腕关节融合术
Patients › Rehabilitation
全腕关节融合术(关节融合术)后的康复计划,其中磨损的腕关节通过背侧钢板固定以实现牢固融合,从而按设计不再活动,同时从早期开始保持手指、拇指及前臂旋转的活动能力,并在骨性愈合后逐步恢复握力。
本方案指导您在基兰·希尔帕拉(Kieran Hirpara)医生处接受腕关节融合术(又称腕关节融合,一种将磨损的腕关节永久固定以使其不再活动的操作)后的康复过程。方案首先介绍您的家庭锻炼计划,随后是专为您的手部治疗师撰写的结构化临床方案:请将此页面或其PDF文件带给您的首次治疗就诊,以确保您的康复过程协调一致。您的治疗师可能会根据您的康复进展调整计划。
如果您对术后伤口有任何担忧,请联系诊室。拍摄伤口照片并发送电子邮件供审查通常很有帮助。
预期情况
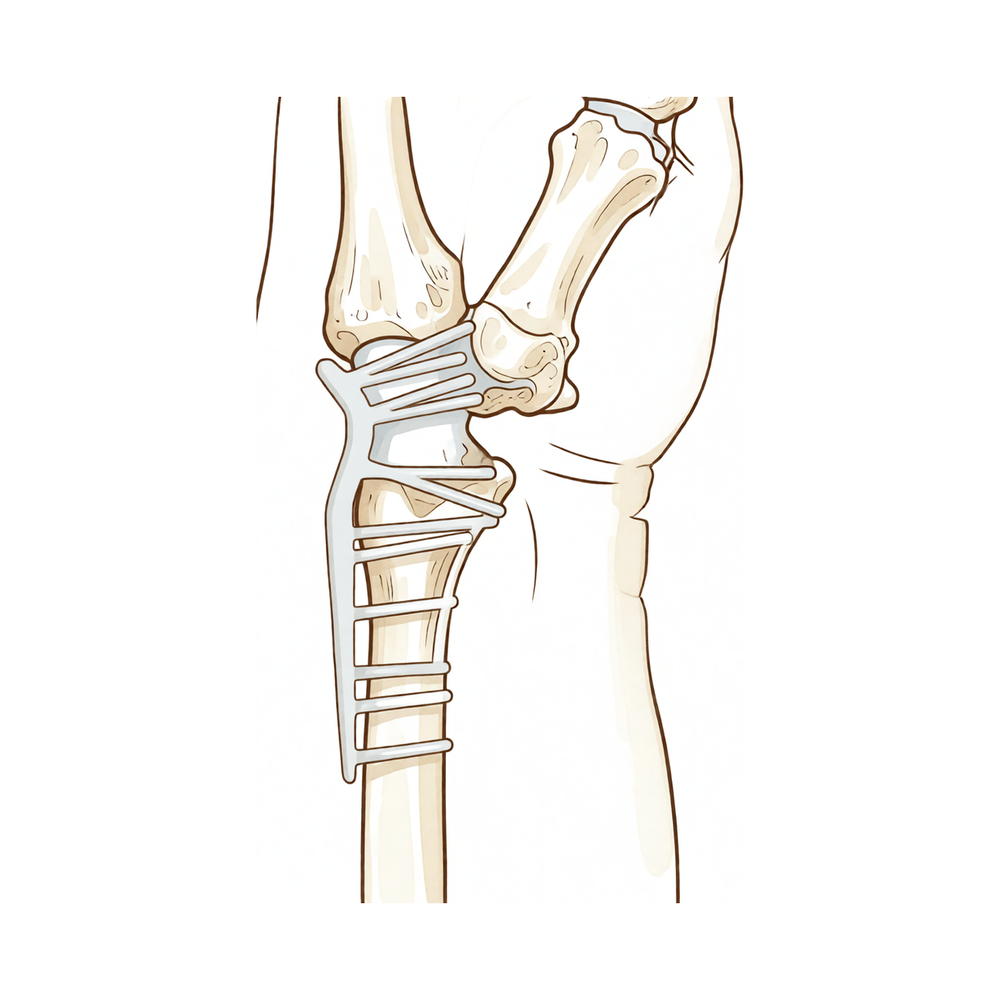
全腕关节融合术适用于所有腕关节均严重磨损(终末期或“全腕”关节炎)且活动时疼痛的腕关节。该手术有意消除腕关节活动,而非试图保留磨损关节的活动度:通过沿腕背侧放置背侧钢板,将前臂骨(桡骨)与手部骨骼(掌骨)固定在一起,使腕关节固定在轻微后伸(轻度背伸)的位置,此位置最有利于抓握。在接下来的数周内,骨骼会愈合(融合)成一个坚实的骨块。
本康复方案的关键理念与大多数手术相反:腕关节应停止活动:这正是治愈手段,而非并发症。 因此,本方案不以恢复腕关节活动度为目标,也不进行屈伸腕关节的锻炼。相反,整个康复过程旨在保护融合术未涉及且对手部功能至关重要的两个方面:
- 手指和拇指必须保持完全活动。 手指僵硬是腕关节融合术失败的主要原因,因此手指和拇指的活动从术后第一天开始。
- 前臂旋转功能(手掌向上和向下的转动)得以保留。 融合术不涉及此动作,且前臂旋转将承担腕关节原有的大部分功能(如转动钥匙、水龙头和门把手),因此从一开始就保持其灵活性。
由于背侧钢板提供了牢固的骨骼固定(稳定固定),仅需佩戴轻型夹板或敷料以提供舒适感,并鼓励早期进行手指和前臂活动,而非限制活动。一旦骨骼愈合(通常在六至八周后),即可开始握力强化训练。许多患者在腕关节融合术后功能良好,且由于抓握不再疼痛,其握力往往较术前疼痛的腕关节有所提高。
注意事项与限制
- 切勿尝试活动腕关节本身:腕关节已按设计实现骨性融合。不存在任何腕关节屈伸锻炼,现在及将来均不可进行。
- 务必从术后第一天起保持手指、拇指及前臂旋转功能的充分活动:这是您能为手部功能恢复所做的最重要事项。
- 遵医嘱佩戴夹板或敷料,直至骨性愈合,以提供舒适与保护;保持其清洁干燥。
- 切勿负重或用力握持,并避免提起超过轻杯重量的物品,直至融合处骨性愈合且获医生许可(通常在术后六至八周):在骨性愈合前负重可能导致内固定钢板或融合失败。
- 佩戴夹板期间或无法安全操控车辆时,切勿驾驶;待拆除夹板且经复查确认您可安全操控方向盘后,方可恢复驾驶。
关于伤口、肿胀及瘢痕管理,请参阅诊所的伤口护理指南。
您的练习
这些是您讲义中的练习。仅在 Hirpara 医生和您的手部治疗师的指导下开始进行。早期练习旨在保护融合术后保留的功能(手指和拇指活动、前臂旋转以及肿胀控制),均不涉及腕关节,腕关节将保持固定。握力强化属于后期阶段,必须在融合愈合且您获得明确许可后方可开始。如果腕背侧出现锐痛,请立即停止任何相关动作。
您的临床方案
本页面其余部分为腕关节融合术后的分阶段康复临床方案。本节内容将提供给您的手部治疗师,每个阶段均以通俗语言解释当前的治疗目标。本方案不设定腕关节活动度(ROM)目标:桡腕关节(通常还包括第三腕掌关节)已通过背侧钢板进行融合。该方案旨在骨性愈合期间维持手指活动度、前臂旋转功能并控制水肿,随后在稳定的内固定结构基础上增强握力。
治疗前,请查阅患者的手术记录和既往病史,并与主刀医生沟通内固定情况(背侧融合钢板;第三腕掌关节是否包含在内或保留)、腕关节融合位置、是否使用骨移植以及骨愈合情况。Hirpara 医生使用背侧钢板将腕关节融合于轻度背伸位;由于固定牢固,仅使用轻便夹板或敷料以提供舒适感,而非长期严格石膏固定,早期手指和前臂活动是首要任务。
第一阶段 — 保护内固定,活动未融合关节(第0至6周)
前六周在保护愈合中的融合部位的同时,保持所有未融合关节的完全活动度。佩戴轻便夹板或敷料以提供舒适感。禁止腕关节活动(内固定设计为刚性结构),重点完全放在手指、拇指、前臂及消肿上。
致手部治疗师:
教育与注意事项 - 夹板/敷料用于舒适和保护,直至临床和影像学证实骨性愈合;鉴于钢板固定稳定,无需进行长期的刚性石膏固定 - 禁止腕关节活动: 桡腕关节/腕掌关节已融合;无关节活动度(ROM)目标 - 禁止负重抓握或提起超过轻握杯子的重量,直至确认愈合 - 监测指僵硬:指僵硬是腕关节融合术后影响预后的主要威胁
管理措施 - 伤口:按医嘱进行外科敷料处理;约10–14天拆线并复查夹板/X线片;监测感染迹象 - 水肿:抬高至心脏水平以上,轻柔的手指泵动练习,必要时冰敷 - 锻炼:从第一天起进行手指和拇指的完全主动关节活动度(AROM)练习(握拳→完全伸展,拇指对掌);前臂主动旋前/旋后;肩关节和肘关节主动活动度练习;禁止腕关节活动,禁止抗阻抓握
进阶标准 - 伤口愈合;维持完全或接近完全的手指关节活动度;约六周时出现早期影像学愈合征象
第二阶段——确认骨性愈合,开始握力负荷(第6至12周)
大约在6至8周时,X线片通常显示融合处正在愈合,一旦外科医生确认愈合,支具即可拆除,并开始握力强化训练。前臂和手指训练继续进行;在确认骨性愈合之前,腕关节保持融合且不负重状态。
致您的手部治疗师:
评估 - 在开始负荷训练前,与主治医生确认愈合状态;测量手指关节活动度(ROM);测量前臂旋转活动范围;建立握力基线;检查伤口/瘢痕
教育和注意事项 - 仅在外科医生确认骨性愈合后(通常为6至8周)开始握力训练和轻度负荷 - 背侧腕部的内固定物位于皮下;注意观察是否有突起/刺激症状并及时报告 - 始终优先确保手指完全活动度
管理 - 练习:一旦确认骨性愈合,进行渐进式握力强化(软球→橡皮泥→分级握力器);伤口愈合后开始瘢痕管理;继续前臂旋转和手指完全活动度;引入轻度的功能性手部使用 - 教育患者,在日常任务(如钥匙、水龙头、旋转动作)中,前臂旋转现在替代了丧失的腕关节活动
进阶标准 - 确认骨性愈合;无痛性轻度握力;手指完全活动度;瘢痕可移动
第三阶段——强化与负荷恢复(第12周及以后)
一旦骨融合牢固,便无需再限制活动以进行保护;手部可按耐受情况承受负荷并逐步加强。握力及手部整体力量在数月内持续改善,通常可优于术前水平,因为此时握持动作已无痛。
致手部治疗师:
评估 - 与健侧对比的握力;功能性及工作/任务特异性测试;内固定物耐受性
教育与注意事项 - 骨愈合后无活动限制;按耐受情况逐步增加负荷 - 重体力/手动负荷应逐步增加;力量提升可持续至约12个月
管理 - 练习:渐进性抗阻握力及前臂强化训练;分级恢复功能性及工作活动;继续任何残留的手指活动度训练 - 若握力达到功能水平且持续改善,并能处理日常活动,可考虑出院;若出现手指僵硬、持续性内固定物刺激或预后不良,请转诊回主治医生
负荷恢复标准 - 骨性融合牢固;握力具有功能性且持续改善;任务特异性负荷无痛
重返工作与活动
在融合愈合之前,只要不用力握持或提起超过轻杯重量的物品,鼓励从术后初期开始进行日常轻度手部活动(如进食、书写、轻度自我护理),以舒适为度。由于佩戴支具期间或无法安全操控车辆时不得驾驶,请在术后早期安排他人协助交通;待拆除支具且经复查确认能够安全操控方向盘后,方可恢复驾驶。
在融合愈合(通常为术后六至八周)并获得医生许可后,方可逐步恢复负重握持、提举和牵拉活动。大多数人可在术后约三个月重返办公室工作或从事轻度劳动,重体力或手工劳动则需更晚,具体进展由 Hirpara 医生和您的手部治疗师根据功能标准而非仅依据术后时间进行评估。握力可持续改善长达一年,且由于原本退变的腕关节不再疼痛,许多患者术后的握力更强,手部活动也更为自如。
您的康复方案
本方案与诊所的一般术后康复建议配合使用:请参阅术后疼痛管理、伤口护理和瘢痕管理。上述分阶段计划反映了全腕关节融合术后的已发表结果和康复指导,您的后续康复将由Hirpara医生和您的手部治疗师根据您关节融合和手部功能的进展情况进行个体化指导。
Evidence & references
Total Wrist Arthrodesis — Procedure Outcomes & Post-operative Rehabilitation (Radiocarpal Fusion, Dorsal Plate)
Topic scope: post-operative rehabilitation after total wrist arthrodesis — permanent surgical fusion of the radiocarpal (and usually the third carpometacarpal) joints with a dorsal arthrodesis plate, for end-stage pancarpal (panarticular) arthritis of the wrist. This is a salvage reconstruction that deliberately abolishes wrist motion, not a motion-preserving operation, so the rehabilitation has no wrist-ROM goal. It is built around preserving the joints the fusion leaves free — the fingers, thumb and forearm rotation — and controlling oedema while the fusion unites, then progressive grip loading once united.
Defining principle of the rehab here: total wrist fusion trades motion for a stable, pain-free wrist. The whole wrist is set solid (radius → metacarpals) in slight extension; loss of wrist movement is the intended endpoint, not a deficit to be rehabilitated. Modern dorsal locking-plate fixation is rigid enough that prolonged casting is unnecessary — so the deliberate priorities are early digital and forearm-rotation motion (digital stiffness is the principal threat to a good result) and swelling control, with grip strengthening deferred until radiographic union (typically 6–8 weeks). The single branch point is union status: loading is gated on the surgeon confirming the fusion has consolidated, after which there are no motion restrictions to protect.
A. PROCEDURE OUTCOMES (total wrist arthrodesis, dorsal plate)
Total wrist arthrodesis is a reliable, durable salvage for the painful, arthritic wrist that has failed non-operative care: the great majority of patients obtain lasting pain relief and a stable hand, accepting the loss of wrist motion in exchange.
- High union rates and durable pain relief. Plate arthrodesis is a well-established, reproducible operation; published series and the JAAOS review of indications and outcomes report reliable fusion, good pain relief and high patient satisfaction, with most patients willing to undergo it again [Wei & Feldon, JAAOS 2017; Shah et al., J Hand Surg Am 2022 — technique/modifications]. Moderate–strong (review + technique series).
- Grip strength is preserved or improves. Because gripping is no longer painful and the wrist is a stable platform, grip strength after fusion is typically equal to or better than the painful pre-operative wrist. A 2026 systematic review and meta-analysis of long-term grip strength after total wrist fusion (comparing inclusion vs sparing of the third CMC joint) confirms maintained long-term grip with comparable complication profiles between the two constructs [Lawson-Smith et al., J Hand Surg Glob Online 2026]. Moderate (SR/meta-analysis).
- Function is good for daily tasks; forearm rotation compensates for lost wrist motion. Patients adapt well because forearm pronation/supination (unaffected by the fusion) substitutes for much of the lost wrist arc in activities such as turning keys, taps and handles. Carpometacarpal-joint– sparing plate designs aim to retain a small amount of motion and reduce distal hardware issues [Briotti et al., HAND 2022 — Medartis CMC-sparing plate]. Moderate (cohort).
- Complications are defined and manageable. Principal complications are nonunion, hardware prominence/irritation requiring plate removal (the dorsal plate is subcutaneous), wound issues, and adjacent-segment problems (distal radioulnar joint / digital stiffness). These are recognised, generally treatable, and informed-consent staples rather than common catastrophes [Wei & Feldon, JAAOS 2017; Kalb & Prommersberger, Oper Orthop Traumatol 2009 — AO plate technique]. Moderate.
B. REHABILITATION / THERAPY EVIDENCE
The rehab questions after total wrist fusion are different from a motion-preserving operation: there is no wrist arc to recover. The evidence and consensus instead converge on early mobilisation of the unfused joints, oedema control, and union-gated grip loading, exploiting the stability of modern plate fixation.
- Stable plate fixation permits early digital and forearm motion. Rigid dorsal locking-plate constructs are robust enough that prolonged rigid immobilisation is unnecessary; a light splint or dressing for comfort, with immediate finger, thumb and forearm-rotation motion, is the intended default [Shah et al., J Hand Surg Am 2022; Kalb & Prommersberger, Oper Orthop Traumatol 2009]. Moderate (technique consensus).
- Preserving digital range is the priority — stiffness is the main avoidable failure. Because the hand's function after fusion depends entirely on the joints left mobile, full active finger and thumb range from day one, plus preserved forearm rotation, is the core therapeutic aim. This is a mechanistic/consensus position rather than one from comparative rehab trials. Weak–moderate (mechanism strong, dedicated rehab RCTs absent).
- Grip strengthening is deferred to union, then progressed freely. Loaded grip is withheld until the surgeon confirms radiographic union (commonly 6–8 weeks), after which there are no motion restrictions and strengthening is progressed as tolerated; grip continues to improve for several months. Consensus / protocol-based.
- Hand therapy targets the free joints, not the wrist. Published patient-guidance protocols and surgical references describe early referral to a hand therapist for finger and forearm mobility and later putty-based grip strengthening — there is no wrist-ROM component by design [AAOS OrthoInfo — Wrist Fusion; institutional post-op protocols]. Consensus (patient-guidance).
Recovery trajectory (expected, evidence-anchored)
| Phase | Window | Restraint | Hand use / therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Protect construct, mobilise free joints | Week 0–6 | Light splint/dressing for comfort; no wrist motion (fused) | Elevate; immediate full finger + thumb AROM; forearm pronation/supination; elbow/shoulder ROM; oedema control | Light functional use only; no loaded grip / lifting > a light cup | Sutures + splint/X-ray review ~10–14 days. Digital stiffness is the chief threat |
| II — Confirm union, begin grip loading | Week 6–12 | Loading gated on surgeon-confirmed union (≈6–8 wk) | Splint discarded at union; progressive grip (ball → putty → grippers); scar massage once healed; continue forearm + digital ROM | Grip introduced light → graded after union | Forearm rotation substitutes for lost wrist motion. Watch dorsal hardware prominence |
| III — Strengthening & return to load | Week 12 → 12 months | None once united | Progressive resisted grip/forearm strengthening; work-/task-specific loading | Full load as tolerated; heavy/manual built up gradually | Office/light work ~3 months; strength improves up to ~12 months, often exceeding pre-op (pain-free grip) |
(Phase windows mirror the precautions and recovery structure in the patient protocol; they are typical guides anchored to union, not trial-derived deadlines.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY
- Fusion vs total wrist arthroplasty. The central modern controversy. Systematic review of total wrist arthroplasty versus arthrodesis (originally in rheumatoid disease) found insufficient evidence to declare either superior, with arthroplasty preserving some motion at the cost of higher revision/implant-related complications, and fusion offering durability at the cost of motion [Cavaliere & Chung, Plast Reconstr Surg 2008]. A cost-utility analysis found arthrodesis and arthroplasty both reasonable, with trade-offs in motion, complications and cost [Cavaliere & Chung, J Hand Surg Am 2010]. The "where are we now" synthesis frames the choice as patient-specific (demand, bilateral disease, expectations) rather than a settled winner [Jump, Trail & Talwalkar, J Hand Surg Eur 2025]. Moderate; genuine equipoise.
- Arthrodesis as salvage for failed arthroplasty. Total wrist fusion reliably salvages a failed total wrist arthroplasty, though such salvage fusions behave somewhat differently (bone loss, grafting) from primary arthrodesis [Zijlker et al., J Hand Surg Eur 2021]. Moderate.
- Include or spare the third CMC joint. Constructs differ in whether the plate crosses the third carpometacarpal joint. Long-term grip and complication outcomes are broadly comparable between inclusion and sparing, with CMC-sparing designs aiming to reduce distal hardware issues and retain a trace of motion [Lawson-Smith et al., J Hand Surg Glob Online 2026; Briotti et al., HAND 2022]. Moderate.
- Hardware prominence and removal. The subcutaneous dorsal plate is a recognised source of irritation and a common reason for elective hardware removal once the fusion is solid — expected, not a failure of the operation [Wei & Feldon, JAAOS 2017]. Moderate.
- Special populations. In spastic/neurological wrists (e.g. cerebral palsy), fusion changes hand function in nuanced ways — improving positioning but with task-specific trade-offs — underlining that the goal is a useful stable position, not motion [Hargreaves, Warwick & Tonkin, J Hand Surg Br 2000]. Moderate (specialised cohort).
D. EVIDENCE STRENGTH FLAGS (summary)
- STRONG (SR / meta-analysis): preserved-to-improved long-term grip strength after total wrist fusion; comparable outcomes between CMC-inclusion and CMC-sparing constructs [Lawson-Smith et al. 2026].
- MODERATE: reliable union, durable pain relief and high satisfaction with plate arthrodesis [Wei & Feldon 2017; Shah et al. 2022]; genuine equipoise between fusion and arthroplasty with motion-vs-durability/complication trade-offs [Cavaliere & Chung 2008, 2010; Jump et al. 2025]; fusion as salvage for failed arthroplasty [Zijlker et al. 2021]; defined complication set (nonunion, hardware removal, DRUJ/digital adjacent issues).
- WEAK / CONSENSUS: the specific early digital/forearm-motion, union-gated grip rehabilitation programme (mechanistically rationalised — stiffness avoidance — with no dedicated rehab RCTs); exact phase timings (typical, anchored to union rather than trial-derived); stable-fixation early-motion default from technique consensus [Shah et al. 2022; Kalb & Prommersberger 2009].
CITATIONS
RAG corpus (180,000+ Orthopaedic articles)
- Total Wrist Arthrodesis: Indications and Clinical Outcomes. J Am Acad Orthop Surg. 2017. DOI: 10.5435/jaaos-d-15-00424
- Radiocarpal Fusion: Indications, Technique, and Modifications. J Hand Surg Am. 2022. DOI: 10.1016/j.jhsa.2022.04.002
- Long-term Grip Strength and Complications After Total Wrist Fusion With and Without Inclusion of the Third Carpometacarpal Joint: A Systematic Review and Meta-analysis. J Hand Surg Glob Online. 2026. DOI: 10.1016/j.jhsg.2026.101022
- Wrist Arthrodesis Using the Medartis Carpometacarpal Joint Sparing Plate. HAND. 2022. DOI: 10.1177/15589447221141474
- A Systematic Review of Total Wrist Arthroplasty Compared with Total Wrist Arthrodesis for Rheumatoid Arthritis. Plast Reconstr Surg. 2008. DOI: 10.1097/prs.0b013e318180ece3
- A Cost-Utility Analysis of Nonsurgical Management, Total Wrist Arthroplasty, and Total Wrist Arthrodesis in Rheumatoid Arthritis. J Hand Surg Am. 2010. DOI: 10.1016/j.jhsa.2009.12.013
- Arthrodesis or arthroplasty, complete or partial: where are we at in the 21st century? J Hand Surg Eur Vol. 2025. DOI: 10.1177/17531934241296758
- Comparative outcomes of total wrist arthrodesis for salvage of failed total wrist arthroplasty and primary wrist arthrodesis. J Hand Surg Eur Vol. 2021. DOI: 10.1177/17531934211057389
- Die vollständige Versteifung des Handgelenks mit der AO-Handgelenk-Arthrodesenplatte (Complete wrist arthrodesis with the AO wrist arthrodesis plate). Oper Orthop Traumatol. 2009. DOI: 10.1007/s00064-009-1905-2
- Changes in Hand Function Following Wrist Arthrodesis in Cerebral Palsy. J Hand Surg Br. 2000. DOI: 10.1054/jhsb.2000.0366
Wrist-fusion rehabilitation / patient-guidance literature (URLs)
- American Academy of Orthopaedic Surgeons — Wrist Fusion (Wrist Arthrodesis), OrthoInfo (recovery timeline; fusion heals ~8–12 weeks; the fused wrist no longer moves; therapy for joints not fused). https://orthoinfo.aaos.org/en/treatment/wrist-fusion-wrist-arthrodesis/
- Wrist Arthrodesis Technique — postoperative care and approach considerations. Medscape eMedicine. https://emedicine.medscape.com/article/1241236-technique
- Total Wrist Arthrodesis (Wrist Fusion) — procedure and rehabilitation overview. Resurgens Orthopaedics. https://www.resurgens.com/hand-wrist/procedures/wrist-fusion-total-wrist-arthrodesis
- Full Wrist Fusion — Post-Operative Rehabilitation Protocol (institutional hand-therapy protocol; early digital/forearm motion, union-gated grip strengthening). Alaska Orthopedic. https://www.akortho.com/wp-content/uploads/Full-Wrist-Fusion.pdf





