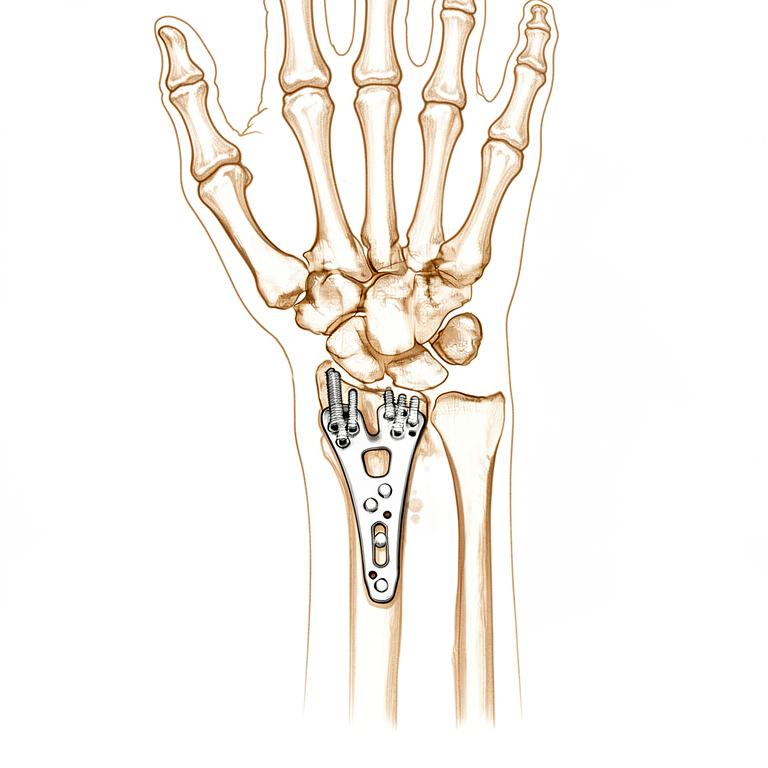
Nẹp cố định xương cẳng tay dưới
Patients › Wrist
Open reduction and volar plate fixation of the distal radius — operation, recovery, rehabilitation.
Lý do phẫu thuật này được đề xuất
Bác sĩ phẫu thuật của bạn đã đề xuất phương pháp nắn kín và cố định bên trong (open reduction and internal fixation), còn được gọi là ORIF, để sửa chữa xương cổ tay bị gãy bằng cách sử dụng tấm kim loại và vít. Phẫu thuật này thường được chỉ định cho người lớn có các loại gãy xương phức tạp, khi xương bị lệch vị trí hoặc vỡ thành nhiều mảnh. Mặc dù các phương pháp không phẫu thuật như bó bột thường được áp dụng trước tiên, phẫu thuật được khuyến nghị khi những phương pháp này không thể cung cấp đủ độ ổn định hoặc khả năng liền xương.
Mục tiêu chính của phẫu thuật này là khôi phục hình dạng bình thường của khớp cổ tay và giúp bạn cử động bàn tay sớm hơn. Bằng chứng cho thấy việc sử dụng tấm kim loại mang lại kết quả tốt nhất cho quá trình phục hồi sớm và duy trì so với các phương pháp khác. Nó cũng làm giảm đáng kể nguy cơ biến chứng liên quan đến việc xương không liền đúng cách.
Trước khi phẫu thuật
Vui lòng nhịn ăn trong sáu giờ trước ca phẫu thuật và ngừng các loại thuốc làm loãng máu theo chỉ định của bác sĩ phẫu thuật. Hãy sắp xếp để có người đưa bạn về nhà và mang theo danh sách tất cả các loại thuốc hiện tại bạn đang sử dụng. Bạn có thể cần chụp X-quang, và có thể cả MRI hoặc xét nghiệm máu, để kiểm tra sức khỏe xương và khớp trước khi thực hiện thủ thuật. Bác sĩ phẫu thuật sẽ thực hiện một ca mổ mở thông qua một vết rạch tiêu chuẩn để căn chỉnh lại xương và cố định nó bằng một tấm kim loại. Đôi khi, một camera nhỏ được sử dụng bên trong khớp để đảm bảo sự căn chỉnh là hoàn hảo. Hãy mặc quần áo thoải mái và đến nơi sẵn sàng cho buổi đánh giá gây mê.
Vào ngày phẫu thuật
Bạn sẽ đến bệnh viện và gặp bác sĩ phẫu thuật cùng bác sĩ gây mê. Phẫu thuật này được thực hiện dưới gây mê toàn thân. Bạn sẽ hoàn toàn bất tỉnh trong suốt quá trình phẫu thuật. Một số bệnh nhân cũng có thể được gây tê vùng (khối thần kinh) để giảm đau sau phẫu thuật; bác sĩ gây mê sẽ quyết định vào ngày phẫu thuật dựa trên tình trạng cá nhân của bạn.
Sau đó, bạn sẽ được đưa vào phòng mổ, nơi bác sĩ phẫu thuật sẽ rạch da để tiếp cận xương. Họ sử dụng một tấm kim loại và các vít để cố định các mảnh xương gãy vào vị trí. Sau phẫu thuật, bạn sẽ tỉnh dậy tại khu vực hồi sức, trong khi các y tá theo dõi và kiểm soát cơn đau của bạn.
Thủ thuật phẫu thuật bao gồm
Bác sĩ phẫu thuật của bạn sẽ thực hiện một vết rạch duy nhất qua cổ tay để tiếp cận xương bị gãy. Đây là phương pháp phẫu thuật mở, nghĩa là khu vực được phơi bày hoàn toàn thay vì sử dụng các camera nội soi nhỏ. Qua vết mổ này, bác sĩ phẫu thuật của bạn sẽ cẩn thận đưa các mảnh xương gãy trở lại vị trí chính xác.
Sau khi xương được căn chỉnh, bác sĩ phẫu thuật của bạn sẽ cố định xương bằng một tấm kim loại và các vít. Phương pháp này mang lại kết quả tốt nhất cho quá trình phục hồi sớm và bền vững, đồng thời giúp giảm thiểu các biến chứng trong quá trình lành xương. Tấm kim loại được đặt dọc theo cạnh của xương quay để giữ mọi thứ ổn định trong quá trình lành xương. Trong một số trường hợp, bác sĩ phẫu thuật của bạn có thể sử dụng một kỹ thuật vít đặc biệt với bất kỳ tấm khóa nào có các tùy chọn ở thân xương.
Sau khi xương được cố định, bác sĩ phẫu thuật của bạn sẽ khâu vết mổ lại. Bạn có thể cần một cuộc phẫu thuật nhỏ thứ hai sau này nếu thiết bị gây kích ứng, vì có 28% khả năng cần phải tháo thiết bị cho những bệnh nhân được phẫu thuật với tấm kim loại này. Việc vận động sớm bàn tay và cổ tay sau phẫu thuật được khuyến khích để giúp bạn sớm khôi phục chức năng hơn so với việc chờ đợi.
Sau phẫu thuật
Bạn sẽ tỉnh dậy tại khoa hồi sức, nơi cơn đau của bạn được kiểm soát bằng thuốc giảm đau thông thường. Cánh tay của bạn sẽ được đặt trong nẹp hoặc băng cố định, với băng gạc phủ lên vết mổ. Bác sĩ phẫu thuật của bạn đã thực hiện một vết mổ mở để cố định xương, đôi khi sử dụng một camera nhỏ để kiểm tra khớp. Bạn có thể bắt đầu cử động ngón tay và cổ tay sớm để hỗ trợ chức năng. Hầu hết bệnh nhân nằm viện một đêm sau phẫu thuật này, mặc dù một số có thể về nhà cùng ngày. Bạn cần có người ở bên cạnh trong 24 giờ đầu tiên.
Phục hồi
Bạn có thể sẽ cảm thấy đau và sưng ở cổ tay và bàn tay trong vài ngày đầu. Đây là điều bình thường khi cơ thể bạn đang hồi phục sau phẫu thuật. Bác sĩ phẫu thuật của bạn có thể sử dụng một tấm kim và vít để cố định xương tại chỗ thông qua một vết rạch nhỏ ở cổ tay. Bạn cũng có thể được đeo nẹp hoặc bột bó để bảo vệ vùng tổn thương trong thời gian nghỉ ngơi.
Vận động sớm là yếu tố then chốt để giúp bàn tay của bạn trở lại bình thường. Chuyên viên vật lý trị liệu sẽ hướng dẫn bạn thực hiện các bài tập nhẹ nhàng để giảm cứng khớp. Bạn sẽ đeo nạng hoặc nẹp khi di chuyển, nhưng bạn nên bắt đầu cử động các ngón tay và khuỷu tay ngay khi có thể. Những cử động nhỏ này giúp bàn tay của bạn cảm thấy tốt hơn sớm hơn nhiều so với việc chờ đợi quá lâu.
Khi tình trạng sưng giảm bớt, bạn sẽ nhận thấy khả năng nắm và các hoạt động hàng ngày trở nên dễ dàng hơn. Bạn có thể quay trở lại các hoạt động nhẹ nhàng tại nhà sau khi bác sĩ phẫu thuật cho phép. Thời gian phục hồi của bạn có thể khác với người khác, vì vậy hãy tuân thủ các lời khuyên cụ thể từ bác sĩ phẫu thuật và nhóm vật lý trị liệu. Họ sẽ giúp bạn xác định chính xác thời điểm an toàn để tăng mức độ hoạt động.
Những biến chứng có thể xảy ra
Hầu hết bệnh nhân đều hồi phục tốt, nhưng đôi khi có thể xảy ra các vấn đề. Bác sĩ phẫu thuật và đội ngũ y tế sẽ theo dõi bạn chặt chẽ để phát hiện sớm bất kỳ vấn đề nào.
Đôi khi, các dụng cụ kim loại được sử dụng để cố định xương của bạn gây khó chịu hoặc kích ứng. Nếu bạn cảm thấy đau hoặc áp lực ở vị trí đặt tấm kim loại, bạn có thể cần một thủ thuật nhỏ thứ hai để loại bỏ nó. Điều này xảy ra ở khoảng một trên bốn bệnh nhân.
Bạn có thể nhận thấy cổ tay của mình không cử động mượt mà như mong đợi. Việc vận động sớm giúp bàn tay của bạn hoạt động tốt hơn so với việc chờ đợi quá lâu. Nếu cổ tay của bạn cảm thấy cứng hoặc yếu, hãy báo ngay cho bác sĩ phẫu thuật để họ hướng dẫn liệu pháp phục hồi chức năng.
Trong một số trường hợp, sự căn chỉnh của xương có thể bị lệch nhẹ theo thời gian. Điều này có thể xảy ra nếu các vít không được đặt đủ sâu vào trong xương. Nếu bạn nghe thấy tiếng kêu lách cách mới hoặc nhận thấy bàn tay của mình trông khác đi, hãy đề cập điều này trong lần kiểm tra tiếp theo.
Nhìn chung, các biến chứng nghiêm trọng là hiếm. Hầu hết mọi người sau khi thực hiện phẫu thuật này đều hồi phục tốt nhờ vận động sớm và theo dõi cẩn thận. Bảng biến chứng trên trang này liệt kê các tỷ lệ điển hình nếu bạn muốn biết chi tiết.
Khi nào cần gọi cho chúng tôi
Gọi cho chúng tôi nếu bạn bị sốt, đỏ tăng dần hoặc có dịch chảy ra từ vết mổ. Đến khoa cấp cứu nếu bạn cảm thấy đau dữ dội đột ngột, nhận thấy bắp chân của bạn sưng lên hoặc gặp khó khăn khi thở. Gọi ngay lập tức nếu bạn mất cảm giác ở các ngón tay hoặc không thể cử động bàn tay. Những dấu hiệu này cần được đánh giá khẩn cấp để bảo vệ quá trình hồi phục của bạn.
Evidence & references
Overview
- Early mobilization for patients with distal radius fractures treated with ORIF may have a beneficial effect on function at earlier stages compared to late mobilization [1].
- Mean differences in DASH scores at 6 weeks for early mobilization in distal radius fractures treated with ORIF surpass the minimal clinically important difference [1].
- Substantial variations in surgical direct costs for distal radius ORIF exist [2].
- Implant choice is the predominant driver of cost variation for distal radius ORIF [2].
- The LOS length can be calculated for the Lift-Off Screw technique in a distal radius fracture model [3].
- The Lift-Off Screw technique can potentially be used with any distal radius periarticular locking plate with locking options in the shaft [3].
- Open reduction and internal fixation with a plate offers the best results for adult patients with a distal radius fracture in terms of early and sustained functional recovery [5].
- Open reduction and internal fixation with a plate offers the best results for adult patients with a distal radius fracture in terms of reduction in fracture healing complications [5].
- Radial column plating of the distal radius is a safe treatment modality [6].
- Radial column plating of the distal radius is a valuable adjunct in the setting of complex distal radius fractures [6].
- There is a 28% chance that hardware removal may be required for patients undergoing radial column plating of the distal radius [6].
- Placing the distal row of screws greater than 3mm from subchondral bone in comminuted intra-articular distal radius fractures was associated with increased odds of worsening ulnar variance [8].
- The treatment of displaced intra-articular distal radius fractures with a dorsally versus a volarly placed interlocking plate system demonstrated similar clinical results [9].
Anatomy & Pathophysiology
- Distal radius fractures are the most common fractures of the upper extremity in the United States, occurring in over 300,000 cases per year [27].
- Distal radius fractures exhibit a bimodal distribution with young patients sustaining high-energy trauma and elderly patients sustaining low-energy falls [27].
- Distal radius fractures are the most common upper extremity osteoporotic fracture in elderly patients [27].
- The distal radius articular surface is biconcave with distinct scaphoid and lunate facets [27].
- The distal radioulnar joint (DRUJ) is the articulation between the radius and ulna at the sigmoid notch [27].
- Lister tubercle is a small dorsal prominence on the distal radius that serves as a landmark for the dorsal approach to the wrist [27].
- Lister tubercle is a cause of attritional rupture of the extensor pollicis longus (EPL) after a distal radius fracture [27].
- The metaphysis of the distal radius has a thin cortex and is vulnerable to bending forces [27].
- The brachioradialis insertion on the radial styloid acts as a deforming force in distal radius fractures [27].
- In a normal wrist, the distal radius bears 80% of the axial load in neutral ulnar variance [27].
- The carpus encompasses two rows of eight bones that serve as a bridge between the forearm and the hand [16].
- The proximal carpal row from radial to ulnar includes the scaphoid, lunate, and triquetrum [16].
- The proximal carpal row is referred to as the key intercalated segment between the forearm and the distal row of the carpus [16].
- There are no direct tendon attachments to the proximal carpal row [16].
- The movement of the proximal carpal row results from the shape of the bones, their interaction with other bones, and ligament attachments [16].
- The pisiform bone is a sesamoid bone enclosed within the sheath of the flexor carpi ulnaris tendon and should not theoretically be considered within the proximal carpal row [16].
- The distal carpal row from radial to ulnar includes the trapezium, trapezoid, capitate, and hamate [16].
- The distal carpal row articulates with the proximal carpal row and distally with the five metacarpals of the hand [16].
- The trapezium articulates with the first metacarpal, the trapezoid with the second, the capitate with the third, and the hamate with the fourth and fifth metacarpals [16].
- The capitate and trapezoid are tightly connected to the metacarpals [16].
- There is 30 to 40 degrees of flexion–extension and rotation at the metacarpotrapezial joint [16].
- Motion at the distal carpal row is controlled by the extrinsic wrist flexors and extensors [16].
- The ligaments of the wrist are predominantly contained within the joint capsule [16].
- The inherent stability of the carpal rows is predominantly due to the support of extrinsic and intrinsic ligaments that reinforce the capsule of the carpus [16].
- Apart from the scaphocapitate ligament, carpal ligaments are not described consistently across anatomical studies [16].
- The extrinsic palmar radiocarpal ligaments include the transverse carpal, radioscaphocapitate (RSC), radioscapholunate (RSL), radial collateral, long radiolunate (RLT), and short radiolunate ligaments [23].
- The extrinsic ulnocarpal ligaments include the ulnotriquetral (dorsal and palmar), ulnolunate, and ulnocapitate ligaments [23].
- The strong oblique extrinsic palmar radial ligaments prevent the carpus from translating medially on the angulated slope of the distal radius through two V-shaped ligamentous bands [23].
- One V-shaped band is proximal (long radiolunate, radioscapholunate, ulnolunate, ulnotriquetral) and connects the forearm to the proximal carpal row [23].
- One V-shaped band is distal (radioscaphocapitate, ulnocapitate) and connects the forearm to the distal carpal row [23].
- Between the radial and ulnar palmar ligaments there is a V-shaped interligamentous sulcus over the capitolunate articulation known as the space of Poirier [23].
- Maximal space in the space of Poirier is seen when the wrist is dorsiflexed [23].
- The space of Poirier almost disappears in palmar flexion [23].
- The lunate displaces into the carpal canal through the space of Poirier during dorsal dislocations [23].
- The arcuate ligament is found in the central third of the palmar joint capsule and is thought to be formed from the interdigitation of transverse fibers of the radioscaphocapitate, ulnocapitate, triquetrocapitate, and volar scaphotriquetral ligaments [23].
- The arcuate ligament forms a support sling for the midcarpal region, in particular the head of the capitate [23].
- The extrinsic dorsal carpal ligaments include the dorsal radiocarpal (DRC) ligament and the dorsal intercarpal ligament [23].
- The dorsal intercarpal ligament forms a V-shaped configuration [23].
- The ulnodorsal capsule of the wrist is reinforced by the ulnolunate and ulnotriquetral ligaments and the floors of the fifth and sixth extensor compartments [23].
- Some studies suggest an essential role of the dorsal carpal ligaments in scapholunate stability [23].
- The intrinsic ligaments connect the individual carpal bones to one another [23].
- The intrinsic ligaments are intra-articular short fibers that connect and hold the carpal bones of both the proximal or distal rows to each other [23].
- There is a contiguous merging of the interosseous ligaments with the joint articular cartilage [23].
- The intrinsic ligaments include the palmar midcarpal ligaments (scaphotrapeziotrapezoid, scaphocapitate, triquetrocapiate, triquetrohamate) [23].
- The intrinsic ligaments include the proximal interosseous ligaments (scapholunate, lunotriquetral) [23].
- The intrinsic ligaments include the distal interosseous ligaments (trapeziotrapezoid, trapeziocapitate, capitohamate) [23].
- The pisotriquetral ligament bridges the pisotriquetral joint [23].
- The pisohamate ligament is an extension of the flexor carpi ulnaris [23].
- On the radial side of the wrist, the V-shaped scaphotrapezium–trapezoid ligament provides stability to the scaphoid–trapezium–trapezoid articulation as well as the scaphoid itself [23].
- Recent studies suggest the existence of two distinct ligaments on the radial side: the scaphotrapezoid and scaphotrapezium ligaments [23].
- The scaphocapitate is a large robust ligament that provides midcarpal stability [23].
- The scaphoid bone is located in the proximal carpal row on the radial aspect of the wrist [21].
- The scaphoid is a small, irregular S-shaped tubular bone [21].
- The scaphoid lies entirely within the wrist joint and is located at a 45-degree plane to the longitudinal and horizontal axis of the wrist [21].
- The scaphoid articulates with the trapezium/trapezoid (distal surface), radius (proximal/lateral surface), capitate (medial surface), and lunate (medial surface) [21].
- The proximal articular surface of the scaphoid is convex and articulates with the radius [21].
- The capitate head articulates with a sulcus on the scaphoid located across the radial articular surface [21].
- The scaphoid gently pronates and flexes distally such that the distal pole sits ulnarly angulated relative to the proximal pole [21].
- At the distal articular surface, two distinct articular facets for the trapezium and trapezoid are present forming the STT joint [21].
- Over 80% of the scaphoid surface is covered with articular cartilage [21].
- The scaphoid has a reduced capacity for periosteal healing and an increased tendency for delayed union and nonunion [21].
- The scaphoid is ridged across its nonarticular dorsoradial surface, along which the critical dorsal ridge vessels traverse [21].
- The ridge is the insertion point for both the dorsal component of the scapholunate and intercarpal ligaments [21].
- The ligamentous attachments of the scaphoid are predominantly found on the nonarticular dorsoradial surface [21].
- The radioscapocapitate ligament does not attach to the bone itself but crosses the waist, acting as a sling across it allowing it to rotate [21].
- There are no tendon attachments to the scaphoid [21].
- The scaphoid acts as a midcarpal joint "bridge" linking and synchronizing the motions of the proximal and distal carpal rows [21].
- Motion of the scaphoid includes rotation proximally and gliding distally [21].
- The potential for nonunion of the scaphoid is often ascribed to the meagre, largely retrograde blood supply [21].
- The blood supply to the scaphoid is provided by two vascular pedicles originating from the scaphoid branches of the radial artery [21].
- The dorsal branch enters via the small foramina along the spiral groove and dorsal ridge of the scaphoid and supplies 70% to 80% of the scaphoid proximally, including the proximal pole [21].
- The volar branch enters via the scaphoid tubercle and supplies the remaining 20% to 30% of distal scaphoid [21].
- The waist of the scaphoid has been shown to have minimal or no perforating vasculature [21].
- No vessels perforate the proximal dorsal cartilaginous area or through the scapholunate ligament [21].
- Proximal fractures are inexorably associated with at least temporary disruption of the interosseous blood supply to the proximal pole [21].
- The metacarpals form a unique cascade similar to that of a Roman arch [20].
- The index and small fingers form the borders of the metacarpal cascade while the middle finger forms the keystone [20].
- The metacarpals are inherently stable secondary to the origins of the intrinsic muscles of the hand as well as the stout attachments of the deep transverse intermetacarpal ligaments [20].
- The bony architecture of the metacarpal is made up of a distal and proximal metaphysis [20].
- The metaphyseal portion of the metacarpal has a thinner cortex and does not provide rigid purchase for cortical fixation [20].
- The diaphyseal portion of the metacarpal provides better purchase with its tubular structure and thick cortices [20].
- The middle and ring fingers have the most inherent stability secondary to their central location [20].
- The border digits are more prone to shortening, rotation, and angulation [20].
- The CMC joints increase in stability and decrease in dorsal-volar mobility when moving from the small to index finger metacarpal [20].
- The small and ring fingers are far more tolerant to deformity than are the index and middle finger metacarpals [20].
- In the sagittal plane, the metacarpal head has a cam-shaped articular surface with a larger volar-dorsal diameter than a proximal-distal diameter [20].
- In the transverse plane, the metacarpal head resembles a trapezoid [20].
- The collateral ligaments of the metacarpal head attach on the dorsal aspect of the metacarpal head within the recess and are thus elongated in flexion [20].
- The combination of the trapezoidal shape of the head, origin and insertion of the collateral ligaments, and cam-shaped morphology contribute to inherent stability during MCP flexion [20].
- The metacarpals of the hand and thumb are subcutaneous in position and are thus susceptible to penetrating and crush injuries [20].
- The metacarpals have a curvature to their diaphyseal segment and often flex during the making of a fist [20].
- The metacarpal necks are susceptible to fracture during punching [20].
- The fifth metacarpal has the most anterior–posterior arc at the CMC joint [20].
- Metacarpal fractures are third in frequency only to phalangeal fractures and distal radius fractures in the upper limb [17].
- Approximately 70% of metacarpal fractures occur during the second and fifth decades of life [17].
- The vast majority of metacarpal fractures are inherently stable and can be treated via closed means with early range of motion [17].
- The flexor carpi radialis (FCR) approach provides excellent exposure for volar plating [26].
- Incising the FCR sheath on its radial aspect may help to avoid injury to the palmar cutaneous branch of the median nerve [26].
- A brachioradialis tenotomy removes a deforming force during the FCR approach [26].
- Repair of the pronator quadratus did not result in better outcomes at 12 months in a randomized trial of 72 patients [26].
- The extended FCR approach aims to facilitate adequate distal exposure including the volar ulnar corner [26].
- By releasing the superficial and deep leaves of the FCR sheath to the level of the trapezium, the carpal tunnel contents are more easily retracted ulnarly [26].
- Pronation of the ulnar shaft through the fracture exposes the dorsal metaphysis in subacute fractures [26].
- Biasing the skin incision more midline allows development of the interval between the digital flexors and ulnar neurovascular bundle [26].
- Retracting the carpal tunnel contents radially provides excellent visualization of the lunate facet fragment [26].
- The approach for the volar ulnar facet fragment is extensile with an open carpal tunnel release [26].
- A radial column approach requires protection of the superficial branch of the radial nerve [26].
- The deep interval for a radial column approach is through the first dorsal compartment or the interval between the first and second compartments [26].
- The dorsal approach is the traditional approach for plating distal radius fractures [26].
- Enthusiasm for dorsal plating waned as a result of extensor tendon complications [26].
- A dorsal approach may be necessary to reduce and stabilize the dorsal ulnar facet fragment [26].
- Elevation of the fourth dorsal compartment on its ulnar aspect exposes the dorsal ulnar corner [26].
- Unlike the volar approach, the dorsal approach affords the option of visualizing the articular surface through a dorsal capsulotomy [26].
- The most common tendon to rupture following application of a volar plate is the flexor pollicis longus [34].
- Rupture of the flexor pollicis longus is due to volar extension of the plate beyond the so-called watershed line [34].
- Dorsal tendons such as the extensor pollicis longus and extensor digitorum communis can fray and rupture from prominent screw tips following volar insertion [34].
- Dorsal plates or constructs are now preferred for dorsal shearing fractures and complex articular fractures [34].
- Distraction (or bridge) plate fixation is increasingly utilized for complex articular fracture, those with complex metaphyseal or diaphyseal fragmentation in particular [34].
- Application of the bridge/distraction plate should not be a substitute for accurate ORIF [34].
- Fractures of the radial styloid may be associated with SL ligament injuries because the intra-articular fracture line extends into the joint at that level [34].
- In the setting of isolated radial styloid fractures, intercarpal ligament injuries must be suspected [34].
- Intra-articular displacement (or diastasis) greater than 2 mm is an indication for surgery for fractures of the radial styloid [34].
- Compression screw fixation with partially threaded 3.5- or 4.0-mm cancellous screws can effectively compress radial styloid fragments and maintain the reduction [34].
- Alternative fixation options for radial styloid fractures include K-wires and fragment-specific pin plate and screw fixation [34].
- The distal radioulnar joint is assessed following stabilization of the radius [34].
- Slightly greater laxity than the opposite uninjured wrist is to be expected after distal radius fracture treatment [34].
- Only frank dislocation with forearm rotation merits surgery to stabilize the distal radioulnar joint [34].
- The presence of a displaced fracture at the base of the ulnar styloid is not in itself an indication for surgical fixation [34].
- Clinical stability of the distal radioulnar joint must be elucidated and compared with
Classification
- Early mobilization for patients with distal radius fractures treated with ORIF may have a beneficial effect on function at earlier stages compared to late mobilization [1].
- Mean differences in DASH scores at 6 weeks for early mobilization in distal radius fractures treated with ORIF surpass the minimal clinically important difference [1].
- Substantial variations in surgical direct costs for distal radius ORIF exist [2].
- Implant choice is the predominant driver of cost variation for distal radius ORIF [2].
- The LOS length can be calculated for the lift-off screw technique in a distal radius fracture model [3].
- The lift-off screw technique can potentially be used with any distal radius periarticular locking plate with locking options in the shaft [3].
- Open reduction and internal fixation with a plate offers the best results for adult patients with a distal radius fracture in terms of early and sustained functional recovery [5].
- Open reduction and internal fixation with a plate offers the best results for adult patients with a distal radius fracture in terms of a reduction in fracture healing complications [5].
- Radial column plating of the distal radius is a safe treatment modality [6].
- Radial column plating of the distal radius is a valuable adjunct in the setting of complex distal radius fractures [6].
- There is a 28% chance that hardware removal may be required for patients undergoing radial column plating of the distal radius [6].
- Placing the distal row of screws greater than 3mm from subchondral bone in comminuted intra-articular distal radius fractures was associated with increased odds of worsening ulnar variance [8].
- The treatment of displaced intra-articular distal radius fractures with a dorsally versus a volarly placed interlocking plate system demonstrated similar clinical results [9].
Clinical Presentation
- Early mobilization for patients with distal radius fractures treated with ORIF may have a beneficial effect on function at earlier stages compared to late mobilization [1].
- Mean differences in DASH scores at 6 weeks for early mobilization in distal radius fractures treated with ORIF surpass the minimal clinically important difference [1].
- Substantial variations in surgical direct costs for distal radius ORIF exist, with implant choice being the predominant driver [2].
- Radial column plating of the distal radius is a safe treatment modality and a valuable adjunct in the setting of complex distal radius fractures [6].
- Patients undergoing radial column plating of the distal radius should be counseled that there is a 28% chance that hardware removal may be required [6].
- Placing the distal row of screws greater than 3mm from subchondral bone in comminuted intra-articular distal radius fractures was associated with increased odds of worsening ulnar variance [8].
- Treatment of displaced intra-articular distal radius fractures with a dorsally versus a volarly placed interlocking plate system demonstrated similar clinical results [9].
- An isolated radial shaft fracture is uncommon in adults because the forearm functions as a ring [35].
- Fractures within 7.5 cm of the radiocarpal joint are more likely to represent a Galeazzi fracture (radial shaft fracture with associated distal radioulnar joint injury) [35].
- Galeazzi fractures require surgical fixation with rare exceptions [35].
- Examination may reveal a prominent ulnar head in cases of dorsal distal radioulnar joint subluxation or dislocation [35].
- Radiographic parameters associated with injury to the distal radioulnar joint include fracture of the base of the ulnar styloid [35].
- Radiographic parameters associated with injury to the distal radioulnar joint include widening of the distal radioulnar joint on the AP wrist radiograph [35].
- Radiographic parameters associated with injury to the distal radioulnar joint include dislocation of the ulna relative to the radius on a true lateral wrist radiograph [35].
- Radiographic parameters associated with injury to the distal radioulnar joint include more than 5 mm of shortening of the radius relative to the ulna (ulnar positive variance) when compared with the contralateral wrist [35].
- Radial shaft fracture line obliquity greater than 30° is a statistically significant predictor of distal radioulnar joint instability [35].
- Closed management of displaced forearm axis fractures in adults results in poor outcomes [35].
- Surgery is indicated for all Galeazzi fractures to restore the structural integrity of the forearm ring [35].
- Complications following management of Galeazzi fractures of the radius include nonunion [35].
- Complications following management of Galeazzi fractures of the radius include malunion with limited forearm rotation [35].
- Complications following management of Galeazzi fractures of the radius include nerve or vessel injury [35].
- Complications following management of Galeazzi fractures of the radius include infection [35].
- Complications following management of Galeazzi fractures of the radius include complex regional pain syndrome [35].
- Complications following management of Galeazzi fractures of the radius include persistent distal radioulnar joint instability [35].
Investigations
- Early mobilization for distal radius fractures treated with ORIF may have a beneficial effect on function at earlier stages compared to late mobilization, with mean differences in DASH scores at 6 weeks surpassing the minimal clinically important difference [1].
- Substantial variations in surgical direct costs for distal radius ORIF exist, with implant choice being the predominant driver [2].
- The length of stay (LOS) can be calculated for a distal radius fracture model using the Lift-Off Screw technique, which can potentially be used with any distal radius periarticular locking plate with locking options in the shaft [3].
- Open reduction and internal fixation with a plate offers the best results for adult patients with a distal radius fracture in terms of early and sustained functional recovery and a reduction in fracture healing complications [5].
- Radial column plating of the distal radius is a safe treatment modality, but patients should be counseled that there is a 28% chance that hardware removal may be required [6].
- Placing the distal row of screws greater than 3mm from subchondral bone in comminuted intra-articular distal radius fractures was associated with increased odds of worsening ulnar variance [8].
- Treatment of displaced intra-articular distal radius fractures with a dorsally versus a volarly placed interlocking plate system demonstrated similar clinical results [9].
- An understanding of the anatomy and kinematics of the eight carpal bones is essential for the diagnosis and management of carpal injuries [16].
- The proximal carpal row includes the scaphoid, lunate, and triquetrum, serving as a key intercalated segment between the forearm and the distal row of the carpus [16].
- The distal carpal row includes the trapezium, trapezoid, capitate, and hamate, articulating with the proximal carpal row and distally with the five metacarpals [16].
- The inherent stability of the carpal rows is predominantly due to the support of extrinsic and intrinsic ligaments that reinforce the capsule of the carpus [16].
- Apart from the scaphocapitate ligament, carpal ligaments are not described consistently across anatomical studies [16].
- The incidence of metacarpal fractures is third in frequency only to phalangeal fractures and distal radius fractures in the upper limb [17].
- Approximately 70% of metacarpal fractures occur during the second and fifth decades of life [17].
- The vast majority of metacarpal fractures are inherently stable and can be treated via closed means with early range of motion [17].
- Assessment of metacarpal fractures requires evaluation of skin integrity, neurovascular status, ligamentous evaluation, and tendon function [17].
- Malrotation must be tested in metacarpal fracture assessment, with particular attention toward the border digits [17].
- Initial X-rays for suspected scaphoid fractures should include posteroanterior (PA) with wrist in ulnar deviation, lateral, semi-pronated oblique, and semi-supinated oblique views [24].
- An anteroposterior (AP) view with the fist clenched can be added if there is a suspicion of a scapholunate injury [24].
- In a normal lateral X-ray, the axes of the radius, lunate, capitate, and third metacarpal are co-linear [24].
- In a normal lateral X-ray, the scaphoid projects at an angle of about 45 degrees to the line of the radius [24].
- Dorsal intercalated segmental instability (DISI) is characterized by the lunate tilting dorsally and the scaphoid tilting somewhat volarwards [24].
- Volar intercalated segmental instability (VISI) is characterized by the lunate and scaphoid tilting somewhat volarwards [24].
- Radiocarpal instability in the acute phase presents with wrist swelling, deformity, and pain aggravated by wrist motion [25].
- Dorsal wrist swelling and tenderness are most noticeable at the radiocarpal level in acute radiocarpal instability [25].
- In patients with ulnar translation of the carpus, the radiographic appearance often shows the lunate positioned just distal to the ulna and a large space between the radial styloid and the scaphoid [25].
- CT may be required to better define associated bony injuries in radiocarpal instability [25].
- MRI can be used to determine the extent of ligamentous disruption in radiocarpal instability [25].
- Scaphoid fractures account for almost 75% of all carpal fractures [30].
- The usual mechanism for scaphoid fractures is forced hyperextension of the wrist [30].
- Scaphoid fractures occur in three anatomical locations: distal tubercle, waist, and proximal pole [30].
- The blood supply of the scaphoid arises from the dorsal distal pole, meaning the proximal pole has a poor blood supply [30].
- Precisely localized tenderness in the anatomical snuffbox is an important diagnostic sign for scaphoid fracture [30].
- Examination for scaphoid fracture should include pressure backwards over the scaphoid tubercle, palpation over the proximal pole, and telescoping of the thumb base [30].
- X-rays for suspected scaphoid fractures should include AP, lateral, and two oblique views [30].
- A CT scan is more sensitive for diagnosing a scaphoid fracture than X-rays [30].
- MRI is the definitive way to confirm or exclude a diagnosis of scaphoid fracture if the technique is available [30].
- If X-rays are normal but clinical features are suggestive of a scaphoid fracture, the patient should be immobilized and either re-X-rayed in 2 weeks or undergo an MRI scan [30].
- Secondary imaging modalities are predominantly used in the assessment of scaphoid fractures and the diagnosis of intercarpal ligament injury and any associated instability [31].
- Ultrasound scanning (USS) is used for suspected carpal fractures and ligament injuries [31].
- CT (2D/3D) is used for suspected carpal fractures, fracture displacement, malunion, nonunion, and bone loss [31].
- Dynamic CT is used by some for ligament injuries [31].
- Bone scintigraphy is used for suspected carpal fractures and avulsion injuries [31].
- Arthrography ± videofluoroscopy is used for ligament injuries [31].
- MRI is useful in detecting suspected fractures and avascular necrosis (AVN) of the carpus [31].
- Wrist arthroscopy can be used as an aid to the diagnosis of ligament injuries and fracture displacement [31].
- The lateral intrascaphoid angle is created by lines drawn perpendicular to the proximal and distal articular surfaces/poles of the scaphoid in a sagittal view [31].
- The normal lateral intrascaphoid angle is 30 degrees ±5 degrees [31].
- An angle greater than 35 degrees is used as a cut-off for scaphoid displacement [31].
- The AP intrascaphoid angle is created by lines drawn perpendicular to the proximal and distal articular surfaces in coronal views [31].
- The normal AP intrascaphoid angle is 40 degrees ± 5 degrees [31].
- The dorsal cortical angle is created by tangential lines drawn along the dorsal cortices of the proximal and distal scaphoid fragments in a sagittal view [31].
- The normal dorsal cortical angle is 140 degrees, with abnormal values greater than 160 degrees [31].
- The scaphoid height-to-length ratio is the ratio of the lines measuring the height and length of the scaphoid in a sagittal view [31].
- The normal scaphoid height-to-length ratio is 0.60, with abnormal values greater than 0.65 [31].
- Live/video fluoroscopic evaluation of the wrist can provide diagnostic clarity for dynamic instability with sensitivities reported between 86% and 95% [31].
- Sensitivities for live/video fluoroscopic evaluation are reported between 86% and 95%, with similar specificity between 80% and 97% for diagnosing scapholunate ligament injury [31].
- Ultrasound scanning provides an additional tool for the detection of carpal ligament injuries [31].
- Standard scaphoid radiographic views detect most carpal injuries [31].
- The DISI pattern is most commonly associated with displaced scaphoid fractures and scapholunate dissociation (SLD) [31].
- Perilunate dislocations can be missed on standard imaging [31].
- Assessment of Gilula's lines can aid in the diagnosis of perilunate dislocations [31].
- CT is useful in the diagnosis of suspected carpal fractures and assessment of union [31].
- MRI is useful in detecting suspected fractures and AVN of the carpus [31].
- Wrist arthroscopy can be used as an aid to the diagnosis of ligament injuries and fracture displacement [31].
- A cortical ring sign with the wrist in flexion, pronation, and ulnar deviation can help localize the ulnar aspect of the proximal pole of the scaphoid [32].
- A stab incision or mini-open incision can be performed to avoid injury to the soft tissue during percutaneous scaphoid fixation [32].
- The wire is advanced antegrade along the central axis of the scaphoid and then pulled distally from the palmar side until the proximal guidewire clears the radiocarpal joint [32].
- The wire is advanced retrograde until it exits the skin dorsally for percutaneous scaphoid fixation [32].
- Several millimeters should be subtracted from the measured screw length to avoid prominence at either end during scaphoid fixation [32].
- Biomechanical studies support the view that larger screws are stronger [32].
- Cannulated screws have been shown to improve central placement of the screw when compared with the Herbert screw [32].
- High-quality images are required for scaphoid fracture detection, and if initial X-rays are normal, the wrist should be treated and immobilized [24].
- 10–15% of scaphoid fractures are not visible on initial X-rays [24].
- Early MRI reduces uncertainty and streamlines care for suspected scaphoid fractures [24].
- If MRI is not available, repeated X-rays are needed 2 weeks later for suspected scaphoid fractures [24].
- If there is still doubt after a further 2 weeks, X-ray again for suspected scaphoid fractures [24].
- Unusual gaps between the scaphoid and the lunate suggest disruption of ligaments [24].
- With traumatic instability, the linked carpal segments collapse like the buckled carriages of a derailed train [24].
- In chronic causes for ulnar translation, rheumatoid arthritis and developmental deformities (e.g., Madelung deformity) are included [25].
- A decrease in the ulnocarpal index may provide the only clue to diagnosis in subtle ulnar shift cases [25].
- Scaphoid fractures are rare in children and in the elderly [30].
- Some scaphoid fractures, especially distal oblique and waist fractures, are unstable, which predisposes to non-union or malunion [30].
- If any of the clinical signs (snuffbox tenderness, pressure over tubercle, palpation of proximal pole, telescoping) are positive, the suspicion for a scaphoid fracture should be high [30].
- The crack in a scaphoid fracture is usually transverse through the narrowest part of the bone (the waist), but it may be more proximal or more distal [30].
- One must always look for signs of associated carpal displacement when evaluating scaphoid fractures [30].
- A CT scan is useful for showing the fracture configuration of a scaphoid fracture [30].
- The wrist should be held dorsiflexed and the thumb forwards in the 'glass-holding' position (the so-called scaphoid plaster) for suspected scaphoid fractures [30].
- The cast for suspected scaphoid fractures extends from the upper forearm to just short of the metacarpophalangeal joints of the fingers, but incorporates the proximal phalanx of the thumb [30].
- At least four X-rays should be taken of possible scaphoid fractures [30].
- Even if X-rays are normal initially, if there is any doubt, the patient should be put in plaster and either re-X-rayed in 2 weeks or an MRI scan should be obtained [30].
- The length of the screw for scaphoid fixation should be measured carefully, and several millimeters subtracted from the measured length to avoid prominence at either end [32].
- Predrilling is used depending on the type of screw during scaphoid fixation [32].
- If there is resistance during drilling for scaphoid fixation, it may indicate a bend in the wire that will lead to drill or wire breakage [32].
- Even if the screw is self-drilling, there is a risk of distraction of the fracture during scaphoid fixation [32].
- If distraction occurs during scaphoid fixation, the screw is removed, and the track drilled [32].
- If there is a bend in the wire during scaphoid fixation, the wire can usually be further advanced so that the drill passes over a nonbent part of the wire [32].
- After drilling for scaphoid fixation, the screw is advanced under image intensification [32].
- It is important to judge the screw length prior to fully seating the screw during scaphoid fixation [32].
- Central positioning of the screw without joint penetration at the radiocarpal joint or prominence at the scaphotrapezial joint should be confirmed with AP, lateral, supinated, and pronated views of the wrist after scaphoid fixation [32].
- There are a number of screws available which vary in size and pitch variation and can be partially, fully, or tip threaded [32].
- Some screws have ancillary techniques for achieving compression, such as special screwdrivers or mobile parts of the screw [32].
- A high index of suspicion is critical for scaphoid injuries as they can be missed in up to 25% of cases [31].
- Additional cost-effective tools to help in the diagnosis of scaphoid injuries can be performed with live/video fluoroscopic evaluation of the wrist [31].
- Few comparative studies exist regarding the utility of ultrasound scanning for carpal ligament injuries [31].
- The technique of ultrasound scanning for carpal ligament injuries is operator dependent [31].
- Ultrasound scanning has yet to be universally adopted for carpal ligament injuries because of operator dependence [31].
- Standard scaphoid radiographic views detect most carpal injuries [31].
- The DISI pattern is most commonly associated with displaced scaphoid fractures and SLD [31].
- Perilunate dislocations can be missed [31].
- Assessment of Gilula's lines can aid in the diagnosis of perilunate dislocations [31].
- CT is useful in the diagnosis of suspected carpal fractures and assessment of union [31].
- MRI is useful in detecting suspected fractures and AVN of the carpus [31].
- Wrist arthroscopy can be used as an aid to the diagnosis of ligament injuries and fracture displacement [31].
Treatment
- Early mobilization for patients with distal radius fractures treated with ORIF may have a beneficial effect on function at earlier stages compared to late mobilization [1].
- Mean differences in DASH scores at 6 weeks for early mobilization in distal radius fractures treated with ORIF surpass the minimal clinically important difference [1].
- Substantial variations in surgical direct costs for distal radius ORIF exist [2].
- Implant choice is the predominant driver of cost variation for distal radius ORIF [2].
- The LOS length can be calculated for the Lift-Off Screw technique in a distal radius fracture model [3].
- The Lift-Off Screw technique can potentially be used with any distal radius periarticular locking plate with locking options in the shaft [3].
- Open reduction and internal fixation with a plate offers the best results for adult patients with a distal radius fracture in terms of early and sustained functional recovery [5].
- Open reduction and internal fixation with a plate offers the best results for adult patients with a distal radius fracture in terms of reduction in fracture healing complications [5].
- Radial column plating of the distal radius is a safe treatment modality [6].
- Radial column plating of the distal radius is a valuable adjunct in the setting of complex distal radius fractures [6].
- There is a 28% chance that hardware removal may be required for patients undergoing radial column plating of the distal radius [6].
- Placing the distal row of screws greater than 3mm from subchondral bone in comminuted intra-articular distal radius fractures was associated with increased odds of worsening ulnar variance [8].
- The treatment of displaced intra-articular distal radius fractures with a dorsally versus a volarly placed interlocking plate system demonstrated similar clinical results [9].
- Open reduction and internal fixation is a recommended option for extra-articular distal humeral fractures in elderly patients aged 70 years or older in whom conservative treatment has failed [19].
- The patient in the case of proximal plate migration after internal fixation of a pediatric distal radius fracture required washout and hardware removal, with resolution of symptoms [40].
Complications
- Early mobilization for patients with distal radius fractures treated with ORIF may have a beneficial effect on function at earlier stages compared to late mobilization, with mean differences in DASH scores at 6 weeks surpassing the minimal clinically important difference [1].
- Substantial variations in surgical direct costs for distal radius ORIF exist, and implant choice is the predominant driver [2].
- The LOS length can be calculated, and the lift-off screw technique can potentially be used with any distal radius periarticular locking plate with locking options in the shaft [3].
- Open reduction and internal fixation with a plate offers the best results for adult patients with a distal radius fracture in terms of early and sustained functional recovery and a reduction in fracture healing complications [5].
- Radial column plating of the distal radius is a safe treatment modality, but patients should be counseled that there is a 28% chance that hardware removal may be required [6].
- In a two-center retrospective cohort of comminuted intra-articular distal radius fractures, placing the distal row of screws greater than 3mm from subchondral bone was associated with increased odds of worsening ulnar variance [8].
- The treatment of displaced intra-articular distal radius fractures with a dorsally versus a volarly placed interlocking plate system demonstrated similar clinical results [9].
- A low overall complication rate of 12.3% was found in a retrospective study of 822 patients treated with volar locking plate fixation of distal radius fractures, with 4.8% major and 7.5% minor complications [39].
Recovery
- Early mobilization for patients with distal radius fractures treated with ORIF may have a beneficial effect on function at earlier stages compared to late mobilization [1].
- Mean differences in DASH scores at 6 weeks for early mobilization in distal radius fractures treated with ORIF surpass the minimal clinically important difference [1].
- Substantial variations in surgical direct costs for distal radius ORIF exist [2].
- Implant choice is the predominant driver of cost variation for distal radius ORIF [2].
- Open reduction and internal fixation with a plate offers the best results for adult patients with a distal radius fracture in terms of early and sustained functional recovery [5].
- Open reduction and internal fixation with a plate offers the best results for adult patients with a distal radius fracture in terms of a reduction in fracture healing complications [5].
- Radial column plating of the distal radius is a safe treatment modality [6].
- Radial column plating of the distal radius is a valuable adjunct in the setting of complex distal radius fractures [6].
- There is a 28% chance that hardware removal may be required for patients undergoing radial column plating of the distal radius [6].
- Placing the distal row of screws greater than 3mm from subchondral bone in comminuted intra-articular distal radius fractures was associated with increased odds of worsening ulnar variance [8].
Key Evidence
- [L1] Functionally, at earlier stages, early mobilization for patients with distal radius fractures treated with ORIF may have a beneficial effect compared to late mobilization, with mean differences in DASH scores at 6 weeks surpassing the minimal clinically important difference. [1] (10.1186/s13018-021-02837-0)
- [L3] Substantial variations in surgical direct costs for distal radius ORIF exist, and implant choice is the predominant driver. [2] (10.1016/j.jhsa.2018.04.015)
- [L5] The LOS length can be calculated, and this technique can potentially be used with any distal radius periarticular locking plate with locking options in the shaft. [3] (10.1016/j.jhsa.2018.02.011)
- [L1] A network meta-analysis of randomized trials revealed that open reduction and internal fixation with a plate offers the best results for adult patients with a distal radius fracture, in terms of early and sustained functional recovery and a reduction in fracture healing complications. [5] (10.5435/jaaos-d-18-00424)
- [L4] Radial column plating of the distal radius is a safe treatment modality and a valuable adjunct in the setting of complex distal radius fractures, but patients should be counseled that there is a 28% chance that hardware removal may be required. [6] (10.1177/1558944718760861)
- [L4] In this two-center retrospective cohort of comminuted intra-articular distal radius fractures, placing the distal row of screws greater than 3mm from subchondral bone was associated with increased odds of worsening ulnar variance. [8] (10.1016/j.jhsa.2025.03.016)
- [L3] The treatment of displaced intra-articular distal radius fractures with a dorsally versus a volarly placed interlocking plate system demonstrated similar clinical results. [9] (10.1177/1558944716675129)
- [L4] Osteosynthesis by open reduction and internal fixation is a recommended option for extra-articular distal humeral fractures in elderly patients aged 70 years or older in whom conservative treatment has failed. [19] (10.1016/j.jse.2017.08.024)
- [L4] A low overall complication rate of 12.3% was found, with 4.8% major and 7.5% minor complications. [39] (10.1016/j.jhsa.2022.11.012)
- [L4] The patient required washout and hardware removal, with resolution of his symptoms. [40] (10.1177/15589447221130083)
References
[1] In adults, early mobilization may be beneficial for distal radius fractures treated with open reduction and internal fixation: a systematic review and meta-analysis. Journal of Orthopaedic Surgery and Research. 2021. DOI: 10.1186/s13018-021-02837-0 [2] Evaluation of Factors Driving Cost Variation for Distal Radius Fracture Open Reduction Internal Fixation. The Journal of Hand Surgery. 2018. DOI: 10.1016/j.jhsa.2018.04.015 [3] Lift-Off Screw Results in Accurate Sagittal Tilt Correction in a Distal Radius Fracture Model. The Journal of Hand Surgery. 2018. DOI: 10.1016/j.jhsa.2018.02.011 [5] Interventions for Distal Radius Fractures: A Network Meta-analysis of Randomized Trials. Journal of the American Academy of Orthopaedic Surgeons. 2019. DOI: 10.5435/jaaos-d-18-00424 [6] Complications of Radial Column Plating of the Distal Radius. HAND. 2018. DOI: 10.1177/1558944718760861 [8] The Association Between Distal Screw and Articular Subsidence in the Open Treatment of Intra-articular Distal Radius Fractures. The Journal of Hand Surgery. 2026. DOI: 10.1016/j.jhsa.2025.03.016 [9] Management of Intra-Articular Distal Radius Fractures: Volar or Dorsal Locking Plate—Which Has Fewer Complications?. HAND. 2016. DOI: 10.1177/1558944716675129 [16] Rockwood And Green S Fractures In Adults. 42: Fractures of the Distal Radius and Ulna > Pathoanatomy and Applied Anatomy Relating to Carpal Fractures and Dislocations. [17] Rockwood And Green S Fractures In Adults. 42: Fractures of the Distal Radius and Ulna > Metacarpal Fractures. [19] Open reduction and internal fixation for nonunion of extra-articular distal humeral fractures in patients 70 years and older. Journal of Shoulder and Elbow Surgery. 2018. DOI: 10.1016/j.jse.2017.08.024 [20] Rockwood And Green S Fractures In Adults. 42: Fractures of the Distal Radius and Ulna > Pathoanatomy and Applied Anatomy Relating to Metacarpal Fractures. [21] Rockwood And Green S Fractures In Adults. 42: Fractures of the Distal Radius and Ulna > Pathoanatomy and Applied Anatomy Related to Scaphoid Fractures. [23] Rockwood And Green S Fractures In Adults. 42: Fractures of the Distal Radius and Ulna > Extrinsic Ligaments. [24] Apley And Solomon S Concise System Of Orthopaedics And Trauma. FRACTURES OF THE DISTAL RADIUS IN CHILDREN > Imaging. [25] Rockwood And Green S Fractures In Adults. 42: Fractures of the Distal Radius and Ulna > Assessment of Radiocarpal Instability. [26] Orthopaedic Knowledge Update Trauma. Fractures of the Forearm and Distal Radius > Surgical Approaches. [27] Miller S Review Of Orthopaedics. SECTION 16 PATELLAR TRACKING IN TOTAL KNEE ARTHROPLASTY > DISTAL RADIUS FRACTURES. [30] Apley And Solomon S Concise System Of Orthopaedics And Trauma. FRACTURES OF THE DISTAL RADIUS IN CHILDREN > FRACTURE OF THE SCAPHOID. [31] Rockwood And Green S Fractures In Adults. 42: Fractures of the Distal Radius and Ulna > Secondary Imaging Methods. [32] Rockwood And Green S Fractures In Adults. 42: Fractures of the Distal Radius and Ulna > Dorsal Approach. [34] Aaos Comprehensive Orthopaedic Review 3. Wrist Fractures and Dislocations, Carpal Dissociation, and Distal Radius Fractures > III. Fractures of the Distal Radius. [35] Orthopaedic Knowledge Update Trauma. Fractures of the Forearm and Distal Radius > Forearm Fractures > Galeazzi Fractures. [39] Complications After Volar Locking Plate Fixation of Distal Radius Fractures: A Retrospective Study of 822 Patients. The Journal of Hand Surgery. 2024. DOI: 10.1016/j.jhsa.2022.11.012 [40] Proximal Plate Migration After Internal Fixation of a Pediatric Distal Radius Fracture. HAND. 2023. DOI: 10.1177/15589447221130083





