அருகில் உள்ள இடுப்பு உறுப்பு (ORIF)
Patients › Rehabilitation
Rehabilitation after locking-plate fixation of a proximal humerus fracture, gated on radiographic healing at review.
மேட்டர் தனியார் மருத்துவமனை ராக்ஹாம்ப்டனில் உள்ள டாக்டர் கியரன் ஹிர்பாராவுடன் ஒரு நெருக்கமான இடுப்பு எலும்பு முறிவின் அறுவை சிகிச்சைக்குப் பிறகு மறுவாழ்வை இந்த நெறிமுறை உள்ளடக்கியது. இந்த பக்கத்தை அல்லது அதன் PDF ஐ உங்கள் முதல் உடலியல் சிகிச்சை வருகைக்கு கொண்டு வாருங்கள், இதனால் உங்கள் மறுவாழ்வு ஒருங்கிணைக்கப்படுகிறது. உங்கள் எலும்பு முறிவு எவ்வாறு குணமடைகிறது என்பதைப் பொறுத்து, உங்கள் உடலியல் சிகிச்சையாளர் கீழே உள்ள கட்டங்கள் மூலம் தனித்தனியாக முன்னேறுகிறார்.
அறுவை சிகிச்சைக்குப் பிறகு உங்கள் காயத்தைப் பற்றி ஏதேனும் கவலைகள் இருந்தால், அறைகளைத் தொடர்பு கொள்ளுங்கள். காயத்தின் புகைப்படத்தை எடுத்து அதை மதிப்பாய்வு செய்ய மின்னஞ்சல் அனுப்புவது பெரும்பாலும் உதவியாக இருக்கும்.
எதிர்பார்ப்பது என்ன
பெரும்பாலான திட்டமிடப்பட்ட தோள்பட்டை அறுவை சிகிச்சைகளுக்குப் பிறகு மறுவாழ்வு வேறுபட்டதாக செயல்படுகிறது. தகடு மற்றும் திருகுகள் உடைந்த எலும்பை நிலைநிறுத்துகின்றன, ஆனால் எலும்பு இன்னும் குணமடைய வேண்டும், அந்த குணமடையும் வேகம் நபருக்கு நபர் மாறுபடும். அந்த காரணத்திற்காக, கீழே உள்ள கால அட்டவணை ஒரு நிலையான அட்டவணைக்கு பதிலாக ஒரு வழிகாட்டியாகும்: உங்கள் திட்டத்தில் ஒவ்வொரு அடியும் அறுவை சிகிச்சைக்குப் பிறகு வாரங்களின் எண்ணிக்கையையும், உங்கள் எக்ஸ்-கதிர்களில் எலும்பு எவ்வாறு குணமடைகிறது என்பதையும் பொறுத்தது, டாக்டர் ஹிர்பாராவுடன் உங்கள் மதிப்புரைகளில் உறுதிப்படுத்தப்பட்டுள்ளது. காலெண்டரில் அடுத்த கட்டத்திற்கு நீங்களே செல்ல வேண்டாம்; உங்கள் மதிப்பாய்வைக் காத்திருங்கள்.
இந்த அறுவை சிகிச்சையை வித்தியாசமாக்கும் இன்னொரு விஷயம் இருக்கிறது. கட்டிகள்ரோட்டேட்டர் கஃப் தசைகள் இணைக்கப்படுகின்றன, மேலும் பல அருகிலுள்ள இடுப்பு முறிவுகளில் இந்த துண்டுகள் முறிவின் ஒரு பகுதியாகும் மற்றும் தட்டு அல்லது தையல்களால் பின்னால் சரி செய்யப்படுகின்றன. ரோட்டேட்டர் கஃப் தசைகளை மிகவும் கடினமாக வேலை செய்வது, அவை குணமடைவதற்கு முன்பே அந்த துண்டுகளை இழுக்கலாம். ஒரு நவீன பூட்டு தட்டுடன் உறுதிப்படுத்தல் முதல் நாளிலிருந்து வலுவாக உள்ளது, எனவே மென்மையான ஆரம்ப இயக்கம் ஊக்குவிக்கப்படுகிறது: நீங்கள் தோள்பட்டை தீவிரமாக உதவியுடன் மற்றும் மென்மையாக ஆரம்பத்தில் இருந்து வசதியாக நகர்த்தலாம், வலி இல்லாத வரம்பில் கையை உயர்த்தலாம். கவனமாக இருக்கும் உறுப்பு ரோட்டேட்டர் கஃப் சுமைஃ குழாய் துண்டுகள் முறிவின் ஒரு பகுதியாக இல்லாதபோது, அல்லது திடமாக சரிசெய்யப்பட்டால், உங்கள் அறுவை சிகிச்சையாளர் செயலில் சுழற்சி மற்றும் கஃப் வேலைகளை விரைவாகத் தொடங்க உங்களுக்கு அனுமதி அளிக்கலாம்; குழாய் சுழற்சிகள் ஈடுபட்டுள்ள மற்றும் குணமடையும் போது, ரோட்டேட்டர் கஃப் வேலை மற்றும் கட்டாய சு
உங்கள் உடற்பயிற்சி திட்டம் மூன்று வகையான இயக்கங்களைப் பயன்படுத்துகிறது, உங்கள் குழு உங்களுக்கு பொருந்தும் என்பதைக் குறிக்கும்:
- இயக்கத்தின் செயலில் உள்ள வரம்பு: உதவி அல்லது உதவியின்றி இயக்கம் அனுமதிக்கப்படுகிறது.
- செயலில்-உதவி பெற்ற இயக்கம் வரம்புஃ மற்றொரு கையை அல்லது கையை நகர்த்த உதவும் ஒரு பொருளை பயன்படுத்தி.
- செயலற்ற இயக்கம் வரம்பு: முற்றிலும் தளர்வான, 100% வேலை செய்ய மற்ற கை அல்லது வலிமை பயன்படுத்தி.
நீங்கள் அறுவை சிகிச்சையிலிருந்து உங்கள் கையை ஒரு ஸ்லிங்கில் கொண்டு எழுந்திருப்பீர்கள். முதல் மூன்று வாரங்களுக்கு அதை முழுநேரமாக அணியுங்கள், பின்னர் ஆறுதல் அனுமதிக்க அடுத்த வாரங்களில் அதை விலக்கி விடுங்கள்; வெளியிடப்பட்ட நெறிமுறைகள் சராசரியாக மூன்று வாரங்கள் இயங்காதவை, மற்றும் சான்றுகள் ஸ்லிங்கில் நீண்ட காலத்திற்கு முந்தைய இயக்கத்தை ஆதரிக்கின்றன. நீங்கள் அதில் தூங்க வேண்டியதில்லை. உங்கள் உடற்பயிற்சிகள் மற்றும் கழுவுதல் மற்றும் ஆடை அணிவதற்கு ஒரு நாளைக்கு பல முறை அதை எடுத்துக் கொள்ளுங்கள், மேலும் வீட்டில் அமைதியாக உட்கார்ந்திருக்கும்போது கையை ஸ்லிங்கிலிருந்து வெளியேற்றலாம். சட்டைப் பட்டை அணிந்திருக்கும்போது வாகனம் ஓட்ட வேண்டாம்.
ஒரு பார்வையில் பயணம்:
- கட்டம் I பாதுகாப்பு மற்றும் ஆரம்பகால செயலற்ற இயக்கம்: வாரங்கள் 06
- கட்டம் II மீண்டும் செயலில் இயக்கம்ஃ வாரங்கள் 612
- கட்டம் III வலுவூட்டல்: சுமார் 3 முதல் 41⁄2 மாதங்கள்
- கட்டம் IV முழுமையான செயல்பாட்டிற்கு திரும்புதல்: சுமார் 41⁄26 மாதங்களிலிருந்து
கட்டம் I பாதுகாப்பு மற்றும் ஆரம்பகால செயலற்ற இயக்கம் (வாரங்கள் 06)
முதல் ஆறு வாரங்கள் நிலையான எலும்பு முறிவைப் பாதுகாப்பதைப் பற்றியது, அதே நேரத்தில் மீதமுள்ள கை (மற்றும் தோள்பட்டை மூட்டு) இறுக்கமடைவதைத் தடுக்கிறது. பூட்டுதல் தட்டு ஆரம்பத்தில் இருந்து எலும்பைப் பாதுகாப்பாக வைத்திருப்பதால், ஆறு வாரங்கள் காத்திருப்பதற்குப் பதிலாக மென்மையான ஆரம்ப இயக்கம் ஊக்குவிக்கப்படுகிறது. நீங்கள் வீட்டிற்குச் செல்வதற்கு முன்பு ஒரு பிசியோதெரபிஸ்ட் மென்மையான பயிற்சிகளில் உங்களைத் தொடங்குவார்ஃ பெண்டலூம் பயிற்சிகள் (கை தொங்கவிடவும், உங்கள் உடலை அசைப்பதன் மூலம் மெதுவாக அசைக்கவும்), மற்றும் முழங்கை, மணிக்கட்டு மற்றும் கையை ஒரு நாளைக்கு பல முறை ஸ்லிங்கிலிருந்து வெளியே நகர்த்துவது. ஆரம்பத்தில் இருந்தே, மற்றும் வசதியான, வலி இல்லாத வரம்பிற்குள், உங்கள் மற்ற கையின் உதவியுடன் (செயலில்-உதவி) மற்றும் மெதுவாக அதன் சொந்த சக்தியின் கீழ் (செயலில்) கையை நகர்த்தத் தொடங்கலாம், வசதியை அனுமதிக்கும் போது அதை உங்கள் முன் உயர்த்துவது. எச்சரிக்கையான பகுதி ரோட்டேட்டர் கம்பை சுமைப்பதைத் தவி
உங்கள் பிசியோதெரபிஸ்ட்டுக்கு:
இலக்குகள்
- உறுப்பைப் பாதுகாக்கவும், எலும்பு குணமடையச் செய்யவும்
- வலி மற்றும் வீக்கத்தை குறைக்க
- வலி இல்லாத வரம்பிற்குள் செயலில் உள்ள உயரத்திற்கு முன்கூட்டியே செயலில்-உதவி செய்யப்படும் முன்னேற்றத்தை நிறுவுதல்
- கழுத்து, முழங்கை, மணிக்கட்டு மற்றும் கைகளின் முழு இயக்கத்தையும் பராமரிக்கவும்
நிர்வாகம்
- ~3 வாரங்களுக்கு முழுநேரமாக ஸ்லிங், பின்னர் வசதிக்காக அனுமதிக்கிறது (இலெக்டிரேஷன் கன்வென்ஷன்); உடற்பயிற்சி மற்றும் சுகாதாரத்திற்காக தினமும் பல முறை அகற்றப்படுகிறது; படுக்கையில் தேவையில்லை
- தினமும் பலமுறை பெண்டில் / கோட்மேன் உடற்பயிற்சி
- நிலையான உறுதிப்படுத்தலுக்காக ஆரம்பத்தில் இருந்து வசதியான, வலி இல்லாத வரம்பிற்குள் முன்கூட்டியே செயலில்-உதவி மற்றும் மென்மையான செயலில் முன்னோக்கி உயர்வு; கட்டுப்பாட்டு அனுமதிப்பதைப் போல செங்குத்தாக முன்னேறும் சாய்ந்த-தொடக்க உயர்வு; ஆறுதல் அனுமதிப்பதைப் போல வரம்பை முன்னேற்றுங்கள்
- செயல்திறன் இன்னும் அனுமதிக்கப்படாதபோது தேவைக்கேற்ப செயலற்ற இயக்க வரம்புஃ ஸ்கேப்புலர் விமானத்தில் சுமார் 90 ° வரை முன்னோக்கி உயர்வு, வயிற்றின் உள் சுழற்சி (பின்புறம் அல்ல)
- வெளிப்புற சுழற்சி சுமார் 30 40 ° ஒரு மென்மையான ஆரம்ப இயல்புநிலை வைக்கப்படும் பக்கத்தில் கை; அறுவை சிகிச்சை நிபுணர் tuberosities uninvolved அல்லது உறுதியாக நிலையான இந்த முன்கூட்டியே முடியும்
- கழுத்து, முழங்கை, மணிக்கட்டு மற்றும் கை ஆகியவற்றின் சுறுசுறுப்பான சுறுசுறுப்பான சுறுசுறுப்பு; பந்து பிடிப்புக்கான சுருக்கங்கள்
- ஸ்காப்புலர் அமைத்தல் மற்றும் ஸ்காப்புலர் இயக்கம் (உயர்வு, மனச்சோர்வு, இழுத்தல், நீட்டிப்பு)
- மென்மையான டெல்டோயிட் மற்றும் பெரிஸ்காப்புலர் ஐசோமெட்ரிக்ஸ் வசதியை அனுமதிக்கும் வகையில் அறிமுகப்படுத்தப்படலாம்
- குளிர் சிகிச்சை மற்றும் அனல்ஜீசியா அமர்வுகளுக்கு முன்; காயம் குணமடைந்தவுடன் வடுக்களை அணிதிரட்டுதல் மற்றும் உணர்திறன் குறைத்தல்
எச்சரிக்கைகள்
- கட்டாய அல்லது எதிர்ப்பு வெளிப்புற சுழற்சி மற்றும் கனமான சுழற்சி-மணிக்கட்டு சுமை ஆகியவற்றைத் தவிர்க்கவும், குடலிறக்கம் குணமடையும் வரை (அறுவை சிகிச்சை நிபுணர் வழிகாட்டுதல்); வலி இல்லாத வரம்பில் செயலில் உயர்வு அனுமதிக்கப்படுகிறது
- பின்புறத்தில் உள் சுழற்சி இல்லை; கொரோனல் விமானத்தில் கடத்தப்படுவதைத் தவிர்க்கவும்
- ஆரம்பகால இயக்கம் வலியற்றதாக இருக்கட்டும்: மென்மையாகவும் வசதியாகவும், கட்டாயப்படுத்தப்படாமல்
- இயக்கப்படும் கையில் சுமார் 0.51 கிலோவுக்கு மேல் தூக்குதல் இல்லை
- அறுவை சிகிச்சையளிக்கப்பட்ட கை வழியாக எடை தாங்கல் இல்லை (ஒரு நாற்காலியில் இருந்து அல்லது படுக்கையில் இருந்து தள்ளுதல் இல்லை)
- ஸ்லிங் அணிந்திருக்கும் போது வாகனம் ஓட்டக்கூடாது
- கட்டாயமான அல்லது வலிமிகுந்த இறுதி வரம்பு இயக்கம் இல்லை
முன்னேற்றத்திற்கான அளவுகோல்கள்
- சுமார் 6 வாரங்களில் டாக்டர் ஹிர்பாராவுடன் ஆய்வு செய்தபோது உறுதிப்படுத்தப்பட்டபடி, குணமடைதல் முன்னேறுவதற்கான ரேடியோகிராஃபி சான்றுகள்
- வலி நன்கு கட்டுப்படுத்தப்பட்டது
- முழு முழங்கை, மணிக்கட்டு மற்றும் கை இயக்கம் பராமரிக்கப்படுகிறது
- ஒரு வலி இல்லாத வரம்பிற்குள் வசதியான செயலில் உதவியுடன் செயலில் உயர்வு
கட்டம் II மீண்டும் செயலில் இயக்கம் (வாரங்கள் 612)
ஆறு வாரங்களுக்குள் உங்கள் மதிப்பாய்வில், டாக்டர் ஹிர்பாரா உங்கள் எக்ஸ்-கதிர்களை சரிபார்க்கிறார். குணமடைதல் எதிர்பார்த்தபடி முன்னேறினால், மீதமுள்ள ஸ்லிங் பயன்பாடு நிறுத்தப்பட்டு, நீங்கள் முதலில் உதவியுடன் (மற்ற கை, ஒரு குச்சி அல்லது ஒரு புல்லியைப் பயன்படுத்தி), பின்னர் சுறுசுறுப்பாக உங்கள் கையை நகர்த்தத் தொடங்குவீர்கள். உங்கள் முதுகில் படுத்துக் கொண்டிருக்கும்போது கையை சுறுசுறுப்பாக உயர்த்தத் தொடங்குவது சிறந்தது, அங்கு ஈர்ப்பு குறைவாக இருக்கும், மேலும் கட்டுப்பாடு மேம்படும்போது உட்கார்ந்து நின்று முன்னேறுவது சிறந்தது. டாக்டர் ஹிர்பாரா உறுதிப்படுத்தியவுடன் சுழற்சி மண்டலத்திற்கான மென்மையான தசை-அமைத்தல் (ஐசோமெட்ரிக்) பயிற்சிகள் இந்த கட்டத்தில் தொடங்குகின்றன; எதிர்ப்புக்கு எதிரான பயிற்சிகள் பின்னர் வருகின்றன. நீங்கள் ஸ்லிங்கிலிருந்து வெளியேறியவுடன், பாதுகாப்பாக ஓட்டுவதற்கு கையின் போதுமான இயக்கம் மற்றும் கட்டுப்பாடு மற்றும் இனி வலுவான வலி நிவாரணிகளை எடுத்துக்கொள்வதில்லை; சந்தேகம் இருந்தால், அதை உங்கள் மதிப்பாட்டில் விவாதிக்கவும்.
உங்கள் பிசியோதெரபிஸ்ட்டுக்கு:
இலக்குகள்
- முழு செயலற்ற இயக்க வரம்பை மீட்டெடுக்கவும்
- அனைத்து விமானங்களிலும் செயலில் உதவியுடன் செயலில் உள்ள இயக்க வரம்பிலிருந்து முன்னேற்றம்
- சாதாரண scapulohumeral தாளத்தை மீட்டெடுக்க மற்றும் ஈடுசெய்யும் வடிவங்களை குறைக்க
- சாதாரண ஒளி தினசரி நடவடிக்கைகளுக்கு திரும்புதல்
நிர்வாகம்
- 6 வாரங்கள் மீளாய்வில் முற்றிலுமாக நிராகரிக்கப்பட்ட ஸ்லிங்
- சுறுசுறுப்பான உதவியுடன் இயக்கம் வரம்புஃ புல்வெளி-கருவி முன்னேற்றம், அட்டவணை / சுவர் ஸ்லைடுகள், புல்லிகள், குச்சி பயிற்சிகள், வசதி அனுமதிக்கும் போது கட்டம் I வரம்புகளைத் தாண்டி முன்னேறுதல்
- 6 முதல் 8 வாரங்கள் வரையிலான செயல்திறன் கொண்ட இயக்க வரம்புஃ பின்புற வளைவு செங்குத்தாக உயரத்திற்கு முன்னேறுகிறது; பக்கவாட்டு வெளிப்புற சுழற்சி மற்றும் வளைவு; குறைந்த வரிசைகள் / குறைந்த குத்து
- சுழற்சி சுழற்சி மற்றும் டெல்டாய்டு ஐசோமெட்ரிக்ஸ் சுமார் 6 முதல் 8 வாரங்கள் வரை, பக்கவாட்டில் கை, குணமடைந்தவுடன் உறுதிப்படுத்தப்பட்டது
- லேசான முழங்கை ஐசோடோனிக்ஸ் (பிசிப்ஸ் சுருட்டைகள், ட்ரிசிப்ஸ் நீட்டிப்புகள்) மற்றும் ஸ்கேப்புலர் வலுவூட்டல் (திருப்பு, சாய்ந்த வரிசைகள்)
- சுட்டிக்காட்டப்பட்டபடி க்ளெனோஹுமரல் மற்றும் ஸ்காப்புலோதோராசிக் அணிதிரட்டுதல், குணமடையும் படிப்படியாக
- தோரணை சரிசெய்தல்; வெப்பம் / பனி மற்றும் அனல்ஜீசியாவை அமர்வுகள் முழுவதும் விரும்பியபடி தொடரவும்
எச்சரிக்கைகள்
- ஒருங்கிணைப்பு உறுதி செய்யப்படும் வரை சுழற்சி மஞ்ச் வலுவூட்டல் (ஐசோடோனிக்) எதிர்ப்பு இல்லை, பொதுவாக 812 வாரங்களுக்கு முன்னர் இல்லை
- வலுவான இறுதி வரம்பில் அதிக அழுத்தம் அல்லது ஆக்கிரமிப்பு செயலற்ற நீட்டிப்பு இல்லை
- இயக்கப்படும் கரத்துடன் சுமார் 12 கிலோ வரை மட்டுமே தூக்குதல்
- தோள்பட்டை இழுத்தல் மற்றும் தண்டு-இழுப்பு இழப்பீடு ஆகியவற்றைக் கண்காணித்து சரிசெய்யவும்
முன்னேற்றத்திற்கான அளவுகோல்கள்
- முழு, அல்லது கிட்டத்தட்ட முழு, செயலற்ற இயக்கம்
- குறைந்தபட்சம் தோள்பட்டை உயரத்திற்கு கீழே நல்ல இயந்திரத்துடன் செயலில் உயர்வு
- ஐசோமெட்ரிக்ஸ் நன்கு பொறுத்துக்கொள்ளப்படுகிறது வலி ஒரு எரியும் இல்லாமல்
- டாக்டர் ஹிர்பாராவுடன் நீங்கள் பரிசீலித்ததில் உறுதிப்படுத்தப்பட்டபடி, யூனியன் எக்ஸ்-ரே மீது முன்னேறி வருகிறது.
கட்டம் III வலுவூட்டல் (சுமார் 3 முதல் 41⁄2 மாதங்கள் வரை)
எலும்பு முறிவு ஒன்றிணைக்கப்பட்டு, உங்கள் செயலில் இயக்கம் திரும்பியவுடன், வலிமையை மீண்டும் கட்டமைப்பதில் கவனம் செலுத்தப்படுகிறது. எதிர்ப்பு வேலை மெதுவாக தொடங்குகிறது (சுழலும் மடிப்பு, டெல்டாய்டு மற்றும் தோள்பட்டை தசைகளுக்கு மீளக்கூடிய பட்டைகள் மற்றும் இலகுவான எடைகள்) மற்றும் படிப்படியாக முன்னேறுகிறது. நீட்டிப்பு தொடர்கிறது, முதுகுக்குப் பின்னால் எட்டுவது உட்பட அனைத்து திசைகளிலும் முழு இயக்கத்தை நோக்கி செயல்படுகிறது. இந்த கட்டத்தில் சாதாரண தினசரி நடவடிக்கைகள் பெரும்பாலும் வழக்கமான நிலைக்குத் திரும்ப வேண்டும், மேலும் இலகுவான பொழுதுபோக்கு நடவடிக்கைகள் வழக்கமாக உங்கள் உடற்பயிற்சி நிபுணரின் வழிகாட்டுதலின்படி மீண்டும் தொடர வேண்டும்.
உங்கள் பிசியோதெரபிஸ்ட்டுக்கு:
இலக்குகள்
- இயல்பான இயந்திரத்துடன் அனைத்து விமானங்களிலும் இயக்கத்தின் முழுமையான செயலில் வரம்பு
- ரோட்டேட்டர் மஞ்ச், டெல்டோயிட் மற்றும் ஸ்கேப்புலர் வலிமை மற்றும் சகிப்புத்தன்மையின் படிப்படியான மீட்பு
நிர்வாகம்
- ஐசோமெட்ரிக்ஸில் இருந்து எலாஸ்டிக்-பேண்ட் மற்றும் பின்னர் இலவச எடை வலுவூட்டல் (சுமார் 0.5 2 கிலோ) க்கு முன்னேற்றம்ஃ குறைந்த சுமை, அதிக மறுபரிசீலனைகள் (எடுத்துக்காட்டாக 2 3 செட் 8 12), அதிக சுமையைத் தவிர்க்க வாரத்திற்கு 3 முறை எதிர்ப்பு அமர்வுகள்
- சுழற்சி வலுவூட்டல் ஆரம்பத்தில் கை பக்கத்தில், தோள்பட்டை உயரத்திற்கு கீழே
- ஒரு நிலையான ஸ்கேப்புலர் அடித்தளத்திற்கான முன்னணி டெல்டாய்டு மற்றும் டிராபெசியஸ் செராடஸ் முன்னணி வலிமை ஜோடியை வலியுறுத்துங்கள்
- அனைத்து விமானங்களிலும் இறுதி வரம்பிற்கான நெகிழ்வுத்தன்மை திட்டம்ஃ பின்புற காப்ஸ்யூல் (கிராஸ்-பாடி) நீட்சி, பின்புற உள் சுழற்சி, முன் மார்பு சுவர் / பெக்டோரலிஸ் சிறு நீட்சிகள், கதவு நீட்சி
- உள் சுழற்சியை முதுகுக்குப் பின்னால் தொடங்குங்கள் மற்றும் தரம் III IV அணிதிரட்டுதல்கள் தூரம் அனுமதிக்கும்
- குறைந்த எதிர்ப்புடன் மேல்-உடல் எர்கோமீட்டர்; பொதுவான ஏரோபிக் கண்டிஷனிங்
எச்சரிக்கைகள்
- வலுவூட்டல் வசதியான வரம்பிற்குள் உள்ளது மற்றும் நீடித்த வலியைத் தூண்டக்கூடாது
- இந்த கட்டத்தில் 45 கிலோவுக்கு மேல் தூக்கக் கூடாது.
- அதிக எடையை கை வழியாக சுமப்பதைத் தவிர்க்கவும் (புஷ்-அப்கள் மற்றும் அதுபோன்றவை பின்னர் வரும்)
முன்னேற்றத்திற்கான அளவுகோல்கள்
- ஈடுசெய்யும் உத்திகள் இல்லாமல் முழு செயலில் இயக்கம்
- வலி அதிகரிப்பு அல்லது வரம்பு இழப்பு இல்லாமல் பொறுத்துக்கொள்ளப்பட்ட வலுவூட்டல் திட்டம்
கட்டம் IV முழு செயல்பாட்டுக்கு திரும்புதல் (சுமார் 41⁄26 மாதங்களில்)
கடைசி கட்டம் கனமான தூக்குதல், கையேடு வேலை, மேல்நிலை பணிகள் மற்றும் விளையாட்டுக்கு படிப்படியாக திரும்புவது. வலிமை வேலை கனமான எதிர்ப்பு மற்றும் கலப்பு இயக்கங்களுக்கு முன்னேறுகிறது, மேலும் இது உங்கள் வேலை அல்லது விளையாட்டுக்கு பொருத்தமானதாக இருந்தால், வேகமான, அதிக மாறும் உடற்பயிற்சிக்கு. பெரும்பாலான மக்கள் ஆறு மாதங்களுக்குள் தங்கள் வழக்கமான நடவடிக்கைகளுக்குத் திரும்புகிறார்கள், இருப்பினும் வலிமையும் நம்பிக்கையும் பொதுவாக ஒரு வருடம் வரை மேம்படுகின்றன. சரியான இறுதிக் கோடு உங்களுக்கு கை என்ன செய்ய வேண்டும் என்பதைப் பொறுத்தது, எனவே கனமான கையேடு வேலை அல்லது தொடர்பு மற்றும் மேல்நிலை விளையாட்டுக்கு திரும்புவது காலண்டரால் நிர்ணயிக்கப்படுவதை விட டாக்டர் ஹிர்பாரா மற்றும் உங்கள் உடற்பயிற்சி நிபுணருடன் ஒப்புக்கொள்ளப்படுகிறது.
உங்கள் பிசியோதெரபிஸ்ட்டுக்கு:
இலக்குகள்
- முழு வேலை, பொழுதுபோக்கு மற்றும் விளையாட்டு நடவடிக்கைகளுக்கு திரும்புதல்
- இயக்கப்படும் கையின் வலிமை மற்ற பக்கத்தின் வலிமையை நெருங்குகிறது
நிர்வாகம்
- இசைக்குழுக்கள், இலவச எடைகள் மற்றும் உடற்பயிற்சி அடிப்படையிலான கலப்பு இயக்கங்கள் மூலம் முற்போக்கான எதிர்ப்பு
- அனுமதிக்கப்பட்டபடி தள்ளுதல் முன்னேற்றம் (சுவர் → பெஞ்ச் → முழங்கால்கள் → முழு) மற்றும் மூடிய சங்கிலி ஸ்திரத்தன்மை வேலை
- ஏறக்குறைய 41⁄2 மாதங்களிலிருந்துஃ எக்ஸென்ட்ரிக் சுமை, பிளையோமெட்ரிக் (எடை கொண்ட பந்து வேலை), சுயநல மற்றும் தாள நிலைப்படுத்தல் பயிற்சிகள் தேவைப்பட்டால்
- 90° உயரத்தில் எதிர்ப்பு சுழற்சி, மற்றும் பொருத்தமான விளையாட்டு-குறிப்பிட்ட அல்லது தொழில்-குறிப்பிட்ட இடைவெளி திட்டங்கள்
எச்சரிக்கைகள்
- நோயின் முன்னேற்றம் அறிகுறிகளால் வழிநடத்தப்படுகிறது: வலி அல்லது சுற்றளவு இழப்பு மீண்டும் ஏற்பட்டால், முதலில் மெதுவாக திரும்பி, வசதியான இயக்கத்தை மீட்டெடுக்கவும்
தள்ளுபடிக்கான அளவுகோல்கள்
- இயக்கப்படும் கையின் வலிமை மற்ற பக்கத்தில் குறைந்தது சுமார் 80% அளவிடப்படுகிறது
- படிப்படியாக வலுவடையும் வலி இல்லை
- பராமரிப்பு வீட்டு திட்டத்துடன் சுயாதீனமாக
உங்கள் நெறிமுறை பிறகு
மேலே உள்ள கட்டங்கள் அருகிலுள்ள இடுப்பு எலும்பு முறிவு சரிசெய்தலுக்கான வெளியிடப்பட்ட மறுவாழ்வு நெறிமுறைகளிலிருந்து மாற்றியமைக்கப்பட்டுள்ளன: மாசசூசெட்ஸ் ஜெனரல் பிரிகாம் ஸ்போர்ட்ஸ் மெடிசின், இரட்டை நகரங்கள் எலும்பியல், யுகான் தசை மற்றும் எலும்பு நிறுவனம், NYU லாங்கன் எலும்பியல் மையம் மற்றும் சவுத் பெண்ட் எலும்பியல், அருகிலுள்ள இடுப்பு எலும்பு முறிவுக்குப் பிறகு மறுவாழ்வின் முறையான மதிப்பாய்வுடன். இந்த அறுவை சிகிச்சைக்கு வெளியிடப்பட்ட நெறிமுறைகள் பெரும்பாலான தோள்பட்டை அறுவை சிகிச்சைகளை விட வேறுபடுகின்றன, ஏனென்றால் சரியான வேகம் தனிப்பட்ட எலும்பு முறிவு எவ்வாறு சரிசெய்யப்பட்டது மற்றும் அது எவ்வாறு குணமடைகிறது என்பதைப் பொறுத்தது; எனவே கட்டங்கள் மூலம் உங்கள் முன்னேற்றம் உங்கள் மதிப்புரைகளில் டாக்டர் ஹிர்பராவால் இயக்கப்படுகிறது மற்றும் அவற்றுக்கு இடையில் உங்கள் இயற்பியல் சிகிச்சையாளரால் சரிசெய்யப்படுகிறது. இந்த பக்கம் நடைமுறையின் பொதுவான மீட்பு ஆல அறுவை சிகிச்சைக்குப் பிந்தைய வலியை நிர்வகித்தல் மற்றும் காயம் பராமரிப்புஅறுவை சிகிச்சை தொடர்பாக, காண்க அருகில் உள்ள இடுப்புத் தண்டு இணைப்பு.
இந்த நெறிமுறைக்கு பின்னால் உள்ள ஆதாரங்களை நீங்கள் படிக்க விரும்பினால் (பிளேட் பத்திரப்படுத்தலுக்குப் பிறகு ஆரம்ப மற்றும் தாமதமான இயக்கம் பற்றிய ஆராய்ச்சி, அறுவை சிகிச்சை-எதிராக-ஸ்லிங் விவாதம், மற்றும் சிக்கல்களைத் தவிர்ப்பதற்கு கட்டம் முன்னேற்றம் வடிவமைக்கப்பட்டுள்ளது), ஒரு முழுமையான குறிப்பு ஆதார சுருக்கம் இந்த பக்கத்துடன் PDF ஆக கிடைக்கிறது.
Evidence & references
Proximal Humerus Fracture Fixation (Locking-Plate ORIF) — Post-operative Rehabilitation: Evidence
Topic scope: Post-operative rehabilitation after open reduction and internal fixation (ORIF) of a proximal humerus fracture with a locking (angular-stable) plate and screws. This page covers the evidence behind the phased rehabilitation program — early protected/passive motion, deferred active and resisted motion, and graded strengthening — and the surgical-outcome facts that shape it. It does not cover the separate pathways of non-operative fracture management, intramedullary nailing, hemiarthroplasty or reverse total shoulder arthroplasty, although the operative-versus-non-operative debate is summarised because it frames who is offered this operation at all.
Defining principle of the rehab here (mobilise early, protect the tuberosities): A locking plate is an angular-stable construct — the screws lock into the plate, so the fixation holds even in osteoporotic bone without relying on bone-to-screw friction. Because that stability is present from day one, this protocol now permits early active (and active-assisted) shoulder elevation in a pain-free range for stable fixation, consistent with the early-active-motion RCT evidence (Loew 2025), rather than holding the shoulder passive-only for six weeks. The element still keyed to biological healing is rotation and rotator-cuff loading: where the tuberosity fragments to which the rotator cuff attaches are part of the fracture, active/resisted rotation and cuff work are held back until those fragments unite, whereas where the tuberosities are uninvolved or solidly fixed the surgeon may clear cuff loading sooner. The brake is therefore biological, not mechanical — the plate is strong immediately — and it is now selective (rotation/cuff), not a blanket movement ban. Progression of cuff loading remains governed by fracture stability and radiographic healing, not the calendar. This places the protocol close to the early-active-movement end of the spectrum while still being more tuberosity-aware than a pure debridement/decompression, and far less tuberosity-dependent than a fracture arthroplasty, where healing of the tuberosities to the prosthesis dictates a slower, stricter cuff-loading timetable.
The operation
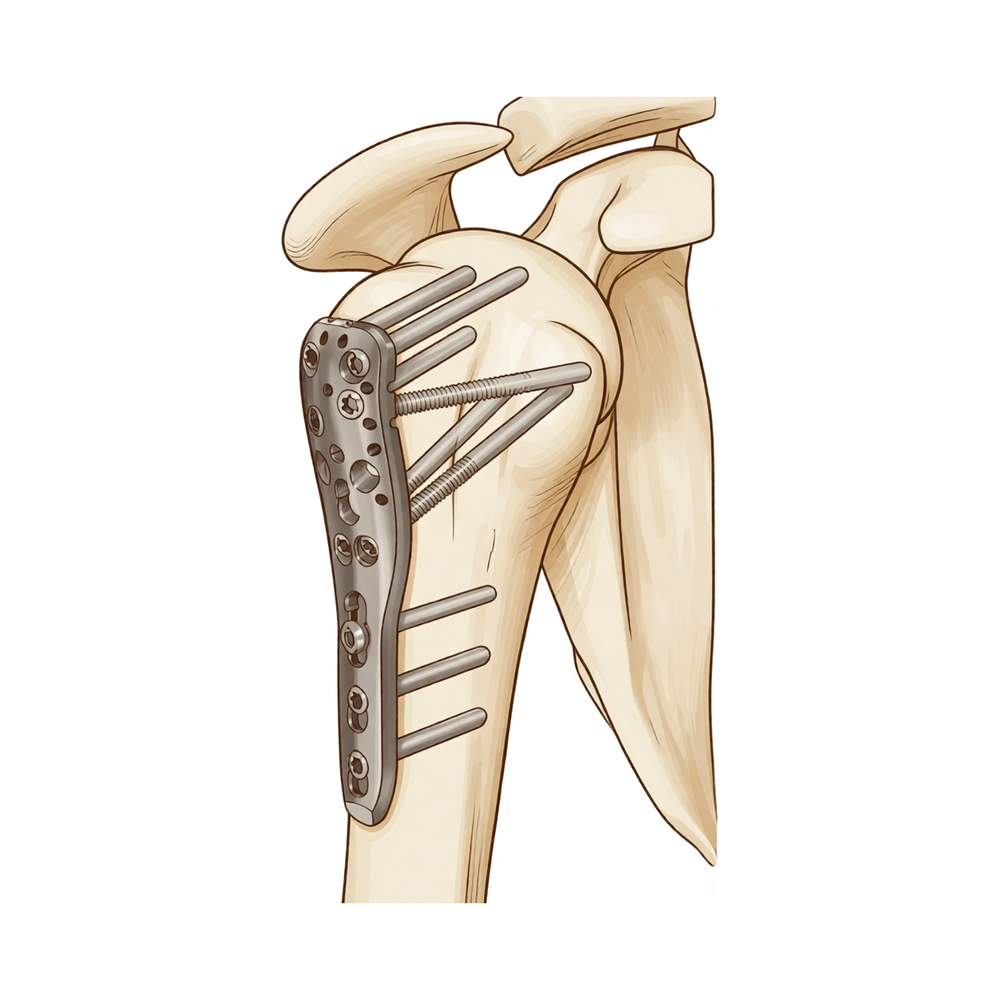
A proximal humerus fracture is a break of the upper end of the arm bone, near the shoulder. In ORIF the fragments are realigned (reduced) and held with a pre-contoured locking plate on the outer surface of the bone, fixed with multiple locking screws into the humeral head. Where the tuberosities (the bony knobs carrying the rotator-cuff attachments) are part of the fracture, they are reduced and secured to the plate, often reinforced with heavy sutures through the cuff. The plate provides immediate mechanical stability; the rehabilitation then protects the biological healing of the fracture and the tuberosity fragments.
Evidence by theme
1. Modern locking plates permit early active motion — supported by RCT evidence and adopted here for stable fixation
The historical "restrictive" protocol kept the arm immobilised with no active movement for ~6 weeks, with passive limits of flexion to ~90°, external rotation to ~20° and internal rotation to the belly. The rationale for early motion is to prevent the shoulder stiffening (adhesive capsulitis is a recognised complication of these fractures) while still protecting the bone. Because an angular-stable locking plate is mechanically strong from day one, early active elevation can be permitted for stable fixation; the element kept keyed to biological healing is rotation and rotator-cuff loading, because that is what pulls on the tuberosity fragments.
The more aggressive question — can patients move actively from the start? — has now been tested. A prospective randomised controlled trial (Loew et al., J Orthop, 2025) compared a conventional 4-week sling-immobilisation group against an early functional group with no movement or force restrictions after locking-plate ORIF (both groups avoided heavy lifting and impact for 3 months). At 24 months there was no significant difference in DASH or Constant score: Constant score averaged 81.3 (conventional) vs 78.4 (early functional), with relative Constant score 89.8% of the uninjured side in both groups — i.e. early active motion was non-inferior. Moderate (single RCT). This is consistent with the broader signal that early intensive mobilisation yields similar outcomes to conventional later mobilisation after operative treatment. In line with this evidence, Dr Hirpara's protocol now permits early active elevation in a pain-free range for stable fixation; the literature still has no consensus on the optimal regimen, so the one element kept deliberately cautious and keyed to radiographic healing is active/resisted rotation and rotator-cuff loading, because that is the movement that stresses the healing tuberosity fragments.
2. Post-operative protocols are highly heterogeneous, but converge on short immobilisation and early passive ROM
The best summary of practice is a systematic review of 45 cohorts (40 articles, 3,507 patients, 3,519 fractures) (Budharaju et al., Shoulder Elbow, 2024). Across studies:
- Sling immobilisation averaged 3.1 weeks (most commonly 3 weeks; range 0–6).
- Passive ROM began at ~0.9 weeks on average (most commonly at 2 days).
- Active ROM began at ~2.5 weeks on average (most commonly at 3 weeks).
- Strengthening began at ~5.5 weeks on average (most commonly at 6 weeks).
The authors emphasised substantial variability regardless of management, concluded that this heterogeneity limits cross-study comparison, and noted that early mobilisation may produce superior function — supporting consideration of shorter immobilisation. The synthesis page's "~3 weeks in the sling, then wean" reflects this averaged convention, not a trial-proven optimum. Moderate for the descriptive pattern; weak/consensus for any specific timetable.
3. Progression is governed by fracture stability and healing, not the calendar — because of the tuberosities and biological complications
The locking plate is strong immediately; what limits the rehab is the bone. Two facts anchor the "wait-for-healing" rule:
- Tuberosity / cuff loading. When the tuberosities are part of the fracture, loading the rotator cuff (forced/resisted external rotation and resisted cuff work) too early risks displacing fragments before they unite. This is the explicit reason the early phases keep rotation cautious and defer cuff loading until healing, even though early active elevation in a pain-free range is permitted; where the tuberosities are uninvolved or solidly fixed, the surgeon may clear cuff loading sooner.
- The major complications of locking-plate ORIF are largely biological and mechanical, and several are loading- and reduction-sensitive. A systematic review (Thanasas / Brorson-class series) reports the commonest complications as intra-articular screw perforation (~9–12%), varus collapse (~6.8%), loss of reduction, avascular necrosis of the humeral head (~4.6%, reported range 0–15%), subacromial impingement (~5%), adhesive capsulitis (~4%), nonunion (~1.5%) and deep infection (~1.4%). Screw perforation and avascular necrosis frequently coincide, because a head that collapses or undergoes AVN lets fixed-length locked screws migrate into the joint. Moderate (pooled observational series).
This complication profile is why progression waits on radiographs: premature loading risks tipping a borderline reduction into varus collapse or screw cut-out. Some surgeons even advocate early planned plate removal to avoid secondary screw penetration once the head shows AVN/collapse (Dimitriou et al., J Orthop, 2019) — a salvage strategy, not part of routine rehab, but it illustrates how mechanical and biological failure interact.
4. Who is offered ORIF at all — the operative-versus-non-operative debate (PROFHER and after)
The single most influential trial is PROFHER (Rangan et al., JAMA, 2015; 250 patients, 32 UK centres, displaced fractures involving the surgical neck): surgery showed no important difference in Oxford Shoulder Score versus sling-based non-operative care over 2 years, and was more expensive. The 5-year follow-up (Handoll/Keding et al., Bone Joint J, 2017) confirmed no significant difference in shoulder function or quality of life persisting to 5 years. A smaller RCT in displaced 3-part fractures in the elderly (Fjalestad et al., J Shoulder Elbow Surg, 2012) similarly found no functional advantage to internal fixation over non-operative care in that group, and a systematic review and meta-analysis (Beks et al., J Shoulder Elbow Surg, 2018) found no clear superiority of operative treatment across observational and randomised data combined. Strong (multiple RCTs + SR-MA).
The clinical upshot — and the reason this matters to a rehab page — is that ORIF is selectively indicated, typically in younger patients, in fractures where reduction and stable fixation are achievable and worthwhile, and where the alternative (non-operative care or arthroplasty) is judged less favourable. The decision is individualised; "difficulty in decision-making" for displaced fractures is itself documented as affecting outcomes (Okike et al., J Shoulder Elbow Surg, 2018). Patients should understand that being offered ORIF is a considered judgement, not an automatic consequence of the fracture.
5. Adjacent rehabilitation evidence (non-operative immobilisation duration)
Although it concerns non-operatively treated fractures, a relevant randomised controlled trial (Tanji et al., J Bone Joint Surg Am, 2021) compared 1 versus 3 weeks of immobilisation and supports the broad theme that earlier movement is at least as good as longer immobilisation for many proximal humerus fractures. It does not directly govern the post-ORIF protocol but reinforces the same direction-of-travel away from prolonged slings. Moderate (RCT, non-operative population).
Phased post-operative timeline (consistent with the synthesis page)
| Phase | Window | Sling | Shoulder motion | Strengthening | Governing rule |
|---|---|---|---|---|---|
| I — Protection & early passive motion | Weeks 0–6 | Full-time ~3 weeks, then weaned; off for exercises/hygiene; not in bed | Early active-assisted/active elevation permitted in a pain-free range from the outset (supine-start → upright); passive as needed; pendulums; elbow/wrist/hand active. ER kept to a gentle ~30–40° default; rotation cautious — defer active/resisted cuff work until tuberosities heal (surgeon-guided) | None at the shoulder (deltoid/periscapular isometrics as comfort allows) | Protect fixation + tuberosities; settle pain/swelling |
| II — Regaining active movement | Weeks 6–12 | Discarded by the 6-week review at the latest | Active-assisted → active in all planes (supine-start elevation); submaximal cuff/deltoid isometrics once healing confirmed | Light elbow/scapular work; no resisted cuff work until union (typically not before 8–12 weeks) | Radiographic healing at the ~6-week review gates active motion |
| III — Strengthening | ~Months 3–4½ | Off | Full active ROM in all planes, including behind-the-back | Graded bands → light free weights (~0.5–2 kg) for cuff, deltoid, scapula | Union confirmed; symptom-guided load progression |
| IV — Return to full activity | ~4½–6 months | Off | Full, with dynamic/overhead drills as relevant | Heavier resistance, compound + sport/work-specific | Return-to-task agreed with surgeon/physio, not the calendar |
The phase boundaries are individualised at Dr Hirpara's reviews on the basis of X-ray healing — this is the operative consequence of the "stability- and healing-governed, not calendar-governed" principle.
Key controversies / evidence quality
-
Early active versus delayed (protected) mobilisation after ORIF. A single RCT (Loew 2025) found unrestricted early active motion non-inferior to 4-week immobilisation at 24 months, and the broader literature leans toward shorter immobilisation. The protocol here aligns with that early-active-motion evidence: early active and active-assisted elevation in a pain-free range is permitted for stable fixation, rather than holding the shoulder passive-only for six weeks. Because there is still no consensus and no large confirmatory trial (protocols remain heterogeneous — Budharaju 2024), the protocol keeps one deliberate, evidence-aware caution: active/resisted rotation and cuff loading is keyed to radiographic tuberosity healing rather than released wholesale on day one. Moderate evidence, unsettled.
-
Operative versus non-operative treatment of displaced fractures. PROFHER (2015) and its 5-year follow-up (2017), plus an elderly-3-part RCT (Fjalestad 2012) and a meta-analysis (Beks 2018), found no clear functional benefit of surgery on average — which is why ORIF is selectively, not routinely, offered. The trials enrolled broad/older populations; the subgroup most likely to benefit from fixation (younger patients, good bone, reconstructable head-preserving fractures) is exactly where this operation is concentrated. Strong evidence overall; subgroup benefit remains debated.
-
The post-operative rehab protocol itself is consensus/expert. No high-level RCT defines the optimal phase structure, ROM limits or strengthening onset after ORIF. The timings here are drawn from published surgeon protocols and the systematic-review averages, individualised at review. Weak/consensus.
Evidence-strength flags (summary)
- STRONG (RCT / SR-MA): operative versus non-operative equivalence on average for displaced fractures (PROFHER 2-yr JAMA 2015 + 5-yr Bone Joint J 2017; Fjalestad 2012 RCT; Beks 2018 SR-MA).
- MODERATE (single RCT / pooled series): early active motion non-inferior to immobilisation after ORIF at 24 months (Loew 2025 RCT); 1-vs-3-week immobilisation non-operatively (Tanji 2021 RCT); locking-plate complication profile — screw perforation, varus collapse, AVN, etc. (pooled observational series); descriptive practice pattern of short sling + early passive ROM (Budharaju 2024 SR of 45 cohorts).
- WEAK / CONSENSUS: the specific phased rehabilitation timetable after ORIF (no defining rehab RCT; published surgeon protocols + systematic-review averages; progression individualised by radiographic healing).
Citations
RAG corpus (180,000+ Orthopaedic articles) — real DOIs
- Five-year follow-up results of the PROFHER trial comparing operative and non-operative treatment of adults with a displaced fracture of the proximal humerus. Bone Joint J. 2017. DOI: 10.1302/0301-620x.99b3.bjj-2016-1028
- Operative versus nonoperative treatment of proximal humeral fractures: a systematic review, meta-analysis, and comparison of observational studies and randomized controlled trials. J Shoulder Elbow Surg. 2018. DOI: 10.1016/j.jse.2018.03.009
- Internal fixation versus nonoperative treatment of displaced 3-part proximal humeral fractures in elderly patients: a randomized controlled trial. J Shoulder Elbow Surg. 2012. DOI: 10.1016/j.jse.2010.12.018
- One Versus 3-Week Immobilization Period for Nonoperatively Treated Proximal Humeral Fractures: a randomized controlled trial. J Bone Joint Surg Am. 2021. DOI: 10.2106/jbjs.20.02137
- Contemporary Management of Proximal Humeral Fractures. J Am Acad Orthop Surg. 2024. DOI: 10.5435/jaaos-d-24-01073
- The Use of Precontoured Humeral Locking Plates in the Management of Displaced Proximal Humerus Fracture. J Am Acad Orthop Surg. 2009. DOI: 10.5435/00124635-200909000-00005
- Use of locking plates in the treatment of proximal humerus fractures. J Shoulder Elbow Surg. 2010. DOI: 10.1016/j.jse.2010.01.001
- Functional results and unfavorable events after treatment of proximal humerus fractures using a new locking plate system. BMC Musculoskelet Disord. 2023. DOI: 10.1186/s12891-023-06176-5
- Fracture site augmentation with calcium phosphate cement reduces screw penetration after open reduction–internal fixation of proximal humeral fractures. J Shoulder Elbow Surg. 2012. DOI: 10.1016/j.jse.2011.09.017
- Difficulty in decision making in the treatment of displaced proximal humerus fractures: the effect of uncertainty on surgical outcomes. J Shoulder Elbow Surg. 2018. DOI: 10.1016/j.jse.2017.09.033
Literature (URLs)
- Loew M, et al. Postoperative treatment of proximal humerus fractures with an early active motion protocol: a prospective randomized controlled trial. J Orthop. 2025. https://www.sciencedirect.com/science/article/pii/S1058274625001867 (Constant 81.3 conventional vs 78.4 early-functional at 24 months; early active motion non-inferior)
- Budharaju A, Hones KM, Hao KA, et al. Rehabilitation protocols in proximal humerus fracture management: a systematic review. Shoulder Elbow. 2024;16(4):449–458. https://pmc.ncbi.nlm.nih.gov/articles/PMC11437559/ (45 cohorts; sling 3.1 wk, passive 0.9 wk, active 2.5 wk, strengthening 5.5 wk; early mobilisation may improve function)
- Rangan A, et al. (PROFHER). Surgical vs nonsurgical treatment of adults with displaced fractures of the proximal humerus: the PROFHER randomized clinical trial. JAMA. 2015;313(10):1037–1047. https://pubmed.ncbi.nlm.nih.gov/25756440/ (250 patients; no important difference in Oxford Shoulder Score at 2 years)
- Complications associated with locking plate of proximal humerus fractures (systematic review of complication rates). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC5858203/ (screw perforation ~9–12%, varus collapse ~6.8%, AVN ~4.6%)
- Avascular necrosis and posttraumatic arthritis after proximal humerus fracture internal fixation: evaluation and management. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC9889581/ (AVN reported range 0–15%)
- Late screw-related complications in locking plating of proximal humerus fractures: a systematic review. Injury. https://www.sciencedirect.com/science/article/abs/pii/S0020138319306989
- Dimitriou D, et al. Early locking plate removal following ORIF of proximal humeral fractures could prevent secondary implant-related complications. J Orthop. 2019;17:106–109. https://pmc.ncbi.nlm.nih.gov/articles/PMC6919395/
Published rehabilitation protocols (patient-guidance — basis for the phase structure)
- Massachusetts General Brigham Sports Medicine. Rehabilitation Protocol for Proximal Humeral Fracture Open Reduction Internal Fixation (ORIF). https://www.massgeneral.org/assets/MGH/pdf/orthopaedics/sports-medicine/physical-therapy/rehabilitation-protocol-for-proximal-humeral-fracture-with-ORIF.pdf
- LaPrade CM. Post-Surgical Physical Therapy Protocol: Proximal Humerus Fracture ORIF. Twin Cities Orthopedics. https://tcomn.com/wp-content/uploads/2024/08/CML_Proximal-Humerus-ORIF-PT_10-2024.pdf
- Coyner KJ. ORIF Proximal Humerus Fractures Protocol. UConn Musculoskeletal Institute. https://www.drcoyner.com/pdf/orif-proximal-humerus-fractures-protocol.pdf
- Jazrawi LM. Rehabilitation Protocol: Proximal Humerus Open Reduction & Internal Fixation (ORIF). NYU Langone Orthopedic Center. https://www.newyorkortho.com/pdf/proximal-humerus-fracture-orif-post-op-instructions-and-rehab.pdf
- South Bend Orthopaedics. ORIF Proximal Humerus Fracture Rehab Protocol. https://www.sbortho.com/wp-content/uploads/2023/09/br-pt-fracture-orif-proximal-humerus.pdf





