EnFix Biological Scaffold Info
Last reviewed
Also on YouTube.
Video transcript
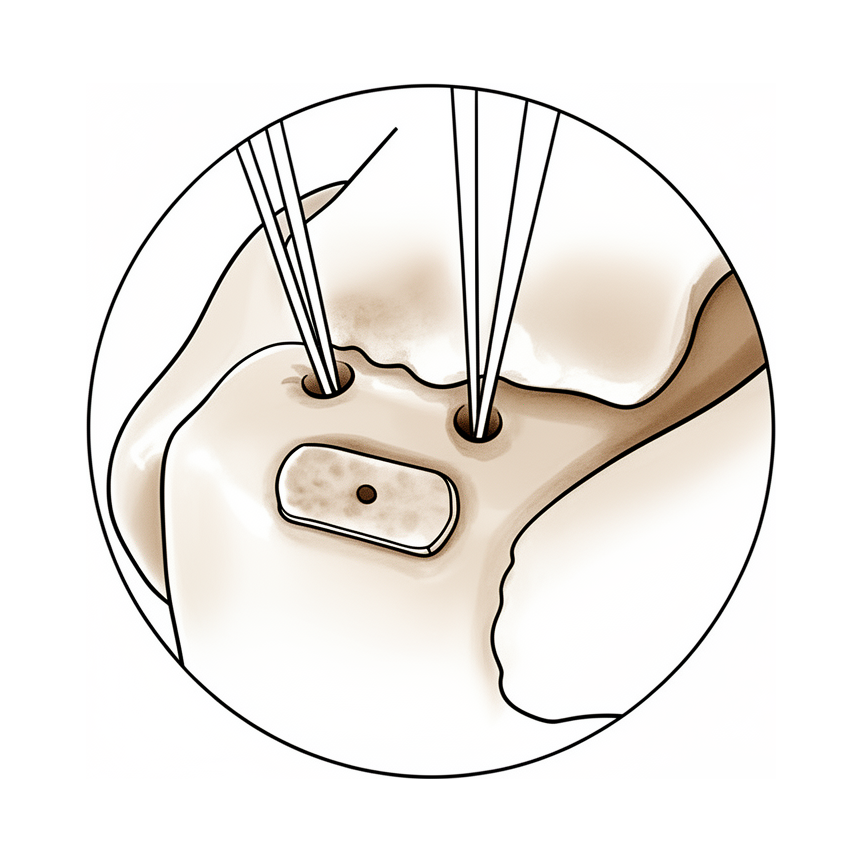
The cuff has been mobilised, and medial row anchors have been placed at the articular margin. The sutures have been passed, but not yet secured laterally. These are the anchors, which I'm identifying prior to choosing the location for the EnFix. I'm using a punch to create a socket for the implant. The EnFix is made from demineralised cortical bone fibres, brought into the joint on its introducer through the anchor portal just lateral to the edge of the acromion. The EnFix is now seated in its socket in the footprint. Next, the sutures will be retrieved and secured to lateral row anchors, which will bring the tendon over the EnFix.
If we used a biological scaffold during your rotator cuff repair, you may have seen the name EnFix on your paperwork and wondered what it is. This page explains it in plain terms: what the scaffold is, the problem it is meant to help with, and, just as importantly, what we do and don't yet know about it. It is an add-on to a standard rotator cuff repair, not a different operation, and it does not change how you recover.
The weak spot in a cuff repair
A rotator cuff repair reattaches a torn tendon back onto the top of the arm bone. The tricky part is not the stitches: it is getting the tendon to truly heal back onto the bone. Tendon and bone meet at a special junction (your surgeon may call it the footprint, or the enthesis). In nature this is a gradual transition zone that works like a shock absorber, blending the flexible tendon into the hard bone so that load passes smoothly from one to the other.
The problem is that, once it is torn, the body does not rebuild that elegant transition zone. It tends to fill the gap with ordinary scar tissue, which is weaker than the original attachment. Sometimes that scar does not fully bridge tendon to bone, and the repair can pull away: a re-tear. This is more likely with larger tears, older tendons, and poorer tissue quality, and most re-tears happen in the first few months after surgery while healing is still getting established. Helping that one spot heal properly is the whole goal.
What EnFix is
EnFix is a small implant placed at the footprint, between the tendon and the bone (not as a patch laid over the top of the repair). The idea is to put helpful biology exactly where healing needs to happen.
It is made from demineralised cortical bone fibre, human bone that has been processed so that the hard mineral is removed, leaving the natural fibres and the body's own healing signals behind. It contains no added drugs or chemicals. Because it comes from donated human tissue (an allograft), it is worth knowing that such tissue is carefully screened and processed to remove cells and reduce any risk of infection or rejection; demineralised bone has a long, well-established safety record and is used widely in other areas of surgery, such as the spine.
What we hope it does
The thinking behind EnFix is that it acts as both a scaffold (a natural framework for your own cells to grow into) and a biological signal that encourages those cells to rebuild a proper tendon-to-bone junction rather than plain scar. In short, the hope is that it helps the repair heal more like the original attachment, and so lowers the chance of a re-tear, particularly in the bigger or more difficult tears where healing is least reliable.
What is known so far
It is important to be honest about the evidence, because this is a newer technology. In laboratory and animal studies, repairs supported with this kind of demineralised bone fibre have healed with more organised, more natural tendon-to-bone tissue than repairs without it. Early studies in patients have been encouraging, and our own early results have been promising, but the numbers are still small and the follow-up is still short, so longer follow-up is needed before anyone can say with confidence how much difference it makes. Larger, more formal studies are underway to answer exactly that.
We will always be straight with you about this: EnFix is a well-reasoned, biologically sensible addition with promising early signs, not a guaranteed fix.
What it means for you
In practice, using the scaffold:
- Adds only a couple of minutes to the operation and uses your existing repair technique: there is no separate procedure and no extra incision.
- Does not change your recovery or rehabilitation. Your sling, your movement restrictions, and your physiotherapy are guided by the repair itself, exactly as they would be without it. The scaffold supports healing; it does not replace the need to protect the repair and do your rehab.
- Is one part of giving your repair the best chance to heal, alongside the quality of the repair, your own tissue, and how closely you follow your rehab programme.
When to ask
If you are unsure whether a scaffold was used in your repair, or you would like to talk through what it means for your particular tear, just ask at your next appointment and we are happy to go through it. And the usual advice after any cuff repair still applies: contact us if you have increasing pain that your medication isn't controlling, a wound that becomes red, hot or starts leaking, or a fever, and seek urgent care for sudden chest pain or breathlessness.





