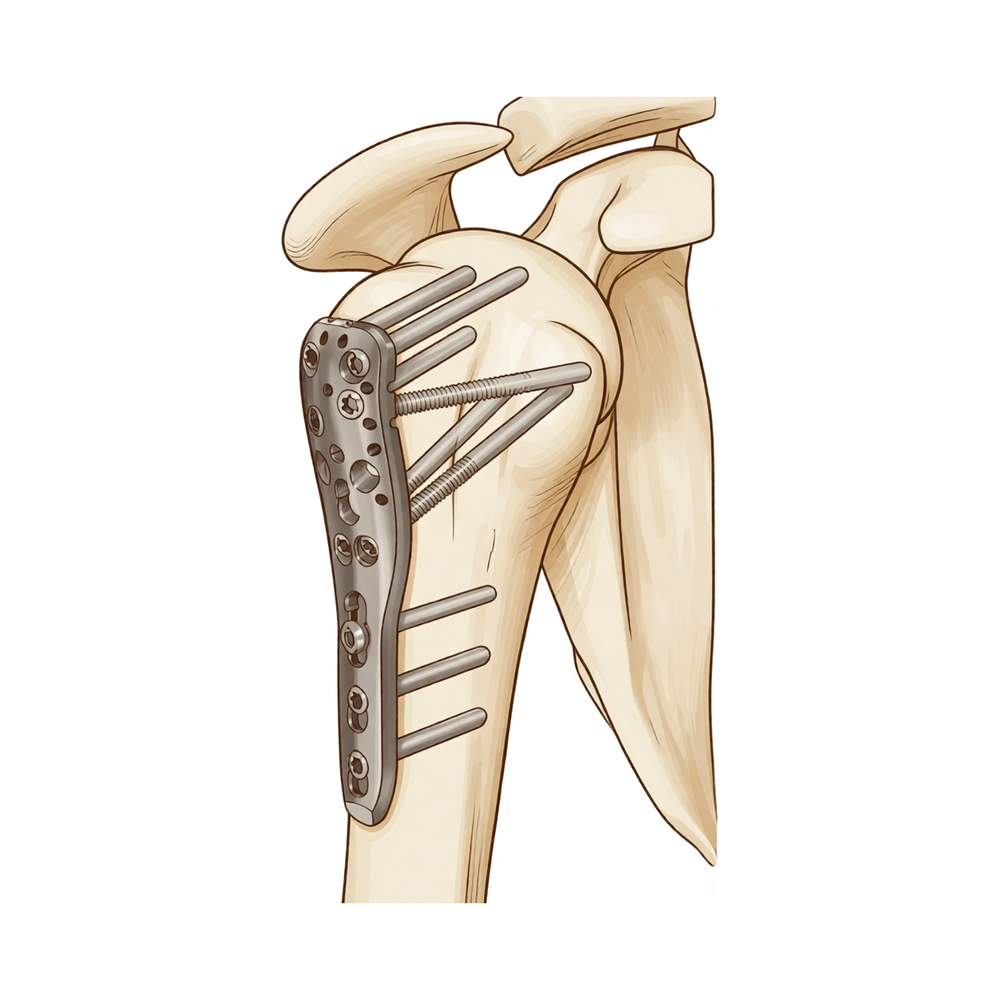
肱骨近端切开复位内固定术(ORIF)
Patients › Rehabilitation
Rehabilitation after locking-plate fixation of a proximal humerus fracture, gated on radiographic healing at review.
本方案涵盖基兰·希尔帕拉(Kieran Hirpara)医生在罗克汉普顿 Mater 私人医院进行的肱骨近端骨折(上臂靠近肩部的骨折,采用锁定钢板和螺钉进行修复,即切开复位内固定术,ORIF)术后康复。请在首次物理治疗就诊时携带此页面或其 PDF 文件,以确保康复过程协调一致。您的物理治疗师将根据骨折愈合情况,通过以下阶段为您个体化推进康复。
如果术后对伤口有任何疑虑,请联系诊室。拍摄伤口照片并发送电子邮件供审查通常很有帮助。
预期情况
骨折固定术后的康复与大多数计划中的肩部手术后的康复方式不同。钢板和螺钉将骨折断端固定在位,但骨骼本身仍需愈合,且愈合速度因人而异。因此,以下时间表仅为典型指南,而非固定日程:您进入下一阶段取决于术后周数以及X光片显示的骨折愈合情况,并由Hirpara医生在复查时确认。切勿仅凭日历自行进入下一阶段;请等待复查。
还有另一件事使该手术与众不同。肱骨顶端的骨性突起(结节)是肩袖肌腱的附着点,在许多肱骨近端骨折中,这些碎片是骨折的一部分,并通过钢板或缝线固定回去。过早或过度用力活动肩袖肌腱可能会在碎片愈合前将其牵拉。使用现代锁定钢板时,固定从第一天起就很牢固,因此鼓励早期进行轻柔活动:您可以尽早进行主动辅助活动和轻柔的主动活动,在无疼痛范围内抬高手臂。谨慎之处在于肩袖负荷:如果结节碎片不是骨折的一部分,或者固定牢固,您的外科医生可能会允许您更早开始主动旋转和肩袖训练;如果结节受累且正在愈合,则需稍晚一些才进行主动肩袖训练和强制外旋。Hirpara医生会告知您适用哪种情况。
您的锻炼计划使用三种类型的活动,您的医疗团队将标记适用于您的类型:
- 主动活动范围: 无需辅助或帮助即可进行的活动。
- 主动辅助活动范围: 使用另一只手臂或物体辅助移动手臂。
- 被动活动范围: 完全放松,使用另一只手臂或外力完成100%的工作。
您将从手术中醒来,手臂置于吊带中。在前三周左右全天佩戴,随后在舒适允许的情况下逐渐减少佩戴时间;已发表的方案平均 immobilisation(制动)时间为三周左右,且证据支持比长时间佩戴吊带更早开始活动。您睡觉时无需佩戴。每天多次取下吊带进行锻炼、洗漱和穿衣,在家安静坐着时,您可以将手臂移出吊带休息。佩戴吊带期间请勿驾驶。
简要概览:
- 第一阶段 — 保护与早期被动活动: 第0–6周
- 第二阶段 — 恢复主动活动: 第6–12周
- 第三阶段 — 强化训练: 约第3至4.5个月
- 第四阶段 — 恢复全面活动: 约从4.5–6个月起
第一阶段——保护与早期被动活动(第0–6周)
前六周的重点是在保护骨折固定端的同时,防止手臂其余部分(包括肩关节本身)僵硬。由于锁定钢板从一开始就能牢固固定骨骼,因此鼓励进行温和的早期活动,而不是等待六周。在您出院前,物理治疗师将开始指导您进行温和的练习:钟摆运动(让手臂自然下垂,通过摆动身体轻轻摇晃),以及每天多次将肘部、手腕和手部从悬吊带中取出进行活动。从早期开始,在舒适且无痛的范围内,您可以开始借助另一只手帮助移动手臂(主动辅助),并在舒适允许的范围内轻轻自主发力(主动)向前抬起手臂。谨慎之处在于肩袖负荷:正如Hirpara医生所确认的,在结节愈合之前,应避免强行向外旋转手臂(外旋),并避免进行抗阻肩袖训练。使用冰敷缓解疼痛,并在进行锻炼和物理治疗预约前服用止痛药。
致物理治疗师:
目标
- 保护内固定并优化骨愈合
- 控制疼痛和肿胀
- 在无痛范围内建立早期主动辅助活动,并逐步过渡到主动抬高
- 保持颈部、肘部、手腕和手部的全范围活动
管理措施
- 全天佩戴悬吊带约3周,随后根据舒适度逐步减少使用(文献惯例);每天多次取下进行锻炼和清洁;卧床时不需要佩戴
- 每天多次进行钟摆/Codman运动
- 对于固定稳定的情况,从一开始就在舒适、无痛的范围内进行早期主动辅助和轻柔的主动前屈抬高;从仰卧位开始抬高,随着控制能力的提高逐渐过渡到直立位;根据舒适度增加活动范围
- 在尚不能耐受主动活动时,按需进行被动活动范围训练:在肩胛平面内前屈抬高至约90°,内旋至腹部(不可置于背后)
- 外旋保持在早期温和的默认角度,即手臂置于体侧时约30–40°;若结节未受累或固定牢固,主刀医生可能会增加此角度
- 在悬吊带外进行颈部、肘部、手腕和手部的主动活动范围训练;进行球类挤压以锻炼握力
- 进行肩胛骨定位和肩胛骨灵活性训练(上提、下沉、后缩、前伸)
- 根据舒适度,可引入轻柔的三角肌和肩周肌群等长收缩训练
- 治疗前进行冷疗和镇痛;伤口愈合后进行瘢痕松动和脱敏处理
注意事项
- 在结节愈合得到确认之前(由主刀医生指导),避免强行或抗阻外旋及重度肩袖负荷;允许在无痛范围内进行主动抬高
- 禁止将手臂内旋至背后;避免在冠状面进行外展
- 保持早期活动无痛:动作轻柔且在舒适范围内,不可强行
- 患侧手臂提举重量不超过约0.5–1公斤
- 患侧手臂禁止负重(禁止从椅子或床上推起身体)
- 佩戴悬吊带期间禁止驾驶
- 禁止强行或引起疼痛的终末端活动
进展标准
- 影像学显示愈合进展,并在约6周时由Hirpara医生复查确认
- 疼痛控制良好
- 保持肘部、手腕和手部的全范围活动
- 在无痛范围内,主动辅助至主动抬高感到舒适
第二阶段——恢复主动活动(第6–12周)
在约六周的复查时,Hirpara 医生会检查您的X光片。如果愈合进展符合预期,将停止使用剩余时间的悬吊带,并开始自行活动手臂,首先是在辅助下活动(使用另一只手臂、手杖或滑轮),然后是主动活动。通常仰卧位开始主动抬臂效果最佳,因为此时重力影响较小,随着控制能力的提高,再逐渐过渡到坐位和站立位。一旦 Hirpara 医生确认愈合情况,即可在此阶段开始肩袖的轻柔肌肉等长收缩(等长)练习;抗阻练习则稍后进行。当您已脱离悬吊带,手臂具备足够的活动度和控制能力以安全驾驶,且不再服用强效止痛药时,即可恢复驾驶;如有疑问,请在复查时讨论。
致您的物理治疗师:
目标
- 恢复完全的被动手臂活动范围
- 在所有平面上从主动辅助活动进展至主动活动范围
- 重建正常的肩肱节律,最小化代偿模式
- 恢复正常轻度的日常活动
管理
- 最迟在6周复查时完全弃用悬吊带
- 主动辅助活动范围:躺椅式进展、桌面/墙壁滑动、滑轮、手杖练习,在舒适允许的情况下进展超出第一阶段的限制
- 约6–8周开始主动活动范围:仰卧位屈曲进展至直立位上举;侧卧位外旋和屈曲;低拉/低冲拳
- 约6–8周开始次最大强度的肩袖和三角肌等长收缩练习,手臂置于体侧,需在确认愈合后进行
- 轻度肘部等张练习(二头肌弯举、三头肌伸展)和肩胛骨强化练习(后缩、俯卧划船)
- 根据需要实施盂肱关节和肩胸关节松动术,随愈合进展调整手法等级
- 姿势矫正;根据偏好,在治疗前后继续使用热敷/冷敷及镇痛药
注意事项
- 在确认骨性愈合前,禁止进行抗阻(等张)肩袖强化练习,通常不早于8–12周
- 禁止用力进行终末端被动加压或激进的被动拉伸
- 患肢提举重量限制在约1–2公斤
- 观察并纠正上举时的耸肩和躯干侧倾代偿
进展标准
- 完全或接近完全的被动手臂活动范围
- 主动上举具备良好的力学机制,至少低于肩高
- 等长收缩耐受良好,无疼痛加剧
- X光片显示愈合进展,并经与 Hirpara 医生的复查确认
第三阶段——强化训练(约第3至4.5个月)
随着骨折愈合及主动活动度恢复,重点转向重建肌力。抗阻训练从轻柔开始(使用弹力带和轻重量针对肩袖、三角肌及肩胛骨肌肉),并逐步增加强度。拉伸训练同步进行,旨在实现所有方向上的完全活动度,包括手背至腰后的动作。在此阶段,日常活动应基本恢复正常,较轻的休闲活动通常也可在物理治疗师的指导下恢复。
致物理治疗师:
目标
- 所有平面内完全主动活动度,且生物力学正常
- 渐进式恢复肩袖、三角肌及肩胛肌的力量与耐力
管理
- 从等长收缩过渡至弹力带及轻重量自由重量强化训练(约0.5–2公斤),针对肩袖、三角肌及肩胛稳定肌:低负荷、高重复次数(例如2–3组,每组8–12次),每周约3次抗阻训练,以避免过度负荷
- 旋转强化训练初期手臂置于体侧,低于肩高
- 强调前三角肌与斜方肌-前锯肌力偶,以建立稳定的肩胛基底
- 所有平面终末活动度的灵活性训练:后关节囊(跨胸)拉伸、背后内旋拉伸、前胸壁/胸小肌拉伸、门框拉伸
- 根据活动度情况,开始背后内旋训练及III–IV级关节松动术
- 上肢功率自行车低阻力训练;一般有氧体能训练
注意事项
- 强化训练应在舒适范围内进行,不应引发持续性疼痛
- 此阶段患肢避免提举超过约4–5公斤的重物
- 避免手臂过度负重(俯卧撑及类似动作延后)
进阶标准
- 所有平面内完全主动活动度,无代偿策略
- 强化训练耐受良好,无疼痛加剧或活动度丧失
第四阶段 — 恢复全面活动(约4½–6个月起)
最终阶段是逐步恢复较重的提举、体力工作、 overhead 任务及运动。力量训练逐步增加至更大阻力及复合动作,并根据您的工作或运动需求,过渡至更快、更具动态性的练习。大多数人约在6个月时恢复日常活动,尽管力量与信心通常可持续改善长达1年。最终目标取决于手臂所需完成的功能,因此,恢复重体力工作或接触性及 overhead 运动需与Hirpara医生及您的物理治疗师共同商定,而非仅依据日历时间。
致您的物理治疗师:
目标
- 恢复全面工作、休闲及运动活动
- 患侧手臂力量接近对侧
管理
- 通过弹力带、自由重量及健身房复合动作进行渐进性抗阻训练
- 俯卧撑进阶(墙壁 → 长凳 → 跪姿 → 标准)及闭链稳定性训练,根据耐受情况逐步进行
- 约4½个月起:离心负荷、增强式训练(负重球练习)、本体感觉及节奏性稳定训练(如适用)
- 90°上举位抗阻旋转,以及根据情况制定的分阶段专项运动或职业特定训练计划
注意事项
- 进展以症状为导向:若疼痛或活动度丧失复发,应退阶并首先恢复无痛活动范围
出院标准
- 患侧手臂力量至少达到对侧的约80%(经测量)
- 渐进性力量训练时无疼痛
- 能独立完成维持性家庭训练计划
术后方案
上述阶段改编自已发表的肱骨近端骨折固定康复方案:马萨诸塞州总医院布里格姆运动医学科、双子城骨科、康涅狄格大学肌肉骨骼研究所、纽约大学朗格尼骨科中心以及南本德骨科,并结合了肱骨近端骨折术后康复的系统综述。该手术的已发表方案差异较大多数肩关节手术更大,因为合适的进度取决于个体骨折的固定方式及其愈合情况;因此,您在各阶段的进展由Hirpara医生在复查时指导,并在复查间隙由您的物理治疗师进行调整。本页面与诊所的一般康复建议配合使用;请参阅术后疼痛管理和伤口护理。关于手术本身,请参阅肱骨近端固定术。
如果您希望了解本方案背后的循证依据(关于钢板固定后早期活动与延迟活动的研究、手术与悬吊带治疗的争议,以及分阶段进展旨在避免的并发症),一份带有完整参考文献的循证摘要可作为PDF文件与本页面一同提供。
Evidence & references
Proximal Humerus Fracture Fixation (Locking-Plate ORIF) — Post-operative Rehabilitation: Evidence
Topic scope: Post-operative rehabilitation after open reduction and internal fixation (ORIF) of a proximal humerus fracture with a locking (angular-stable) plate and screws. This page covers the evidence behind the phased rehabilitation program — early protected/passive motion, deferred active and resisted motion, and graded strengthening — and the surgical-outcome facts that shape it. It does not cover the separate pathways of non-operative fracture management, intramedullary nailing, hemiarthroplasty or reverse total shoulder arthroplasty, although the operative-versus-non-operative debate is summarised because it frames who is offered this operation at all.
Defining principle of the rehab here (mobilise early, protect the tuberosities): A locking plate is an angular-stable construct — the screws lock into the plate, so the fixation holds even in osteoporotic bone without relying on bone-to-screw friction. Because that stability is present from day one, this protocol now permits early active (and active-assisted) shoulder elevation in a pain-free range for stable fixation, consistent with the early-active-motion RCT evidence (Loew 2025), rather than holding the shoulder passive-only for six weeks. The element still keyed to biological healing is rotation and rotator-cuff loading: where the tuberosity fragments to which the rotator cuff attaches are part of the fracture, active/resisted rotation and cuff work are held back until those fragments unite, whereas where the tuberosities are uninvolved or solidly fixed the surgeon may clear cuff loading sooner. The brake is therefore biological, not mechanical — the plate is strong immediately — and it is now selective (rotation/cuff), not a blanket movement ban. Progression of cuff loading remains governed by fracture stability and radiographic healing, not the calendar. This places the protocol close to the early-active-movement end of the spectrum while still being more tuberosity-aware than a pure debridement/decompression, and far less tuberosity-dependent than a fracture arthroplasty, where healing of the tuberosities to the prosthesis dictates a slower, stricter cuff-loading timetable.
The operation
A proximal humerus fracture is a break of the upper end of the arm bone, near the shoulder. In ORIF the fragments are realigned (reduced) and held with a pre-contoured locking plate on the outer surface of the bone, fixed with multiple locking screws into the humeral head. Where the tuberosities (the bony knobs carrying the rotator-cuff attachments) are part of the fracture, they are reduced and secured to the plate, often reinforced with heavy sutures through the cuff. The plate provides immediate mechanical stability; the rehabilitation then protects the biological healing of the fracture and the tuberosity fragments.
Evidence by theme
1. Modern locking plates permit early active motion — supported by RCT evidence and adopted here for stable fixation
The historical "restrictive" protocol kept the arm immobilised with no active movement for ~6 weeks, with passive limits of flexion to ~90°, external rotation to ~20° and internal rotation to the belly. The rationale for early motion is to prevent the shoulder stiffening (adhesive capsulitis is a recognised complication of these fractures) while still protecting the bone. Because an angular-stable locking plate is mechanically strong from day one, early active elevation can be permitted for stable fixation; the element kept keyed to biological healing is rotation and rotator-cuff loading, because that is what pulls on the tuberosity fragments.
The more aggressive question — can patients move actively from the start? — has now been tested. A prospective randomised controlled trial (Loew et al., J Orthop, 2025) compared a conventional 4-week sling-immobilisation group against an early functional group with no movement or force restrictions after locking-plate ORIF (both groups avoided heavy lifting and impact for 3 months). At 24 months there was no significant difference in DASH or Constant score: Constant score averaged 81.3 (conventional) vs 78.4 (early functional), with relative Constant score 89.8% of the uninjured side in both groups — i.e. early active motion was non-inferior. Moderate (single RCT). This is consistent with the broader signal that early intensive mobilisation yields similar outcomes to conventional later mobilisation after operative treatment. In line with this evidence, Dr Hirpara's protocol now permits early active elevation in a pain-free range for stable fixation; the literature still has no consensus on the optimal regimen, so the one element kept deliberately cautious and keyed to radiographic healing is active/resisted rotation and rotator-cuff loading, because that is the movement that stresses the healing tuberosity fragments.
2. Post-operative protocols are highly heterogeneous, but converge on short immobilisation and early passive ROM
The best summary of practice is a systematic review of 45 cohorts (40 articles, 3,507 patients, 3,519 fractures) (Budharaju et al., Shoulder Elbow, 2024). Across studies:
- Sling immobilisation averaged 3.1 weeks (most commonly 3 weeks; range 0–6).
- Passive ROM began at ~0.9 weeks on average (most commonly at 2 days).
- Active ROM began at ~2.5 weeks on average (most commonly at 3 weeks).
- Strengthening began at ~5.5 weeks on average (most commonly at 6 weeks).
The authors emphasised substantial variability regardless of management, concluded that this heterogeneity limits cross-study comparison, and noted that early mobilisation may produce superior function — supporting consideration of shorter immobilisation. The synthesis page's "~3 weeks in the sling, then wean" reflects this averaged convention, not a trial-proven optimum. Moderate for the descriptive pattern; weak/consensus for any specific timetable.
3. Progression is governed by fracture stability and healing, not the calendar — because of the tuberosities and biological complications
The locking plate is strong immediately; what limits the rehab is the bone. Two facts anchor the "wait-for-healing" rule:
- Tuberosity / cuff loading. When the tuberosities are part of the fracture, loading the rotator cuff (forced/resisted external rotation and resisted cuff work) too early risks displacing fragments before they unite. This is the explicit reason the early phases keep rotation cautious and defer cuff loading until healing, even though early active elevation in a pain-free range is permitted; where the tuberosities are uninvolved or solidly fixed, the surgeon may clear cuff loading sooner.
- The major complications of locking-plate ORIF are largely biological and mechanical, and several are loading- and reduction-sensitive. A systematic review (Thanasas / Brorson-class series) reports the commonest complications as intra-articular screw perforation (~9–12%), varus collapse (~6.8%), loss of reduction, avascular necrosis of the humeral head (~4.6%, reported range 0–15%), subacromial impingement (~5%), adhesive capsulitis (~4%), nonunion (~1.5%) and deep infection (~1.4%). Screw perforation and avascular necrosis frequently coincide, because a head that collapses or undergoes AVN lets fixed-length locked screws migrate into the joint. Moderate (pooled observational series).
This complication profile is why progression waits on radiographs: premature loading risks tipping a borderline reduction into varus collapse or screw cut-out. Some surgeons even advocate early planned plate removal to avoid secondary screw penetration once the head shows AVN/collapse (Dimitriou et al., J Orthop, 2019) — a salvage strategy, not part of routine rehab, but it illustrates how mechanical and biological failure interact.
4. Who is offered ORIF at all — the operative-versus-non-operative debate (PROFHER and after)
The single most influential trial is PROFHER (Rangan et al., JAMA, 2015; 250 patients, 32 UK centres, displaced fractures involving the surgical neck): surgery showed no important difference in Oxford Shoulder Score versus sling-based non-operative care over 2 years, and was more expensive. The 5-year follow-up (Handoll/Keding et al., Bone Joint J, 2017) confirmed no significant difference in shoulder function or quality of life persisting to 5 years. A smaller RCT in displaced 3-part fractures in the elderly (Fjalestad et al., J Shoulder Elbow Surg, 2012) similarly found no functional advantage to internal fixation over non-operative care in that group, and a systematic review and meta-analysis (Beks et al., J Shoulder Elbow Surg, 2018) found no clear superiority of operative treatment across observational and randomised data combined. Strong (multiple RCTs + SR-MA).
The clinical upshot — and the reason this matters to a rehab page — is that ORIF is selectively indicated, typically in younger patients, in fractures where reduction and stable fixation are achievable and worthwhile, and where the alternative (non-operative care or arthroplasty) is judged less favourable. The decision is individualised; "difficulty in decision-making" for displaced fractures is itself documented as affecting outcomes (Okike et al., J Shoulder Elbow Surg, 2018). Patients should understand that being offered ORIF is a considered judgement, not an automatic consequence of the fracture.
5. Adjacent rehabilitation evidence (non-operative immobilisation duration)
Although it concerns non-operatively treated fractures, a relevant randomised controlled trial (Tanji et al., J Bone Joint Surg Am, 2021) compared 1 versus 3 weeks of immobilisation and supports the broad theme that earlier movement is at least as good as longer immobilisation for many proximal humerus fractures. It does not directly govern the post-ORIF protocol but reinforces the same direction-of-travel away from prolonged slings. Moderate (RCT, non-operative population).
Phased post-operative timeline (consistent with the synthesis page)
| Phase | Window | Sling | Shoulder motion | Strengthening | Governing rule |
|---|---|---|---|---|---|
| I — Protection & early passive motion | Weeks 0–6 | Full-time ~3 weeks, then weaned; off for exercises/hygiene; not in bed | Early active-assisted/active elevation permitted in a pain-free range from the outset (supine-start → upright); passive as needed; pendulums; elbow/wrist/hand active. ER kept to a gentle ~30–40° default; rotation cautious — defer active/resisted cuff work until tuberosities heal (surgeon-guided) | None at the shoulder (deltoid/periscapular isometrics as comfort allows) | Protect fixation + tuberosities; settle pain/swelling |
| II — Regaining active movement | Weeks 6–12 | Discarded by the 6-week review at the latest | Active-assisted → active in all planes (supine-start elevation); submaximal cuff/deltoid isometrics once healing confirmed | Light elbow/scapular work; no resisted cuff work until union (typically not before 8–12 weeks) | Radiographic healing at the ~6-week review gates active motion |
| III — Strengthening | ~Months 3–4½ | Off | Full active ROM in all planes, including behind-the-back | Graded bands → light free weights (~0.5–2 kg) for cuff, deltoid, scapula | Union confirmed; symptom-guided load progression |
| IV — Return to full activity | ~4½–6 months | Off | Full, with dynamic/overhead drills as relevant | Heavier resistance, compound + sport/work-specific | Return-to-task agreed with surgeon/physio, not the calendar |
The phase boundaries are individualised at Dr Hirpara's reviews on the basis of X-ray healing — this is the operative consequence of the "stability- and healing-governed, not calendar-governed" principle.
Key controversies / evidence quality
-
Early active versus delayed (protected) mobilisation after ORIF. A single RCT (Loew 2025) found unrestricted early active motion non-inferior to 4-week immobilisation at 24 months, and the broader literature leans toward shorter immobilisation. The protocol here aligns with that early-active-motion evidence: early active and active-assisted elevation in a pain-free range is permitted for stable fixation, rather than holding the shoulder passive-only for six weeks. Because there is still no consensus and no large confirmatory trial (protocols remain heterogeneous — Budharaju 2024), the protocol keeps one deliberate, evidence-aware caution: active/resisted rotation and cuff loading is keyed to radiographic tuberosity healing rather than released wholesale on day one. Moderate evidence, unsettled.
-
Operative versus non-operative treatment of displaced fractures. PROFHER (2015) and its 5-year follow-up (2017), plus an elderly-3-part RCT (Fjalestad 2012) and a meta-analysis (Beks 2018), found no clear functional benefit of surgery on average — which is why ORIF is selectively, not routinely, offered. The trials enrolled broad/older populations; the subgroup most likely to benefit from fixation (younger patients, good bone, reconstructable head-preserving fractures) is exactly where this operation is concentrated. Strong evidence overall; subgroup benefit remains debated.
-
The post-operative rehab protocol itself is consensus/expert. No high-level RCT defines the optimal phase structure, ROM limits or strengthening onset after ORIF. The timings here are drawn from published surgeon protocols and the systematic-review averages, individualised at review. Weak/consensus.
Evidence-strength flags (summary)
- STRONG (RCT / SR-MA): operative versus non-operative equivalence on average for displaced fractures (PROFHER 2-yr JAMA 2015 + 5-yr Bone Joint J 2017; Fjalestad 2012 RCT; Beks 2018 SR-MA).
- MODERATE (single RCT / pooled series): early active motion non-inferior to immobilisation after ORIF at 24 months (Loew 2025 RCT); 1-vs-3-week immobilisation non-operatively (Tanji 2021 RCT); locking-plate complication profile — screw perforation, varus collapse, AVN, etc. (pooled observational series); descriptive practice pattern of short sling + early passive ROM (Budharaju 2024 SR of 45 cohorts).
- WEAK / CONSENSUS: the specific phased rehabilitation timetable after ORIF (no defining rehab RCT; published surgeon protocols + systematic-review averages; progression individualised by radiographic healing).
Citations
RAG corpus (180,000+ Orthopaedic articles) — real DOIs
- Five-year follow-up results of the PROFHER trial comparing operative and non-operative treatment of adults with a displaced fracture of the proximal humerus. Bone Joint J. 2017. DOI: 10.1302/0301-620x.99b3.bjj-2016-1028
- Operative versus nonoperative treatment of proximal humeral fractures: a systematic review, meta-analysis, and comparison of observational studies and randomized controlled trials. J Shoulder Elbow Surg. 2018. DOI: 10.1016/j.jse.2018.03.009
- Internal fixation versus nonoperative treatment of displaced 3-part proximal humeral fractures in elderly patients: a randomized controlled trial. J Shoulder Elbow Surg. 2012. DOI: 10.1016/j.jse.2010.12.018
- One Versus 3-Week Immobilization Period for Nonoperatively Treated Proximal Humeral Fractures: a randomized controlled trial. J Bone Joint Surg Am. 2021. DOI: 10.2106/jbjs.20.02137
- Contemporary Management of Proximal Humeral Fractures. J Am Acad Orthop Surg. 2024. DOI: 10.5435/jaaos-d-24-01073
- The Use of Precontoured Humeral Locking Plates in the Management of Displaced Proximal Humerus Fracture. J Am Acad Orthop Surg. 2009. DOI: 10.5435/00124635-200909000-00005
- Use of locking plates in the treatment of proximal humerus fractures. J Shoulder Elbow Surg. 2010. DOI: 10.1016/j.jse.2010.01.001
- Functional results and unfavorable events after treatment of proximal humerus fractures using a new locking plate system. BMC Musculoskelet Disord. 2023. DOI: 10.1186/s12891-023-06176-5
- Fracture site augmentation with calcium phosphate cement reduces screw penetration after open reduction–internal fixation of proximal humeral fractures. J Shoulder Elbow Surg. 2012. DOI: 10.1016/j.jse.2011.09.017
- Difficulty in decision making in the treatment of displaced proximal humerus fractures: the effect of uncertainty on surgical outcomes. J Shoulder Elbow Surg. 2018. DOI: 10.1016/j.jse.2017.09.033
Literature (URLs)
- Loew M, et al. Postoperative treatment of proximal humerus fractures with an early active motion protocol: a prospective randomized controlled trial. J Orthop. 2025. https://www.sciencedirect.com/science/article/pii/S1058274625001867 (Constant 81.3 conventional vs 78.4 early-functional at 24 months; early active motion non-inferior)
- Budharaju A, Hones KM, Hao KA, et al. Rehabilitation protocols in proximal humerus fracture management: a systematic review. Shoulder Elbow. 2024;16(4):449–458. https://pmc.ncbi.nlm.nih.gov/articles/PMC11437559/ (45 cohorts; sling 3.1 wk, passive 0.9 wk, active 2.5 wk, strengthening 5.5 wk; early mobilisation may improve function)
- Rangan A, et al. (PROFHER). Surgical vs nonsurgical treatment of adults with displaced fractures of the proximal humerus: the PROFHER randomized clinical trial. JAMA. 2015;313(10):1037–1047. https://pubmed.ncbi.nlm.nih.gov/25756440/ (250 patients; no important difference in Oxford Shoulder Score at 2 years)
- Complications associated with locking plate of proximal humerus fractures (systematic review of complication rates). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC5858203/ (screw perforation ~9–12%, varus collapse ~6.8%, AVN ~4.6%)
- Avascular necrosis and posttraumatic arthritis after proximal humerus fracture internal fixation: evaluation and management. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC9889581/ (AVN reported range 0–15%)
- Late screw-related complications in locking plating of proximal humerus fractures: a systematic review. Injury. https://www.sciencedirect.com/science/article/abs/pii/S0020138319306989
- Dimitriou D, et al. Early locking plate removal following ORIF of proximal humeral fractures could prevent secondary implant-related complications. J Orthop. 2019;17:106–109. https://pmc.ncbi.nlm.nih.gov/articles/PMC6919395/
Published rehabilitation protocols (patient-guidance — basis for the phase structure)
- Massachusetts General Brigham Sports Medicine. Rehabilitation Protocol for Proximal Humeral Fracture Open Reduction Internal Fixation (ORIF). https://www.massgeneral.org/assets/MGH/pdf/orthopaedics/sports-medicine/physical-therapy/rehabilitation-protocol-for-proximal-humeral-fracture-with-ORIF.pdf
- LaPrade CM. Post-Surgical Physical Therapy Protocol: Proximal Humerus Fracture ORIF. Twin Cities Orthopedics. https://tcomn.com/wp-content/uploads/2024/08/CML_Proximal-Humerus-ORIF-PT_10-2024.pdf
- Coyner KJ. ORIF Proximal Humerus Fractures Protocol. UConn Musculoskeletal Institute. https://www.drcoyner.com/pdf/orif-proximal-humerus-fractures-protocol.pdf
- Jazrawi LM. Rehabilitation Protocol: Proximal Humerus Open Reduction & Internal Fixation (ORIF). NYU Langone Orthopedic Center. https://www.newyorkortho.com/pdf/proximal-humerus-fracture-orif-post-op-instructions-and-rehab.pdf
- South Bend Orthopaedics. ORIF Proximal Humerus Fracture Rehab Protocol. https://www.sbortho.com/wp-content/uploads/2023/09/br-pt-fracture-orif-proximal-humerus.pdf





