũng làm tăng nguy cơ phát triển viêm khớp này.
Đối với các trường hợp nghiêm trọng, đặc biệt nếu bạn đang thực hiện phẫu thuật thay khớp vai ngược, viêm xương khớp AC nghiêm trọng có liên quan đến gãy xương mỏm vai. Viêm xương khớp AC trên hình ảnh học là phổ biến ở những bệnh nhân đang thực hiện loại phẫu thuật này. Bác sĩ phẫu thuật của bạn sẽ theo dõi chặt chẽ các nguy cơ này.
Nhìn chung, diễn biến của viêm khớp AC rất khác nhau. Nó có thể thuyên giảm với chăm sóc bảo tồn, dai dẳng bất chấp điều trị, hoặc tiến triển chậm. Hầu hết bệnh nhân nhận thấy rằng các phương pháp điều trị nhắm mục tiêu mang lại sự cải thiện đáng kể về chức năng và sự thoải mái.
Khi nào cần gặp bác sĩ
Hãy gặp bác sĩ đa khoa nếu bạn có tình trạng đau dai dẳng không cải thiện khi nghỉ ngơi. Hãy yêu cầu được bác sĩ chuyên khoa khám lại nếu bạn nhận thấy tình trạng yếu hoặc mất ổn định ở khớp vai. Hãy tìm kiếm sự chăm sóc y tế nếu khớp bị khóa hoặc đột ngột mất lực. Hãy liên hệ với bác sĩ phẫu thuật nếu các triệu chứng ảnh hưởng đến giấc ngủ hoặc công việc của bạn. Tình trạng đau tăng lên đột ngột cũng là lý do để bạn tìm kiếm sự giúp đỡ. Lưu ý rằng tình trạng viêm xương khớp do hao mòn không có triệu chứng thường không gây đau trong bảy năm. Tuy nhiên, các vấn đề không được điều trị đôi khi có thể ảnh hưởng đến các phẫu thuật sửa chữa khớp vai khác. Bác sĩ của bạn sẽ kiểm tra các điểm đau và thảo luận xem liệu việc tiêm thuốc có thể giúp ích hay không. Việc đánh giá sớm đảm bảo bạn nhận được sự chăm sóc phù hợp trước khi tình trạng bệnh tiến triển nặng hơn.
Evidence & references
Overview
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Radiographic ACJ osteoarthritis is common in patients undergoing reverse shoulder arthroplasty [7].
- Severe acromioclavicular joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic AC osteoarthritis [8].
- Open and arthroscopic resection arthroplasty techniques have unique sets of potential complications that may be minimized with improved understanding of anatomy, biomechanics, and meticulous surgical technique [8].
- Limited distal clavicle excision reduced pain and improved shoulder function at midterm follow-up in patients with AC joint osteoarthritis resistant to conservative treatment [9].
- A distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary as all patients were equally satisfied with the outcome of preoperative acromioclavicular injection [6].
- Further characterisation of patients in whom mild arthroscopic findings of OA of the AC joint are clinically significant and warrant resection is needed [1].
- Acromioclavicular joint arthritis is not an indication for routine distal clavicle excision in arthroscopic rotator cuff repair [3].
- Clinicians should consider overreduction of the AC joint because it may lead to favorable radiological results [5].
- The authors recommend anatomic reconstruction procedures for the treatment of chronic complete AC dislocations [21].
Anatomy & Pathophysiology
- Anatomic techniques that address both coracoclavicular ligaments and the AC capsule are recommended to restore horizontal and vertical stability while allowing physiological rotation [10].
- None of the reconstruction strategies completely restored the shoulder girdle to its preinjured state [26].
- Kinematic changes resulting from AC joint dislocation could be a potential source of pain and dysfunction in the shoulder [27].
- Scapular and clavicular kinematics were affected in AC separation models [28].
- The position of the hook portion of a clavicle hook plate can predispose anatomic structures to post-operative complications of subacromial impingement and bony erosion [29].
- Future research should focus on addressing horizontal and rotational instability to restore native physiological and biomechanical properties of the AC joint [35].
- Coracoclavicular reconstruction with augmentation of the acromioclavicular joint provides improved horizontal stability compared to isolated coracoclavicular reconstruction [41].
- Adding a fixation of the AC joint minimizes lateral tilting of the scapula and maintains a more anatomic reposition result over time [45].
Classification
- Asymptomatic acromioclavicular osteoarthritis diagnosed by MRI remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated acromioclavicular joint osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Mild arthroscopic findings of acromioclavicular joint osteoarthritis may be clinically significant and warrant resection, but further characterization of such patients is needed [1].
- Severe acromioclavicular joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Radiographic acromioclavicular joint osteoarthritis is common in patients undergoing reverse shoulder arthroplasty [7].
- Osteolytic changes in the acromioclavicular joint seemed to be associated with incongruity of the joint but did not correlate with clinical results [11].
- The acromial center line to dorsal clavicle radiographic measurement and the use of the Alexander view provide a more realistic appreciation of true acromioclavicular joint displacement, especially in defining watershed cases (Rockwood types IIIA, IIB, and IV) [12].
- Evaluating the integrity of the capsuloligamentous structures stabilizing the acromioclavicular joint is reproducible and provides additional information on the severity of the injury [24].
- Injuries to the sternoclavicular joint are uncommon, and recognition and classification are critical to proper management to minimize long-term sequelae [16].
- Some persistent pain and osteoarthritis progression remain concerns in the arthroscopic revision of failed open anterior stabilization of the shoulder [4].
Clinical Presentation
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Preventive arthroscopic distal clavicle resection is not recommended in patients with radiological but asymptomatic ACJ arthritis [19].
- Further characterisation of patients in whom mild arthroscopic findings of OA of the AC joint are clinically significant and warrant resection is needed [1].
- A distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary, as all patients were equally satisfied with the outcome of preoperative acromioclavicular injection [6].
- Osteolytic changes seemed to be associated with incongruity of the AC joint, but did not correlate with clinical results [11].
- Additional research is needed to determine the main cause of pain in isolated acromioclavicular osteoarthritis and to compare clinical outcomes of intra-articular versus extra-articular injections [13].
- Risk factors for subsequent distal clavicle excision after rotator cuff repair include tenderness to palpation at the AC joint, female sex, and surgery on the dominant side [18].
- Subsequent distal clavicle excision was performed in 40% of cases with a combination of the three identified risk factors (tenderness to palpation, female sex, dominant side surgery) [18].
- Recurrence of the initial dislocation after arthroscopically assisted reduction appears to be related to the onset of degenerative ACJ arthropathy [14].
- Some persistent pain and osteoarthritis progression remain concerns in the revision of failed open anterior stabilization of the shoulder [4].
Investigations
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Preventive arthroscopic distal clavicle resection (DCR) is not recommended in patients with radiological but asymptomatic ACJ arthritis [19].
- Further characterization is needed to determine which patients with mild arthroscopic findings of AC joint OA are clinically significant and warrant resection [1].
- Radiographic ACJ osteoarthritis is common in patients undergoing reverse shoulder arthroplasty (RSA) [7].
- Severe ACJ osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Osteolytic changes in the AC joint seemed to be associated with incongruity but did not correlate with clinical results [11].
- Patients with edema on MRI were more likely to present with pain than patients without edema [43].
- Subchondral bone edema on histologic examination was more frequent in patients with pain [43].
- The outcomes of a preoperative AC injection suggest that a distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary, as all patients were equally satisfied with the outcome [6].
- Additional research is needed to determine the main cause of pain and to compare clinical outcomes of intra-articular versus extra-articular steroid injections for isolated AC osteoarthritis [13].
- Risk factors for subsequent distal clavicle excision after rotator cuff repair include tenderness to palpation at the AC joint, female sex, and surgery on the dominant side [18].
- Subsequent distal clavicle excision was performed in 40% of cases with a combination of the three identified risk factors (tenderness, female sex, dominant side) [18].
- The arthroscopic approach offers an advantage in diagnosing and treating occult intra-articular pathology during distal clavicle excision [20].
- Some persistent pain and osteoarthritis progression remain concerns in the revision of failed open anterior stabilization of the shoulder using arthroscopy [4].
- Evaluating the integrity of the capsuloligamentous structures stabilizing the AC joint is reproducible and provides additional information on injury severity, which may influence treatment decisions [24].
- The AC-DC measurement and use of the Alexander view provide a more realistic appreciation of true AC joint displacement, particularly in defining watershed cases (IIIA/IIB/IV) [12].
- Radiological failures were observed in 41% of cases in a prospective multicenter study of arthroscopic acute AC dislocation fixation [50].
Treatment
Non-Operative Management
- Conservative therapy is a valid initial treatment option for Rockwood Type V acromioclavicular dislocations [15].
- Non-operative reduction and stabilization is a valuable treatment option for acute high-grade acromioclavicular joint separations [33].
- Nonoperative treatment is helpful for most patients with painful conditions of the acromioclavicular joint, although those with osteolysis may need to modify their activities [44].
- Conservative and surgical treatments are both effective in the management of acromioclavicular joint osteoarthritis [17].
- Acromioclavicular injections offer a 1-year success rate of 47% in patients with acromioclavicular osteoarthritis [22].
- Additional research is needed to determine the main cause of pain and to compare clinical outcomes of intra-articular versus extra-articular steroid injections for isolated acromioclavicular osteoarthritis [13].
Operative Management
- Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic acromioclavicular osteoarthritis [8].
- Limited distal clavicle excision reduces pain and improves shoulder function at midterm follow-up in patients with acromioclavicular joint osteoarthritis resistant to conservative treatment [9].
- Untreated acromioclavicular joint osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Further characterization is needed to identify patients in whom mild arthroscopic findings of acromioclavicular joint osteoarthritis are clinically significant and warrant resection [1].
- Conversion to anatomic coracoclavicular ligament reconstruction shows similar clinical outcomes compared to successful non-operative treatment in chronic primary type III to V acromioclavicular joint injuries at a minimum 5-year follow-up [49].
- The authors recommend anatomic reconstruction procedures for the treatment of chronic complete acromioclavicular dislocations [21].
- Osteoarthritis is associated with poorer final clinical outcomes after rotator cuff repair, and an unhealed or re-torn cuff increases the risk of osteoarthritis [23].
Diagnostic Considerations
- A distinction between symptomatic and asymptomatic radiographic acromioclavicular osteoarthritis appears unnecessary, as all patients were equally satisfied with the outcome of preoperative acromioclavicular injection [6].
- Asymptomatic acromioclavicular osteoarthritis diagnosed by MRI remained asymptomatic in 90% of patients over a 7-year course [2].
- Some persistent pain and osteoarthritis progression remain concerns following arthroscopy in the revision of failed open anterior stabilization of the shoulder [4].
Complications
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Osteoarthritis is associated with poorer final clinical outcomes after rotator cuff repair [23].
- An unhealed or re-torn rotator cuff increases the risk of developing osteoarthritis [23].
- Severe AC joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Radiographic ACJ osteoarthritis is common in patients undergoing reverse shoulder arthroplasty [7].
- Some persistent pain and osteoarthritis progression remain concerns following arthroscopy in revision of failed open anterior stabilization of the shoulder [4].
- Recurrence of the initial dislocation after arthroscopically assisted reduction of acute AC joint dislocation appears to be related to the onset of degenerative ACJ arthropathy [14].
- Treatment of acute grade III and IV AC dislocations by synthetic ligament reconstruction carries a risk of significant early osteolysis [25].
- Open and arthroscopic AC joint reconstruction techniques have no differences in loss of reduction, complication rate, or revision rate [38].
- Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic AC osteoarthritis but each has a unique set of potential complications [8].
Recovery
- Asymptomatic acromioclavicular osteoarthritis diagnosed by MRI remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated acromioclavicular joint osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Limited distal clavicle excision for acromioclavicular joint osteoarthritis resistant to conservative treatment reduced pain and improved shoulder function at midterm follow-up [9].
- Acromioclavicular injections offer a 1-year success rate of 47% in patients with acromioclavicular osteoarthritis [22].
- A preoperative acromioclavicular injection study suggested that distinguishing between symptomatic and asymptomatic radiographic acromioclavicular osteoarthritis is unnecessary, as all patients were equally satisfied with the outcome [6].
- Osteolytic changes in the acromioclavicular joint seemed to be associated with incongruity but did not correlate with clinical results [11].
- Recurrence of initial acromioclavicular joint dislocation appears to be related to the onset of degenerative acromioclavicular joint arthropathy [14].
- Treatment of acute grade III and IV acromioclavicular dislocations using synthetic ligament reconstruction gave satisfactory results in terms of recovery of strength, but evolution is not risk-free due to the onset of significant early osteolysis [25].
- Arthroscopic coracoclavicular ligament reconstruction with double-bundle soft tissue allograft for chronic type V acromioclavicular dislocations showed sustained and statistically significant improvements in functional outcomes, high rates of return to sport, and maintenance of active-duty military status at minimum 10-year follow-up [39].
- Minimally invasive coracoclavicular ligament augmentation with a flip button/polydioxanone repair for total acromioclavicular joint dislocation revealed excellent radiologic and clinical results with no subluxations or dislocations noted in short-term follow-up [48].
- Some persistent pain and osteoarthritis progression remain concerns in the arthroscopic revision of failed open anterior stabilization of the shoulder [4].
- Type V acromioclavicular dislocations may be given a trial of conservative therapy [15].
Key Evidence
- [L2] Further characterisation of patients in whom mild arthroscopic findings of OA of AC joint are clinically significant and warrant resection is needed. [1] (10.1007/s00167-014-3114-2)
- [L2] Asymptomatic AC-OA remained asymptomatic in 90% over 7 years. [2] (10.1016/j.jse.2019.04.004)
- [L2] Untreated ACJ osteoarthritis, symptomatic or not, encountered during arthroscopic RCR is associated with a low percentage of failure. [3] (10.1007/s00167-020-06098-y)
- [L4] Some persistent pain and osteoarthritis progression remain concerns. [4] (10.1016/j.arthro.2009.04.073)
- [L3] Clinicians should consider overreduction of the AC joint because it may lead to favorable radiological results. [5] (10.1177/0363546519862850)
- [L4] The outcomes of this study seem to suggest that a distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary, as all patients were equally satisfied with the outcome. [6] (10.5397/cise.2023.00073)
- [L3] Radiographic ACJ osteoarthritis is common in patients undergoing RSA. [7] (10.1016/j.jseint.2021.11.008)
- [L5] Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic AC osteoarthritis, though each has a unique set of potential complications that may be minimized with improved understanding of anatomy, biomechanics, and meticulous surgical technique. [8] (10.1177/0363546513485359)
- [L4] Limited distal clavicle excision of patients with AC joint osteoarthritis resistant to conservative treatment reduced pain and improved shoulder function at midterm follow-up. [9] (10.1016/j.otsr.2016.01.008)
- [L5] Anatomic techniques that address both coracoclavicular ligaments and the AC capsule are recommended to restore horizontal and vertical stability while allowing physiological rotation. [10] (10.1016/j.arthro.2019.01.038)
- [L4] The AC-DC measurement and use of the Alexander view provides the clinician with a more realistic appreciation of true AC joint displacement, especially in defining watershed cases (ie, IIIA/IIB/IV) and may better inform the decision-making process regarding management options and recommendations. [12] (10.1016/j.jse.2019.12.014)
- [L4] Additional research is needed to determine the main cause of pain and compare clinical outcomes of intra-articular versus extra-articular injections. [13] (10.5397/cise.2023.00311)
- [L4] Recurrence of the initial dislocation appears to be related to onset of degenerative ACJ arthropathy. [14] (10.1016/j.otsr.2017.11.001)
- [L4] This suggests that Type V AC dislocations may be given a trial of conservative therapy. [15] (10.1177/2325967115s00017)
- [L1] Injuries to the SC joint are uncommon, and recognition and classification are critical to proper management to minimize long-term sequelae. [16] (10.1177/0363546513498990)
- [L4] Conservative and surgical treatments are both effective in acromioclavicular joint osteoarthritis management. [17] (10.1007/s00167-020-06377-8)
- [L3] Risk factors for subsequent DCE included tenderness to palpation at the AC joint, female sex, and surgery on the dominant side, with subsequent DCE performed in 40% of cases with a combination of these 3 factors. [18] (10.1177/2325967119844295)
- [L1] Preventive arthroscopic DCR is not recommended in patients with radiological but asymptomatic ACJ arthritis. [19] (10.1177/0363546514547254)
- [L1] The arthroscopic approach offers a unique advantage in diagnosing and treating occult intra-articular pathology. [20] (10.1016/j.jse.2006.10.006)
- [L4] The authors recommend this procedure for the treatment of chronic complete AC dislocations. [21] (10.1016/j.injury.2010.09.023)
- [L4] AC injections offer a 1-year success rate of 47%. [22] (10.5397/cise.2023.00031)
- [L4] Osteoarthritis is associated with poorer final clinical outcomes, and an unhealed or re-torn cuff increases the risk of osteoarthritis. [23] (10.1016/j.otsr.2017.03.007)
- [L1] Evaluating the integrity of the capsuloligamentous structures stabilizing the AC joint is reproducible and gives additional information on the severity of the injury, which might also influence the treatment decision. [24] (10.1016/j.jse.2020.10.026)
- [L4] Treatment of ACD by synthetic ligament reconstruction gave satisfactory results, notably in terms of recovery of strength, but evolution is not risk-free with onset of significant early osteolysis. [25] (10.1016/j.otsr.2010.06.004)
- [L5] Although each technique was able to restore different elements of the joint kinematics, none of the strategies completely restored the shoulder girdle to its preinjured state. [26] (10.1177/03635465221095231)
- [L5] The kinematic changes could be a potential source of pain and dysfunction in the shoulder with AC joint dislocation. [27] (10.1177/0363546512458571)
- [L5] Scapular and clavicular kinematics were affected in AC separation models. [28] (10.1016/j.jse.2013.01.004)
- [L5] The observed frequency of hook contact with surrounding subacromial structures in a static shoulder confirms that the position of the hook portion of the implant can predispose anatomic structures to the post-operative complications of subacromial impingement and bony erosion. [29] (10.1016/j.injury.2009.12.012)
- [L4] Non-operative reduction and stabilization of high-grade AC joint separations seems to be a valuable treatment option. [33] (10.1007/s00402-020-03630-0)
- [L5] Future research should focus on addressing horizontal and rotational instability, to restore native physiological and biomechanical properties of the AC joint. [35] (10.1186/s12891-022-05935-0)
- [L1] Open and arthroscopic AC joint reconstruction techniques have no differences in loss of reduction, the complication rate, and the revision rate based on the available literature. [38] (10.1177/0363546518795147)
- [L4] Outcomes after arthroscopic CC reconstruction for chronic, type V AC dislocations in an active-duty military patient population show sustained and statistically significant improvements in functional outcomes as well as high rates of return to sport and maintenance of active-duty military status at long-term follow-up. [39] (10.1016/j.arthro.2025.05.008)
- [L1] Coracoclavicular reconstruction with augmentation of the acromioclavicular joint has been shown to provide improved horizontal stability in both biomechanical and clinical studies compared to isolated coracoclavicular reconstruction. [41] (10.1007/s00167-018-5152-7)
- [L4] Patients with edema on MRI were more likely to present pain than patients without edema, and subchondral bone edema on histologic examination was more frequent in patients with pain. [43] (10.1016/j.jseint.2020.03.007)
- [L5] Nonoperative treatment is helpful for most patients, although those with osteolysis may have to modify their activities. [44] (10.5435/00124635-199905000-00004)
- [L3] The presented data suggest adding a fixation of the AC joint to minimize lateral tilting of the scapula and maintain a more anatomic reposition result over time. [45] (10.1007/s00402-021-03761-y)
- [L4] The short-term follow-up of 15 recently operated patients reveals excellent radiologic and clinical results, with no subluxations or dislocations of the acromioclavicular joint noted. [48] (10.1016/j.arthro.2006.12.015)
- [L4] At a minimum 5-year follow-up, patients with successful non-operative treatment for type III-V ACJ injuries achieved similar clinical outcomes compared to those who were converted to ACCR. [49] (10.1007/s00167-020-06159-2)
- [L4] Surgery for AC dislocations is difficult with radiological results that must still be improved, as radiological failures were observed in 41% of cases. [50] (10.1016/j.otsr.2015.09.012)
References
[1] Outcome of distal clavicle resection in patients with acromioclavicular joint osteoarthritis and full‐thickness rotator cuff tear. Knee Surgery, Sports Traumatology, Arthroscopy. 2014. DOI: 10.1007/s00167-014-3114-2 [2] Seven-year course of asymptomatic acromioclavicular osteoarthritis diagnosed by MRI. Journal of Shoulder and Elbow Surgery. 2019. DOI: 10.1016/j.jse.2019.04.004 [3] Acromioclavicular joint arthritis is not an indication for routine distal clavicle excision in arthroscopic rotator cuff repair. Knee Surgery, Sports Traumatology, Arthroscopy. 2020. DOI: 10.1007/s00167-020-06098-y [4] The Role of Arthroscopy in Revision of Failed Open Anterior Stabilization of the Shoulder. Arthroscopy. 2009. DOI: 10.1016/j.arthro.2009.04.073 [5] Factors Predicting the Outcome After Arthroscopically Assisted Stabilization of Acute High-Grade Acromioclavicular Joint Dislocations. The American Journal of Sports Medicine. 2019. DOI: 10.1177/0363546519862850 [6] Diagnostic value of a preoperative acromioclavicular injection for symptomatic acromioclavicular osteoarthritis: a retrospective study of cross-sectional midterm outcomes. Clinics in Shoulder and Elbow. 2024. DOI: 10.5397/cise.2023.00073 [7] Severe acromioclavicular joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty. JSES International. 2022. DOI: 10.1016/j.jseint.2021.11.008 [8] Degenerative Joint Disease of the Acromioclavicular Joint. The American Journal of Sports Medicine. 2013. DOI: 10.1177/0363546513485359 [9] Limited distal clavicle excision of acromioclavicular joint osteoarthritis. Orthopaedics & Traumatology: Surgery & Research. 2016. DOI: 10.1016/j.otsr.2016.01.008 [10] Editorial Commentary: Why We Have To Respect The Anatomy In Acromioclavicular Joint Surgery And Why Clinical Shoulder Scores Might Not Give Us The Information We Need!. Arthroscopy. 2019. DOI: 10.1016/j.arthro.2019.01.038 [11] 10.1016-0020-1383-83-90092-x. n.d.. [12] Improved identification of unstable acromioclavicular joint injuries in a clinical population using the acromial center line to dorsal clavicle radiographic measurement. Journal of Shoulder and Elbow Surgery. 2020. DOI: 10.1016/j.jse.2019.12.014 [13] Isolated acromioclavicular osteoarthritis and steroid injection. Clinics in Shoulder and Elbow. 2023. DOI: 10.5397/cise.2023.00311 [14] Arthroscopically assisted reduction of acute acromioclavicular joint dislocation using a single double-button device: Medium-term clinical and radiological outcomes. Orthopaedics & Traumatology: Surgery & Research. 2018. DOI: 10.1016/j.otsr.2017.11.001 [15] Successful Conservative Therapy in Rockwood Type V Acromioclavicular Dislocations. Orthopaedic Journal of Sports Medicine. 2015. DOI: 10.1177/2325967115s00017 [16] Instability and Degenerative Arthritis of the Sternoclavicular Joint. The American Journal of Sports Medicine. 2013. DOI: 10.1177/0363546513498990 [17] No differences between conservative and surgical management of acromioclavicular joint osteoarthritis: a scoping review. Knee Surgery, Sports Traumatology, Arthroscopy. 2021. DOI: 10.1007/s00167-020-06377-8 [18] Preoperative Factors Associated With Subsequent Distal Clavicle Resection After Rotator Cuff Repair. Orthopaedic Journal of Sports Medicine. 2019. DOI: 10.1177/2325967119844295 [19] Is Arthroscopic Distal Clavicle Resection Necessary for Patients With Radiological Acromioclavicular Joint Arthritis and Rotator Cuff Tears?. The American Journal of Sports Medicine. 2014. DOI: 10.1177/0363546514547254 [20] Arthroscopic versus open distal clavicle excision: Comparative results at six months and one year from a randomized, prospective clinical trial. Journal of Shoulder and Elbow Surgery. 2007. DOI: 10.1016/j.jse.2006.10.006 [21] Surgical treatment of chronic acromioclavicular dislocation: Comparison between two surgical procedures for anatomic reconstruction. Injury. 2010. DOI: 10.1016/j.injury.2010.09.023 [22] Mid- to long-term success rate and functional outcomes of acromioclavicular injections in patients with acromioclavicular osteoarthritis. Clinics in Shoulder and Elbow. 2023. DOI: 10.5397/cise.2023.00031 [23] Osteoarthritis after rotator cuff repair: A 10-year follow-up study. Orthopaedics & Traumatology: Surgery & Research. 2017. DOI: 10.1016/j.otsr.2017.03.007 [24] The ligamentous injury pattern in acute acromioclavicular dislocations and its impact on clinical and radiographic parameters. Journal of Shoulder and Elbow Surgery. 2021. DOI: 10.1016/j.jse.2020.10.026 [25] Acute grade III and IV acromioclavicular dislocations: Outcomes and pitfalls of reconstruction procedures using a synthetic ligament. Orthopaedics & Traumatology: Surgery & Research. 2010. DOI: 10.1016/j.otsr.2010.06.004 [26] Differences between Coracoclavicular, Acromioclavicular, or Combined Reconstruction Techniques on the Kinematics of the Shoulder Girdle. The American Journal of Sports Medicine. 2022. DOI: 10.1177/03635465221095231 [27] The Function of the Acromioclavicular and Coracoclavicular Ligaments in Shoulder Motion. The American Journal of Sports Medicine. 2012. DOI: 10.1177/0363546512458571 [28] Acromioclavicular joint ligamentous system contributing to clavicular strut function: a cadaveric study. Journal of Shoulder and Elbow Surgery. 2013. DOI: 10.1016/j.jse.2013.01.004 [29] Subacromial morphometric assessment of the clavicle hook plate. Injury. 2010. DOI: 10.1016/j.injury.2009.12.012 [33] Can an acute high-grade acromioclavicular joint separation be reduced and stabilized without surgery? A surgeon’s experience. Archives of Orthopaedic and Trauma Surgery. 2020. DOI: 10.1007/s00402-020-03630-0 [35] Current concepts in acromioclavicular joint (AC) instability – a proposed treatment algorithm for acute and chronic AC-joint surgery. BMC Musculoskeletal Disorders. 2022. DOI: 10.1186/s12891-022-05935-0 [38] Current Concepts in the Operative Management of Acromioclavicular Dislocations: A Systematic Review and Meta-analysis of Operative Techniques. The American Journal of Sports Medicine. 2018. DOI: 10.1177/0363546518795147 [39] Arthroscopic Coracoclavicular Ligament Reconstruction With Double‐Bundle Soft Tissue Allograft for Chronic Type V Acromioclavicular Dislocations Shows Excellent Patient Outcomes and Return to Duty and Sport at Minimum 10‐Year Follow‐Up. Arthroscopy. 2025. DOI: 10.1016/j.arthro.2025.05.008 [41] Acromioclavicular joint augmentation at the time of coracoclavicular ligament reconstruction fails to improve functional outcomes despite significantly improved horizontal stability. Knee Surgery, Sports Traumatology, Arthroscopy. 2018. DOI: 10.1007/s00167-018-5152-7 [43] Histologic and magnetic resonance image evaluation in acromioclavicular joint osteoarthritis. JSES International. 2020. DOI: 10.1016/j.jseint.2020.03.007 [44] Painful Conditions of the Acromioclavicular Joint. Journal of the American Academy of Orthopaedic Surgeons. 1999. DOI: 10.5435/00124635-199905000-00004 [45] Additional acromioclavicular cerclage limits lateral tilt of the scapula in patients with arthroscopically assisted coracoclavicular ligament reconstruction. Archives of Orthopaedic and Trauma Surgery. 2021. DOI: 10.1007/s00402-021-03761-y [48] Minimally Invasive Coracoclavicular Ligament Augmentation With a Flip Button/Polydioxanone Repair for Treatment of Total Acromioclavicular Joint Dislocation. Arthroscopy. 2007. DOI: 10.1016/j.arthro.2006.12.015 [49] Conversion to anatomic coracoclavicular ligament reconstruction (ACCR) shows similar clinical outcomes compared to successful non‐operative treatment in chronic primary type III to V acromioclavicular joint injuries. Knee Surgery, Sports Traumatology, Arthroscopy. 2020. DOI: 10.1007/s00167-020-06159-2 [50] Complication rates and types of failure after arthroscopic acute acromioclavicular dislocation fixation. Prospective multicenter study of 116 cases. Orthopaedics & Traumatology: Surgery & Research. 2015. DOI: 10.1016/j.otsr.2015.09.012





