ஃப்ளெக்சர் ஷீத் காங்லியன் எக்ஸிஷன்
Patients › Rehabilitation
ஒரு விரலின் அடிப்பகுதியில் ஒரு ஃப்ளெக்சர் டெண்டன் ஷீட் கேங்க்லியன் (வோலார் ரெட்டினாகுலர் சிஸ்ட்) பிரித்தெடுக்கப்பட்ட பிறகு விரைவான, இயக்கம் தலைமையிலான மீட்பு திட்டம், ஒரு சிறிய கைப்பையை காக்கும் போது நீங்கள் சில நாட்களுக்குள் மென்மையான விரல் இயக்கத்தைத் தொடங்குவீர்கள், பின்னர் காயம் குடியேறும்போது ஸ்கார் பராமரிப்பு மற்றும் பிடியைச் சேர்க்கவும்.
இந்த நெறிமுறை ஒரு சிறிய அறுவை சிகிச்சை பிறகு உங்கள் மீட்பு வழிகாட்டுகிறது நெகிழ்வுத் தாள் காங்லியன், ஒரு விரலின் அடிப்பகுதியில் ஒரு உறுதியான சிறுநீர்ப்பை கையின் உள்ளங்கை பக்கத்தில், டாக்டர் Kieran Hirpara உடன் மேட்டர் தனியார் மருத்துவமனை Rockhampton. அது உங்கள் வீட்டில் உடற்பயிற்சி திட்டம் தொடங்குகிறது, கட்டமைக்கப்பட்ட மருத்துவ நெறிமுறை எழுதப்பட்ட தொடர்ந்து உங்கள் கை சிகிச்சையாளர்; இந்த பக்கத்தை அல்லது அதன் PDF ஐ உங்கள் முதல் சிகிச்சை வருகைக்கு எடுத்துச் செல்லுங்கள், இதனால் உங்கள் மறுவாழ்வு ஒருங்கிணைந்ததாக இருக்கும். உங்கள் கை சிகிச்சையாளர் உங்கள் மீட்பு எவ்வாறு முன்னேறுகிறது என்பதைப் பொறுத்து திட்டத்தை சரிசெய்யலாம்.
அறுவை சிகிச்சைக்குப் பிறகு உங்கள் காயத்தைப் பற்றி ஏதேனும் கவலைகள் இருந்தால், அறைகளைத் தொடர்பு கொள்ளுங்கள். காயத்தின் புகைப்படத்தை எடுத்து அதை மதிப்பாய்வு செய்ய மின்னஞ்சல் அனுப்புவது பெரும்பாலும் உதவியாக இருக்கும்.
எதிர்பார்ப்பது என்ன
ஒரு ஃப்ளெக்ஸர் ஷீட் கங்லியன் (இது ஒரு வால்வர் ரெட்டினாகுலர் சிஸ்டு) என்பது ஒரு சிறிய, உறுதியான, பெரும்பாலும் மென்மையான கட்டி, வழக்கமாக ஒரு சில மில்லிமீட்டர் அகலம் மட்டுமே, இது நெகிழ்வு தசைகள் வழியாக செல்கிறது, கைப்பையில் உள்ள ஒரு விரலின் அடிப்பகுதியில் (பொதுவாக A1 புல்லி என்று அழைக்கப்படும் உறுதியான பட்டைக்கு மேல், கைப்பையை சந்திக்கும் மடிப்பில்). இது கட்டிக்கு இணைக்கப்பட்டுள்ளது மற்றும் விரலை வளைக்கும்போது நகராது. இது முற்றிலும் நன்மை பயக்கும் (புற்றுநோயற்ற) கட்டி, மற்றும் கை மற்றும் மணிக்கட்டில் மிகவும் பொதுவான கட்டிகளில் ஒன்றாகும்.
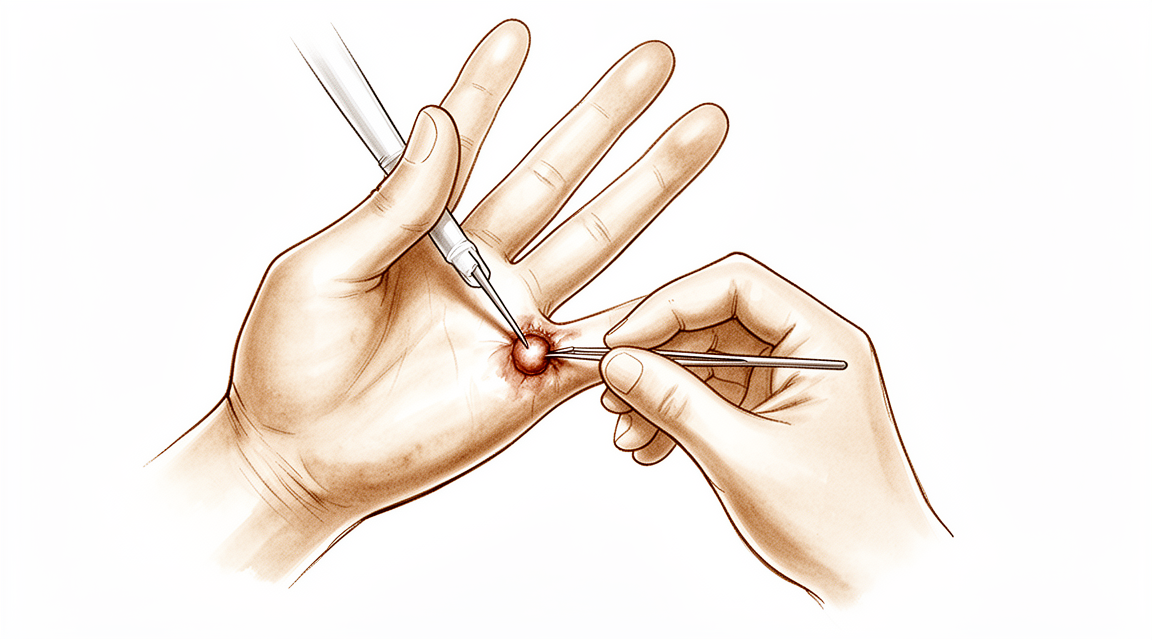
ஆபரேஷன் ஒரு சிறிய நாள் வழக்கு அறுவை சிகிச்சைகைத்தடியில் ஒரு குறுகிய சிக்-சாக் வெட்டு மூலம், டாக்டர் ஹிர்பாரா சிறுநீரகத்தை நீக்குகிறார். அது வளர்ந்த இடுப்பு மூடியின் ஒரு சிறிய கம்பளத்துடன். விரலின் இருபுறமும் ஓடும் இரண்டு சிறிய நரம்புகள் மற்றும் இரத்த நாளங்கள் கவனமாக பாதுகாக்கப்படுகின்றன. சரி செய்யப்படாதது: அதைத் திறந்து வைப்பது வேண்டுமென்றே செய்யப்படுகிறது, விரலை பலவீனப்படுத்தாது. தோல் தையல்களால் மூடப்படுகிறது.
ஏனெனில் விரலின் உள்ளே உள்ள எதையும் அது குணமடையும் போது பாதுகாக்க வேண்டியதில்லை, இது ஒரு விரைவான மீட்பு: வாரங்கள், மாதங்கள் அல்ல. திட்டம் எளிதானது: சிறிய கை காயத்தை பாதுகாக்கவும், வீக்கத்தைக் கட்டுப்படுத்தவும், மற்றும் சில நாட்களுக்குள் மென்மையான விரல் இயக்கத்தைத் தொடங்கவும், இதனால் விரல் இறுக்கமடையாது மற்றும் தசைகள் குணமடையும் வடுக்களில் ஒட்டிக்கொள்ளாது. காயம் குணமடைந்தவுடன், வடுக்கள் மசாஜ் மற்றும் உணர்திறன் குறைப்பு பகுதியை சரிசெய்து, பிடியை மீண்டும் கட்டியெழுப்புகிறது. சிறிய தோல் நரம்புகள் மீண்டு வருவதால் காயத்தைச் சுற்றி ஒரு சிறிய புண் அல்லது மென்மையானது ஆரம்பத்தில் பொதுவானது, மேலும் இது பொதுவாக அடுத்த வாரங்களில் குடியேறுகிறது.
முன்னெச்சரிக்கைகள் மற்றும் வரம்புகள்
- காயம் குணமாகும் வரை மற்றும் தையல்கள் வெளியேறும் வரை (பொதுவாக 10 14 நாட்கள்) பிளாஸ்டர் மற்றும் பொதுவாக ஸ்பிளண்ட் இல்லை, ஒரு மென்மையான பிளாஸ்டிங் மட்டுமே.
- செய் முதல் சில நாட்களில் மென்மையான விரல் இயக்கத்தைத் தொடங்குங்கள் (வளைத்தல், நேராக்குதல் மற்றும் இடுப்பு சறுக்கல்) விறைப்பு மற்றும் இடுப்பு ஒட்டாமல் தடுக்க.
- செய் கையை உயர்த்தி வைத்து, தினசரி இலகுவான வேலைகளைச் செய்ய அதைப் பயன்படுத்துங்கள்.
- செய் இல்லை காயம் குணமடையும் வரை (சுமார் இரண்டு முதல் மூன்று வாரங்கள்) பலமான பிடிப்பு, தூக்குதல் அல்லது வலுவான கிள்ளுதல் ஆகியவற்றை செய்யுங்கள்.
- செய் இல்லை காயம் முழுமையாக குணமடையும் வரை வலியை மசாஜ் செய்யவும் அல்லது கையை ஊறவைக்கவும்.
- செய் இல்லை பொதுவாக முதல் வாரத்தில், நீங்கள் பாதுகாப்பாக சக்கரத்தை பிடிப்பதை தடுக்கும் போதே வாகனம் ஓட்டுங்கள்.
காயம், வீக்கம் மற்றும் வடுக்கள் மேலாண்மை, நடைமுறையில் பார்க்க காயம் பராமரிப்பு வழிகாட்டல்.
உங்கள் பயிற்சிகள்
இவை உங்கள் கையேட்டில் உள்ள பயிற்சிகள். டாக்டர் ஹிர்பரா மற்றும் உங்கள் கை சிகிச்சையாளரின் வழிகாட்டுதலின்படி மட்டுமே அவற்றைத் தொடங்குங்கள், உங்களுக்கு வழங்கப்பட்ட வரம்புகளுக்குள் இருங்கள். ஆரம்ப பயிற்சிகள் (மென்மையான குத்து மற்றும் நேராக்குதல், இடுப்பு நெகிழ்வுகள் மற்றும் வீக்கக் கட்டுப்பாடு) விரலை நகர்த்துவதையும், இடுப்புகளை மெதுவாக நகர்த்துவதையும் முதல் சில நாட்களுக்குள் வைத்திருங்கள், இது மென்மையான மீட்புக்கு மிக முக்கியமான விஷயம். காயம் முழுமையாக குணமடைந்தவுடன் ஸ்கார் மசாஜ் மற்றும் உணர்திறன் குறைப்பு தொடங்குகிறது, மேலும் பிடியை வலுப்படுத்துவது சற்று பிந்தைய கட்டத்திற்கு சொந்தமானது (சுமார் இரண்டு முதல் மூன்று வாரங்கள் வரை). காயம் மீது கூர்மையான வலியை ஏற்படுத்தும் எதையும் நிறுத்துங்கள்.
உங்கள் மருத்துவ நெறிமுறை
இந்த பக்கத்தின் மீதமுள்ள பகுதி ஒரு ஃப்ளெக்சர் ஷீட் கேங்க்லியன் (வோலார் ரெட்டினாகுலர் சிஸ்ட்) பிரித்தெடுத்த பிறகு மறுவாழ்வுக்கான படிநிலை மருத்துவ நெறிமுறை ஆகும். இந்த பிரிவு உங்கள் கை சிகிச்சையாளருக்கு வழங்கப்பட வேண்டும், மேலும் ஒவ்வொரு கட்டமும் என்ன நடக்கிறது என்பதற்கான எளிய ஆங்கில விளக்கத்துடன் தொடங்குகிறது. அறுவை சிகிச்சை, சரிசெய்தல் அல்ல: இடுப்பு மூட்டை திறந்த நிலையில் உள்ளது மற்றும் பாதுகாக்க எந்த கட்டமைப்பும் இல்லை. ஆரம்பகால இயக்கம் காயம் பாதுகாப்பு, வீக்கம் கட்டுப்பாடு, இடுப்பு ஒட்டுதல் தடுக்க இடுப்பு சறுக்கல், மற்றும் வடுக்கள் / desensitization வேலை சுற்றி கட்டப்பட்ட பாதை, பாதுகாக்கப்படாத immobilisation.
சிகிச்சைக்கு முன்னர், அறுவை சிகிச்சை அறிக்கை மற்றும் கடந்தகால மருத்துவ வரலாறு ஆகியவற்றை சரிபார்த்து, சிகிச்சையளிக்கும் அறுவை சிகிச்சையாளருடன் தொடர்பு கொள்ளுங்கள். சம்பந்தப்பட்ட எண், மூட்டு அறுவை சிகிச்சையின் அளவு மற்றும் டிஜிட்டல் நரம்பியல் மூட்டுகளின் ஒருமைப்பாடு குறித்து. டாக்டர் ஹிர்பாராவின் அறுவை சிகிச்சை A1 / அருகிலுள்ள மூட்டு மீது ஒரு ப்ரூனர் (சிக்-சாக்) பால்மர் வெட்டு வழியாக உள்ளது, மூட்டுக் கம்பியுடன் சிஸ்டை நீக்குகிறது; மூட்டு சரிசெய்யப்படவில்லை மற்றும் மென்மையான உடைக்கு அப்பால் இயலாமை இல்லை. தற்காலிக டிஜிட்டல்-நெர்வ் பாராஸ்டீசியா பொதுவானது மற்றும் சுய-வரையறை.
கட்டம் I காயம் பாதுகாப்பு மற்றும் ஆரம்ப இயக்கம் (வாரம் 0 முதல் ~ 1)
முதல் வாரம் சிறு கைப்பையில் உள்ள காயத்தை பாதுகாக்கிறது மற்றும் விரலை விரைவாக நகர்த்துகிறது, இதனால் அது இறுக்கமடையாது அல்லது இடுப்பு ஒட்டுதல்களை உருவாக்காது. தடிமனான மென்மையான பேண்டரிங் ஸ்பிளின்ட் இல்லாமல், மென்மையான சுறுசுறுப்பான விரல் இயக்கத்துடன் சில நாட்களில் தொடங்கியது.
உங்கள் கை சிகிச்சையாளருக்கு:
கல்வி மற்றும் முன்னெச்சரிக்கைகள் - மென்மையான கனமான உடைகள் மட்டுமே, தையல் இல்லை; தையல்கள் வெளியேறும் வரை சுத்தமாகவும் உலர்ந்ததாகவும் வைத்திருக்கவும் (~ நாள் 1014) - கனமான சுமைகளிலிருந்து காயத்தைப் பாதுகாக்கவும்; இலகுவான சுமை இல்லாத கையை வசதியாகப் பயன்படுத்தவும் - ஆலோசனை தற்காலிக டிஜிட்டல்- நரம்பு பாராஸ்டீசியா / அதிக உணர்திறன் காயம் சுற்றி பொதுவான மற்றும் சுய வரையறுக்கப்பட்ட
நிர்வாகம் - காயம்: பரிந்துரைப்படி அறுவை சிகிச்சை; தொற்றுநோயை கண்காணிக்கவும் - வீக்கம்: இதய மட்டத்திற்கு மேலே உயர்வு, மென்மையான விரல் உந்தி, தேவைக்கேற்ப பனி - பயிற்சிகள்: மென்மையான செயலில் விரல் AROM (மென்மையான கலப்பு முஷ்டி மற்றும் முழு நீட்டிப்பு) மற்றும் இடுப்பு சறுக்கல்கள் (குத்து / முஷ்டி / நேராக) சில நாட்களுக்குள் தொடங்கியது; ஈடுபடாத விரல்கள், கட்டைவிரல் மற்றும் மணிக்கட்டு ஆகியவற்றின் செயலில் இயக்கம்; இலகுவான செயல்பாட்டு பயன்பாடு
முன்னேற்றத்திற்கான அளவுகோல்கள் - காயம் குடியேறுதல், தொற்று இல்லை; வசதியான ஆரம்ப செயலில் வளைவு; காயம் அனுமதிக்கும் போது முழு செயலில் / மென்மையான செயலற்ற இயக்கத்திற்கு தயாராக உள்ளது
கட்டம் II முழு இயக்கம், வீக்கம் மற்றும் வடுக்கள் வேலை (வாரம் ~ 1 முதல் 3)
ஏறக்குறைய ஒரு வாரத்திலிருந்து, இயக்கம் முழு செயலில் மற்றும் மென்மையான செயலற்ற வரம்பிற்கு (முழு குத்து மற்றும் முழு நீட்டிப்பு) முன்னேறுகிறது மற்றும், காயம் முழுமையாக குணமடைந்தவுடன் மற்றும் தையல்கள் வெளியே வந்தவுடன், ஸ்கார் மசாஜ் மற்றும் உணர்திறன் குறைப்பு தொடங்குகிறது. வீக்கம் கட்டுப்பாடு தொடர்கிறது.
உங்கள் கை சிகிச்சையாளருக்கு:
மதிப்பீடுகள் - செயலில் மற்றும் செயலற்ற விரல் ROM (முழு குத்து மற்றும் முழு நீட்டிப்பு இலக்கு); காயம் / வடுக்கள் நிலை; வீக்கம்; டிஜிட்டல்-நரம்பு உணர்திறன்
கல்வி மற்றும் முன்னெச்சரிக்கைகள் - முன்னேற்றம் முழு செயலில் மற்றும் மென்மையான செயலற்ற விரல் இயக்கம் வசதியளிக்கும் அளவு - தொடங்கு காயம் முற்றிலுமாக குணமடைந்த பிறகு மட்டுமே வடு மசாஜ் மற்றும் உணர்திறன் குறைப்பு - காயம் குணமடையும் வரை கடுமையாகப் பிடிப்பதைத் தவிர்க்கவும்
நிர்வாகம் - உடற்பயிற்சிகள்: முழு கலப்பு முஷ்டி மற்றும் முழு நீட்டிப்பு; தொடர்ச்சியான இடுப்பு சறுக்கல்கள்; எந்தவொரு மீதமுள்ள இறுக்கத்திற்கும் மென்மையான செயலற்ற நீட்சி - வடுக்கள்: வடுக்கள் மசாஜ் + வண்ணமயமாக்கப்பட்ட உணர்திறன் குறைப்பு குணமடைந்தவுடன்; தேவைக்கேற்ப வீக்கத்தை நிர்வகித்தல்
முன்னேற்றத்திற்கான அளவுகோல்கள் - முழுமையான, வலி இல்லாத செயலில் இயக்கம்; காயம் குணமடைந்தது; குணமடைந்த வடு; ஏற்ற தயாராக உள்ளது
கட்டம் III வலுவூட்டல் மற்றும் திரும்புதல் (வாரம் ~ 3 முதல் 6)
காயம் குணமடைந்து இயக்கம் முழுமையாக இருக்கும்போது (சுமார் மூன்று வாரங்கள்), பிடிப்பு மற்றும் பிஞ்ச் வலுவூட்டல் பெரும்பாலான நோயாளிகள் நான்கு முதல் ஆறு வாரங்களுக்குள் முழுமையான செயல்பாட்டிற்குத் திரும்புகிறார்கள், சுமார் இரண்டு மாதங்களுக்குப் பிறகு வழக்கமான பின்தொடர்தலுடன்.
உங்கள் கை சிகிச்சையாளருக்கு:
மதிப்பீடுகள் - மற்ற பக்கத்திற்கு எதிராக பிடியுங்கள்; மீதமுள்ள வடு அல்லது உணர்திறன்; செயல்பாட்டு / பணி-குறிப்பிட்ட கோரிக்கைகள்
கல்வி மற்றும் முன்னெச்சரிக்கைகள் - தொடங்கு பிடிப்பு மற்றும் பிஞ்ச் வலுவூட்டல் காயம் குணமடைந்த பிறகு சுமார் 2 முதல் 3 வாரங்கள் வரை; படிப்படியாக சுமையை அதிகரிக்கவும் - முன்னேற்றம் முழுமையான கட்டுப்பாடற்ற பயன்பாடு ஆறுதல் மற்றும் வலிமை அனுமதிக்கும்
நிர்வாகம் - உடற்பயிற்சிகள்: கூட்டு / மென்மையான பந்து பிடியை அழுத்துகிறது, பிஞ்ச் வலுவூட்டல், படிப்படியான செயல்பாட்டு சுமை; எஞ்சியுள்ள வடு வேலை மற்றும் உணர்திறன் குறைப்பு - முழு இயக்கம் மற்றும் பிடிப்பு வசதியானது மற்றும் கிட்டத்தட்ட சமச்சீரற்றதாக இருக்கும்போது வெளியேற்றம்; ~ 2 மாதங்களில் வழக்கமான அறுவை சிகிச்சை பின்தொடர்தல் - சிகிச்சையளிக்கும் மருத்துவரை மீண்டும் தொடர்பு கொள்ளவும், குணமடைந்தால், வடுக்கள் வெளிப்படையாக உணர்திறன் அதிகமாக இருந்தால், அல்லது மீண்டும் வருவது குறித்து கவலை இருந்தால்
முழுமையான திரும்ப பெறுதலுக்கான அளவுகோல்கள் - முழுமையான வலி இல்லாத இயக்கம்; வசதியான பிடிப்பு மற்றும் பிஞ்ச்; குடியேறிய வடுக்கள்; வேலை மற்றும் செயல்பாட்டு கோரிக்கைகளை பூர்த்தி செய்ய முடியும்
வேலை மற்றும் செயற்பாட்டிற்கு திரும்புதல்
லேசான அன்றாட கை பயன்பாடு (உண்ணல், எழுதுதல், லேசான சுய-பராமரிப்பு) ஆரம்பத்தில் இருந்தே, ஆறுதலுடன், கனமான பிடிப்பு அல்லது காயத்தின் மூலம் கட்டாய பிஞ்சிங் இல்லாத வரை ஊக்குவிக்கப்படுகிறது. பெரும்பாலான மக்கள் சில நாட்களுக்குள் தினசரி பணிகளை நிர்வகிக்கிறார்கள். ஓட்டுநர் வழக்கமாக ஒரு வாரத்திற்குப் பிறகு மீண்டும் தொடங்குகிறார், நீங்கள் சக்கரத்தை வசதியாகப் பிடிக்கவும் கட்டுப்படுத்தவும் முடியும், மேலும் உங்கள் மதிப்பாய்வில் டாக்டர் ஹிர்பாராவுடன் உறுதிப்படுத்தப்பட்டபடி, இனி உடைகளால் கட்டுப்படுத்தப்படுவதில்லை.
காயம் குணமடைந்தவுடன், சுமார் இரண்டு முதல் மூன்று வாரங்களில் பிடிப்பு மற்றும் வலுவூட்டல் தொடங்குகிறது, மேலும் அவை படிப்படியாக கட்டமைக்கப்படுகின்றன. முழுமையான, கட்டுப்பாடற்ற செயல்பாடு பொதுவாக நான்கு முதல் ஆறு வாரங்களுக்குள் அடையப்படுகிறது. அலுவலக வேலை பெரும்பாலும் சில நாட்களுக்குள் ஒரு வாரத்திற்குள் மீண்டும் தொடங்கலாம்; கனமான கையேடு வேலை உங்கள் பிடியைத் திரும்பும்போது அதே நிலை முன்னேற்றத்தைப் பின்பற்றுகிறது. வழக்கமான பின்தொடர்தல் பொதுவாக இரண்டு மாதங்களுக்கு ஏற்பாடு செய்யப்படுகிறது.
உங்கள் நெறிமுறை பிறகு
இந்த நெறிமுறை நடைமுறையின் பொதுவான மீட்பு ஆலோசனையுடன் இணைந்து செயல்படுகிறதுஃ அறுவை சிகிச்சைக்குப் பிந்தைய வலியை நிர்வகித்தல், காயம் பராமரிப்பு மற்றும் வடு மேலாண்மைA1 தையல் மீது விரலின் அடிப்பகுதியில் இந்த கங்க்லியன் அமர்ந்திருப்பதால், மீட்பு மற்ற சிறிய கைப்பையை பக்க விரல் அடிப்பகுதி நடைமுறைகள் போன்ற பொதுவானது. துப்பாக்கி விரல் வெளியீடுமேற்கண்ட படிப்படியான திட்டம், கங்கை அறுவை சிகிச்சைக்குப் பிறகு வெளியிடப்பட்ட வழிகாட்டுதல்களைப் பிரதிபலிக்கிறது, மேலும் உங்கள் விரல் எவ்வாறு முன்னேறுகிறது என்பதைப் பொறுத்து, உங்கள் தற்போதைய மீட்பு டாக்டர் ஹிர்பரா மற்றும் உங்கள் கை சிகிச்சையாளரால் தனித்தனியாக வழிநடத்தப்படுகிறது.
Evidence & references
Flexor Sheath Ganglion Excision — Lesion, Procedure Outcomes & Post-operative Rehabilitation (Volar Retinacular Cyst)
Topic scope: post-operative rehabilitation after surgical excision of a flexor tendon sheath ganglion (volar retinacular cyst / "seed" ganglion) at the base of a finger — a small, firm, often tender cyst arising from the flexor sheath, commonly over the A1 pulley at the metacarpophalangeal crease of the middle or ring finger. This is an excision, not a reconstruction: the cyst is removed with a small cuff of sheath, the sheath is not repaired, and there is no construct to protect — so the rehab is a brief early-motion pathway built around wound protection, oedema control, tendon gliding and scar/desensitisation work rather than months of protected healing.
Defining principle of the rehab here: a flexor sheath ganglion is a benign cyst tethered to the tendon sheath; excising it (with a cuff of sheath) removes the lesion without creating anything that needs to heal under protection. The sheath is meant to be left open — partial sheath excision does not weaken the digit or cause bowstringing at this level — so immediate, unrestricted light use and early gentle finger motion are the default. The therapy programme exists to keep the flexor tendons gliding through the healing palm wound so they do not adhere, to settle the transient digital-nerve hypersensitivity that commonly follows dissection between the neurovascular bundles, and to mature the scar — not to immobilise. The single branch point is wound healing: scar massage and grip loading wait until the wound is healed and sutures are out.
A. PROCEDURE OUTCOMES (excision of flexor sheath ganglion)
Excision of a flexor sheath ganglion is a small, reliable day-case hand operation: the great majority of patients are rendered symptom-free with a low recurrence rate, and the principal trade-off is the common but self-limiting transient digital-nerve paraesthesia from dissecting the cyst out from between the digital neurovascular bundles.
- Flexor sheath (volar retinacular) ganglions are a well-defined, common entity. They account for roughly 5–16% of ganglions of the hand and wrist, presenting as a small (typically 3–8 mm), firm, often tender nodule fixed to the flexor sheath at the digit base — classically over the A1/A2 pulley region — that does not move with the tendon [JAAOS 2022; JAAOS 1999; Hand Clin 2004]. Well-established (lesion nature).
- Surgical excision gives reliable symptom relief with low recurrence. Level-IV case series of flexor sheath / volar retinacular ganglion excision report durable resolution and low recurrence after complete excision of the cyst with a cuff of sheath; recurrence is the main long-term concern and is uncommon when the lesion and its sheath origin are fully removed [Hand 2007; J Hand Surg series; PMC surgical series]. Moderate (level-IV case series).
- Transient digital-nerve paraesthesia is the principal complication. Because the cyst sits immediately deep to, and is dissected free from, the digital nerves, temporary numbness or tingling in the finger is the commonest reported post-operative event; it is typically self-limiting and settles over weeks. True nerve injury is rare with careful protection of both bundles [Hand 2007; volar retinacular series; Medscape]. Moderate (case series + expert review).
- Partial excision of the sheath is biomechanically tolerated. Removing the cyst with a small cuff of the flexor sheath at the A1 level does not produce clinically significant bowstringing or weakness, which is the anatomical basis for not repairing the sheath and for an early-motion rehab without protected immobilisation [Hand Clin 2004 (palmar digital ganglia / A1–A2 origin)]. Mechanistic.
B. REHABILITATION / THERAPY EVIDENCE
There are no randomised rehab trials specific to flexor sheath ganglion excision; the post-operative programme is low-level / expert-consensus, but it is strikingly consistent across hand-therapy and surgical sources: dressing only (no splint), early gentle finger motion within days, tendon gliding to prevent adhesion, scar massage and desensitisation once healed, and return to full use by ~4–6 weeks.
- Dressing-only, no routine splinting. Aftercare guidance for ganglion (including flexor sheath) excision describes a soft dressing with no immobilisation, with the patient encouraged to move the finger early — there is no construct to protect, so splinting is not required and would risk stiffness [MSA aftercare; Medscape]. Weak / consensus.
- Early active finger motion and tendon gliding prevent stiffness and adhesion. Starting gentle active fist/extension and tendon glides within the first few days keeps the flexor tendons gliding through the palm wound so they do not adhere to the healing scar — the same adhesion-prevention rationale that underpins early-motion hand rehab generally. The benefit is mechanistic / consensus rather than trial-proven for this lesion [hand-therapy aftercare sources]. Weak (mechanism sound).
- Scar massage and desensitisation, started once healed, settle the wound and digital-nerve hypersensitivity. Palm scars at the digit base are prone to tenderness, and the transient digital-nerve paraesthesia from the dissection responds to graded desensitisation; both begin only after the wound is fully healed and sutures are out (~day 10–14) [MSA aftercare; Medscape]. Weak / consensus.
- Grip loading and full return are early. Because nothing is repaired, gripping and strengthening begin once the wound has settled (~2–3 weeks) and full unrestricted use is typically reached by ~4–6 weeks, with routine follow-up around two months — consistent across aftercare sources [MSA aftercare; PMC series; Medscape]. Weak / consensus.
Recovery trajectory (expected, evidence-anchored)
| Phase | Window | Restraint | Hand use / therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Wound protection & early motion | Week 0–1 | Soft dressing, no splint | Elevate above heart; gentle active fist + full extension and tendon glides within a few days; protect wound; light functional use | Light unloaded use only | Transient digital-nerve tingling is expected, not a complication |
| II — Full motion, oedema & scar work | Week ~1–3 | Heavy-grip avoidance | Progress to full active + gentle passive motion (full fist, full extension); scar massage + desensitisation once wound healed; oedema control | No forceful gripping/pinching until wound settled | Sutures out ~day 10–14; scar work only after full healing |
| III — Strengthening & return | Week ~3–6 | Restrictions lifted | Progress grip/pinch loading; task-specific use | Grip/pinch strengthening from ~2–3 wk; full unrestricted use by ~4–6 wk | Routine follow-up ~2 months; driving ~1 wk once gripping the wheel comfortably (surgeon discretion) |
(Phase windows mirror the precautions and return milestones in the patient protocol; they are typical guides, not trial-derived deadlines.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY
- Lesion nature is well-established. The flexor sheath / volar retinacular ganglion is a recognised, characterised entity (firm, sheath-tethered, A1-pulley region, 5–16% of hand/wrist ganglions); its diagnosis and origin are not in dispute. Strong (descriptive).
- Excision outcomes are good but evidenced at level IV. Low recurrence and reliable symptom relief come from case series, not controlled trials — adequate for a small benign lesion, but the evidence tier is modest. Moderate (level-IV).
- Transient digital-nerve paraesthesia vs true nerve injury. Temporary tingling is common and self-limiting; framing it for patients up front avoids alarm, while careful intra-operative protection of both neurovascular bundles keeps true injury rare. Moderate.
- The rehab protocol is consensus, not trial-derived. No RCTs govern post-excision therapy; the dressing-only, early-motion, scar-care, ~4–6-week-return pathway is consistent across sources but rests on expert consensus and the general principles of early-motion hand rehab. Weak / consensus.
- Recurrence is the main long-term failure mode and is uncommon after complete excision of the cyst with its sheath origin; a residual or recurrent lump warrants reassessment rather than prolonged therapy. Moderate.
D. EVIDENCE STRENGTH FLAGS (summary)
- WELL-ESTABLISHED (descriptive): the nature, location and prevalence (5–16% of hand/wrist ganglions) of flexor sheath / volar retinacular ganglions.
- MODERATE (level-IV case series): reliable symptom relief and low recurrence after excision; transient digital-nerve paraesthesia as the principal, self-limiting complication; recurrence as the main long-term failure mode.
- WEAK / CONSENSUS: the dressing-only, early-motion, scar-care rehab programme and its phase timings (consistent across aftercare sources, mechanistically rationalised, but not trial-derived); ~4–6-week full return and ~1-week driving (surgeon discretion).
CITATIONS
RAG corpus (180,000+ Orthopaedic articles)
- Ganglions of the hand and wrist. J Am Acad Orthop Surg. 2022. DOI: 10.5435/jaaos-d-22-00105
- Ganglions of the hand and wrist. J Am Acad Orthop Surg. 1999. DOI: 10.5435/00124635-199907000-00003
- Surgical excision of flexor sheath ganglions of the hand: results and outcomes. Hand (N Y). 2007. DOI: 10.1007/s11552-007-9028-4
- Volar retinacular ganglions of the hand: a clinical series. J Hand Surg Am. 2011. DOI: 10.1016/j.jhsa.2011.05.013
- Palmar digital ganglia and the A1–A2 sheath origin. Hand Clin. 2004. DOI: 10.1016/j.hcl.2004.03.015
Flexor sheath ganglion / rehabilitation literature (URLs)
- Surgical excision of flexor sheath ganglions — case series (full text). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC2527143/
- Volar retinacular ganglions of the hand. Journal of Hand Surgery (American). https://www.jhandsurg.org/article/S0363-5023(11)00627-7/abstract
- Ganglion cyst excision — post-operative aftercare (dressing-only, early motion, scar care, ~4–6 week return). Mississippi Sports & Arthritis (MSA) Hand Center. https://msapc.com/hand-center/aftercare/ganglion-cyst-excision/
- Ganglion treatment (surgical excision, recurrence and transient digital-nerve paraesthesia). Medscape. https://emedicine.medscape.com/article/1243525-treatment





