屈肌腱鞘囊肿切除术
Patients › Rehabilitation
在手指基部切除屈肌腱鞘腱鞘囊肿(掌侧韧带囊肿)后,采用快速、以活动为导向的康复计划,在开始数天内进行轻柔的手指活动以保护手掌的小伤口,随后在伤口愈合过程中加入瘢痕护理和握力训练。
本方案指导您在基兰·希尔帕拉医生(Dr Kieran Hirpara)于洛克汉普顿 Mater 私人医院接受屈肌腱鞘囊肿切除术后的康复过程。该囊肿是一种位于手掌侧手指根部的坚硬囊性肿物。方案从您的家庭锻炼计划开始,随后是为您的手部治疗师制定的结构化临床方案;请在首次治疗就诊时携带此页面或其 PDF 文件,以确保您的康复过程协调一致。您的手部治疗师可能会根据您的康复进展调整该计划。
如果您对术后伤口有任何疑虑,请联系诊所。拍摄伤口照片并通过电子邮件发送以供审查通常很有帮助。
预期情况
屈肌腱鞘囊肿(也称为掌侧腱鞘囊肿)是一种小而硬的、常有压痛的肿块,通常仅几毫米大小,起源于屈肌腱穿行的腱鞘,位于手指掌侧基部(常见于称为A1滑车的坚韧束带处,即手指与手掌交界的横纹处)。该肿块固定于腱鞘,屈曲手指时不会移动。这是一种完全良性(非癌性)的肿块,也是手部和腕部较为常见的腱鞘囊肿之一。
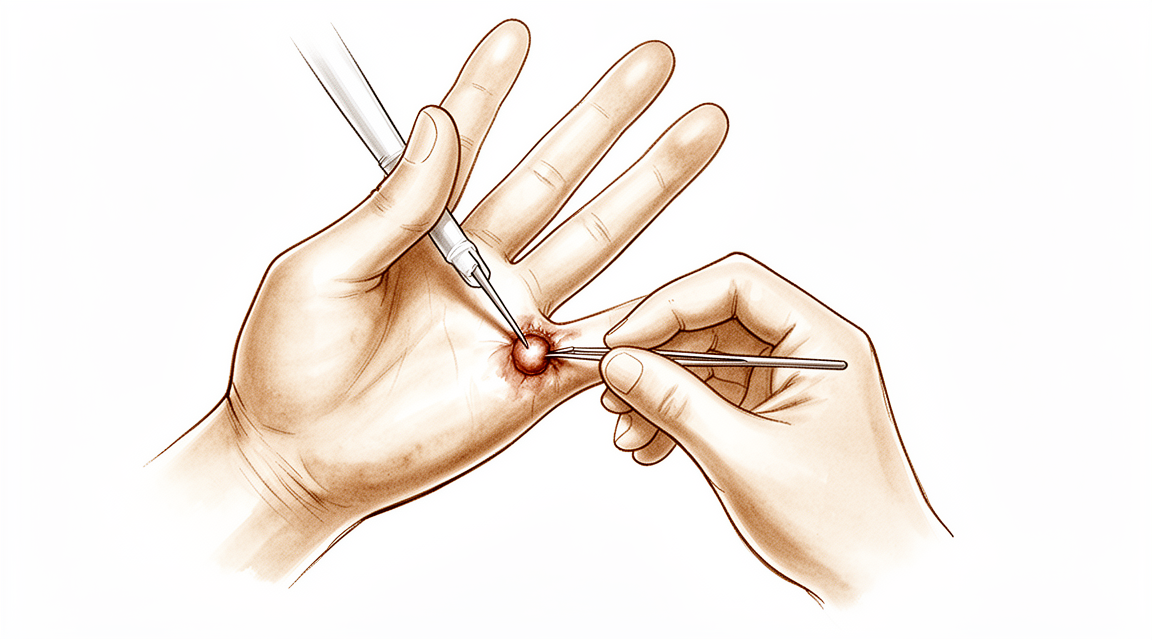
手术为小型日间切除手术。通过在手掌处做一个短的“Z”字形切口,Hirpara 医生将囊肿连同其起源处的一小圈腱鞘一并切除。沿手指两侧走行的两条小神经和血管受到仔细保护。腱鞘本身不予修复:故意保持其开放状态,并不会削弱手指功能。皮肤用缝线闭合。
由于手指内部无需在愈合期间进行保护,因此恢复迅速:以周计,而非以月计。计划很简单:保护手掌的小伤口,控制肿胀,并在几天后开始轻柔的手指活动,以防止手指僵硬以及肌腱粘连至愈合中的瘢痕。伤口愈合后,通过瘢痕按摩和脱敏处理使该区域恢复稳定,并逐步重建握力。早期伤口周围出现轻微麻木或压痛很常见,这是小皮神经恢复过程中的正常现象,通常在随后的几周内逐渐消退。
注意事项与限制
- 在伤口愈合且缝线拆除前(通常为术后第10–14天),保持敷料清洁干燥。无需石膏,通常也不使用夹板,仅使用软性敷料。
- 应在最初几天内开始轻柔的手指活动(屈曲、伸直及肌腱滑动练习),以预防僵硬和肌腱粘连。
- 应保持手部抬高,并在舒适范围内进行日常轻度活动。
- 切勿在伤口稳定前(约2至3周)进行用力握持、提举或强力捏取动作。
- 切勿在伤口完全愈合前按摩瘢痕或浸泡手部。
- 切勿在敷料影响您安全握持方向盘时驾驶车辆,通常需持续约1周。
关于伤口、肿胀及瘢痕管理,请参阅本诊所的伤口护理指南。
您的练习
这些是您讲义中的练习。仅在 Hirpara 医生和您的手部治疗师的指导下开始,并严格遵循您被给予的任何限制。早期练习(轻柔的握拳与伸直、肌腱滑动和肿胀控制)在最初几天内保持手指活动并让肌腱滑动,这是实现顺利康复的最重要因素。瘢痕按摩和脱敏治疗在伤口完全愈合后开始,而握力强化则属于稍晚的阶段(大约从术后两到三周开始)。如果任何练习引起伤口处的锐痛,请立即停止。
您的临床方案
本页面其余部分为屈肌腱鞘囊肿(掌侧腱鞘囊肿)切除术后康复的阶段性临床方案。本节内容将提供给您的手治疗师,每个阶段均以通俗易懂的语言解释当前阶段的治疗重点。本手术为切除而非修复:腱鞘保持开放状态,不存在需要保护的修复结构。该方案属于早期活动路径,核心在于保护伤口、控制水肿、促进肌腱滑动以预防粘连,以及进行瘢痕管理和脱敏训练,而非保护性固定。
治疗前,请查阅手术记录和既往病史,并与主刀医生沟通,确认受累手指、腱鞘切除范围以及指神经血管束的完整性。Hirpara 博士的切除手术采用 Bruner(锯齿状)掌侧切口,覆盖 A1 滑车/近端腱鞘,连同腱鞘袖口一并切除囊肿;腱鞘不予缝合,术后除软性敷料外无需固定。一过性指神经感觉异常较为常见,且具有自限性。
第一阶段——伤口保护与早期活动(第0周至约1周)
第一周旨在保护手掌的小伤口,并尽早活动手指,以防止关节僵硬或肌腱粘连。手部采用无夹板的厚软敷料包扎,保持抬高,并在数天内开始轻柔的主动手指活动。
致您的手部治疗师:
教育与注意事项 - 仅使用厚软敷料,不使用夹板;保持清洁干燥,直至拆线(约第10–14天) - 保护伤口免受重负荷;在舒适范围内进行轻度的无负重手部活动 - 告知患者,伤口周围出现短暂的指神经感觉异常/过敏是常见现象,且具有自限性
管理措施 - 伤口:按医嘱进行外科敷料处理;监测感染迹象 - 水肿:抬高至心脏水平以上,进行轻柔的手指泵动练习,必要时冰敷 - 锻炼:在数天内开始轻柔的主动手指活动度训练(AROM)(轻柔的复合握拳和完全伸展)以及肌腱滑动练习(钩状/握拳/伸直);未受累指、拇指和腕关节的主动活动;轻度功能性使用
进展标准 - 伤口愈合稳定,无感染;舒适的早期主动活动范围;伤口允许的情况下,准备进行全范围主动/轻柔被动活动
第二阶段——完全活动度、水肿及瘢痕处理(约第1至3周)
从大约1周开始,活动度进展至完全主动活动及轻柔的被动活动范围(完全握拳及完全伸直);一旦伤口完全愈合且缝线拆除,即可开始瘢痕按摩及脱敏治疗。水肿控制持续进行。
供您手治疗师参考:
评估 - 手指主动及被动活动范围(目标为完全握拳及完全伸直);伤口/瘢痕状况;肿胀;指神经敏感性
教育与注意事项 - 在舒适允许的情况下,进展至完全主动及轻柔的被动手指活动 - 仅在伤口完全愈合后开始瘢痕按摩及脱敏治疗 - 在伤口稳定前,避免用力握持及强力捏持
管理 - 练习:完全复合握拳及完全伸直;持续进行肌腱滑动练习;对任何残留的僵硬部位进行轻柔的被动牵伸 - 瘢痕:愈合后行瘢痕按摩+纹理脱敏;根据需要管理水肿
进展标准 - 完全无痛的主动活动;伤口愈合;瘢痕趋于稳定;准备好进行负荷训练
第三阶段——强化与恢复(约第3至6周)
伤口愈合且活动度完全恢复后(约三周),开始握力和捏力强化训练,并逐渐增加强度,直至完全无限制使用。大多数患者在约四至六周时恢复全部活动,并在约两个月时进行常规随访。
供您的手部治疗师参考:
评估 - 与健侧对比的握力和捏力;残留瘢痕的压痛或敏感性;功能性/特定任务需求
教育与注意事项 - 伤口稳定后(约2–3周),开始握力和捏力强化训练;逐渐增加负荷 - 根据舒适度和力量情况,逐步过渡至完全无限制使用
管理 - 练习:使用治疗泥/软球进行握力挤压、捏力强化、渐进性功能性负荷;继续进行任何残留的瘢痕处理和脱敏治疗 - 当活动度完全恢复,握力舒适且接近对称时出院;约2个月时进行常规外科随访 - 如果恢复出现平台期、瘢痕持续明显高敏,或担心复发,请转回主治医生处
完全恢复的标准 - 无痛的全范围活动;舒适的握力和捏力;瘢痕稳定;能够满足工作和活动需求
重返工作与活动
从术后开始,鼓励在舒适范围内进行日常手部轻度活动(如进食、书写、轻度自理),前提是避免通过伤口进行用力握持或强迫性捏取。大多数人可在数天内完成日常任务。通常在约一周后可恢复驾驶,前提是能够舒适地握持并控制方向盘,且敷料不再造成限制,并经Hirpara医生在复查时确认。
握力与强化训练通常在伤口愈合稳定后(约术后2至3周)开始,并逐步增加。完全、不受限制的活动通常在术后4至6周达到。办公室工作通常在数天至一周内即可恢复;体力劳动则随着握力恢复,遵循相同的阶段性进展。通常在术后约两个月安排常规随访。
术后方案
本方案与诊所的一般康复建议配合使用:请参阅术后疼痛管理、伤口护理和疤痕管理。由于该腱鞘囊肿位于手指基部、A1滑车之上,其康复过程与其他位于手掌侧手指基部的较小手术(如扳机指松解术)有许多共同之处。上述分阶段计划反映了腱鞘囊肿切除术后已发表的指导原则,您的后续康复将由Hirpara医生和您的手部治疗师根据您手指的恢复情况个体化指导。
Evidence & references
Flexor Sheath Ganglion Excision — Lesion, Procedure Outcomes & Post-operative Rehabilitation (Volar Retinacular Cyst)
Topic scope: post-operative rehabilitation after surgical excision of a flexor tendon sheath ganglion (volar retinacular cyst / "seed" ganglion) at the base of a finger — a small, firm, often tender cyst arising from the flexor sheath, commonly over the A1 pulley at the metacarpophalangeal crease of the middle or ring finger. This is an excision, not a reconstruction: the cyst is removed with a small cuff of sheath, the sheath is not repaired, and there is no construct to protect — so the rehab is a brief early-motion pathway built around wound protection, oedema control, tendon gliding and scar/desensitisation work rather than months of protected healing.
Defining principle of the rehab here: a flexor sheath ganglion is a benign cyst tethered to the tendon sheath; excising it (with a cuff of sheath) removes the lesion without creating anything that needs to heal under protection. The sheath is meant to be left open — partial sheath excision does not weaken the digit or cause bowstringing at this level — so immediate, unrestricted light use and early gentle finger motion are the default. The therapy programme exists to keep the flexor tendons gliding through the healing palm wound so they do not adhere, to settle the transient digital-nerve hypersensitivity that commonly follows dissection between the neurovascular bundles, and to mature the scar — not to immobilise. The single branch point is wound healing: scar massage and grip loading wait until the wound is healed and sutures are out.
A. PROCEDURE OUTCOMES (excision of flexor sheath ganglion)
Excision of a flexor sheath ganglion is a small, reliable day-case hand operation: the great majority of patients are rendered symptom-free with a low recurrence rate, and the principal trade-off is the common but self-limiting transient digital-nerve paraesthesia from dissecting the cyst out from between the digital neurovascular bundles.
- Flexor sheath (volar retinacular) ganglions are a well-defined, common entity. They account for roughly 5–16% of ganglions of the hand and wrist, presenting as a small (typically 3–8 mm), firm, often tender nodule fixed to the flexor sheath at the digit base — classically over the A1/A2 pulley region — that does not move with the tendon [JAAOS 2022; JAAOS 1999; Hand Clin 2004]. Well-established (lesion nature).
- Surgical excision gives reliable symptom relief with low recurrence. Level-IV case series of flexor sheath / volar retinacular ganglion excision report durable resolution and low recurrence after complete excision of the cyst with a cuff of sheath; recurrence is the main long-term concern and is uncommon when the lesion and its sheath origin are fully removed [Hand 2007; J Hand Surg series; PMC surgical series]. Moderate (level-IV case series).
- Transient digital-nerve paraesthesia is the principal complication. Because the cyst sits immediately deep to, and is dissected free from, the digital nerves, temporary numbness or tingling in the finger is the commonest reported post-operative event; it is typically self-limiting and settles over weeks. True nerve injury is rare with careful protection of both bundles [Hand 2007; volar retinacular series; Medscape]. Moderate (case series + expert review).
- Partial excision of the sheath is biomechanically tolerated. Removing the cyst with a small cuff of the flexor sheath at the A1 level does not produce clinically significant bowstringing or weakness, which is the anatomical basis for not repairing the sheath and for an early-motion rehab without protected immobilisation [Hand Clin 2004 (palmar digital ganglia / A1–A2 origin)]. Mechanistic.
B. REHABILITATION / THERAPY EVIDENCE
There are no randomised rehab trials specific to flexor sheath ganglion excision; the post-operative programme is low-level / expert-consensus, but it is strikingly consistent across hand-therapy and surgical sources: dressing only (no splint), early gentle finger motion within days, tendon gliding to prevent adhesion, scar massage and desensitisation once healed, and return to full use by ~4–6 weeks.
- Dressing-only, no routine splinting. Aftercare guidance for ganglion (including flexor sheath) excision describes a soft dressing with no immobilisation, with the patient encouraged to move the finger early — there is no construct to protect, so splinting is not required and would risk stiffness [MSA aftercare; Medscape]. Weak / consensus.
- Early active finger motion and tendon gliding prevent stiffness and adhesion. Starting gentle active fist/extension and tendon glides within the first few days keeps the flexor tendons gliding through the palm wound so they do not adhere to the healing scar — the same adhesion-prevention rationale that underpins early-motion hand rehab generally. The benefit is mechanistic / consensus rather than trial-proven for this lesion [hand-therapy aftercare sources]. Weak (mechanism sound).
- Scar massage and desensitisation, started once healed, settle the wound and digital-nerve hypersensitivity. Palm scars at the digit base are prone to tenderness, and the transient digital-nerve paraesthesia from the dissection responds to graded desensitisation; both begin only after the wound is fully healed and sutures are out (~day 10–14) [MSA aftercare; Medscape]. Weak / consensus.
- Grip loading and full return are early. Because nothing is repaired, gripping and strengthening begin once the wound has settled (~2–3 weeks) and full unrestricted use is typically reached by ~4–6 weeks, with routine follow-up around two months — consistent across aftercare sources [MSA aftercare; PMC series; Medscape]. Weak / consensus.
Recovery trajectory (expected, evidence-anchored)
| Phase | Window | Restraint | Hand use / therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Wound protection & early motion | Week 0–1 | Soft dressing, no splint | Elevate above heart; gentle active fist + full extension and tendon glides within a few days; protect wound; light functional use | Light unloaded use only | Transient digital-nerve tingling is expected, not a complication |
| II — Full motion, oedema & scar work | Week ~1–3 | Heavy-grip avoidance | Progress to full active + gentle passive motion (full fist, full extension); scar massage + desensitisation once wound healed; oedema control | No forceful gripping/pinching until wound settled | Sutures out ~day 10–14; scar work only after full healing |
| III — Strengthening & return | Week ~3–6 | Restrictions lifted | Progress grip/pinch loading; task-specific use | Grip/pinch strengthening from ~2–3 wk; full unrestricted use by ~4–6 wk | Routine follow-up ~2 months; driving ~1 wk once gripping the wheel comfortably (surgeon discretion) |
(Phase windows mirror the precautions and return milestones in the patient protocol; they are typical guides, not trial-derived deadlines.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY
- Lesion nature is well-established. The flexor sheath / volar retinacular ganglion is a recognised, characterised entity (firm, sheath-tethered, A1-pulley region, 5–16% of hand/wrist ganglions); its diagnosis and origin are not in dispute. Strong (descriptive).
- Excision outcomes are good but evidenced at level IV. Low recurrence and reliable symptom relief come from case series, not controlled trials — adequate for a small benign lesion, but the evidence tier is modest. Moderate (level-IV).
- Transient digital-nerve paraesthesia vs true nerve injury. Temporary tingling is common and self-limiting; framing it for patients up front avoids alarm, while careful intra-operative protection of both neurovascular bundles keeps true injury rare. Moderate.
- The rehab protocol is consensus, not trial-derived. No RCTs govern post-excision therapy; the dressing-only, early-motion, scar-care, ~4–6-week-return pathway is consistent across sources but rests on expert consensus and the general principles of early-motion hand rehab. Weak / consensus.
- Recurrence is the main long-term failure mode and is uncommon after complete excision of the cyst with its sheath origin; a residual or recurrent lump warrants reassessment rather than prolonged therapy. Moderate.
D. EVIDENCE STRENGTH FLAGS (summary)
- WELL-ESTABLISHED (descriptive): the nature, location and prevalence (5–16% of hand/wrist ganglions) of flexor sheath / volar retinacular ganglions.
- MODERATE (level-IV case series): reliable symptom relief and low recurrence after excision; transient digital-nerve paraesthesia as the principal, self-limiting complication; recurrence as the main long-term failure mode.
- WEAK / CONSENSUS: the dressing-only, early-motion, scar-care rehab programme and its phase timings (consistent across aftercare sources, mechanistically rationalised, but not trial-derived); ~4–6-week full return and ~1-week driving (surgeon discretion).
CITATIONS
RAG corpus (180,000+ Orthopaedic articles)
- Ganglions of the hand and wrist. J Am Acad Orthop Surg. 2022. DOI: 10.5435/jaaos-d-22-00105
- Ganglions of the hand and wrist. J Am Acad Orthop Surg. 1999. DOI: 10.5435/00124635-199907000-00003
- Surgical excision of flexor sheath ganglions of the hand: results and outcomes. Hand (N Y). 2007. DOI: 10.1007/s11552-007-9028-4
- Volar retinacular ganglions of the hand: a clinical series. J Hand Surg Am. 2011. DOI: 10.1016/j.jhsa.2011.05.013
- Palmar digital ganglia and the A1–A2 sheath origin. Hand Clin. 2004. DOI: 10.1016/j.hcl.2004.03.015
Flexor sheath ganglion / rehabilitation literature (URLs)
- Surgical excision of flexor sheath ganglions — case series (full text). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC2527143/
- Volar retinacular ganglions of the hand. Journal of Hand Surgery (American). https://www.jhandsurg.org/article/S0363-5023(11)00627-7/abstract
- Ganglion cyst excision — post-operative aftercare (dressing-only, early motion, scar care, ~4–6 week return). Mississippi Sports & Arthritis (MSA) Hand Center. https://msapc.com/hand-center/aftercare/ganglion-cyst-excision/
- Ganglion treatment (surgical excision, recurrence and transient digital-nerve paraesthesia). Medscape. https://emedicine.medscape.com/article/1243525-treatment





