Wrist Fusion Info Evidence
Reviewed by Dr Kieran Hirpara, Specialist Orthopaedic Surgeon Last reviewed
This protocol guides your recovery after a total wrist fusion (also called wrist arthrodesis, an operation that permanently joins the worn-out wrist solid so it no longer moves) with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It begins with your home exercise program, followed by the structured clinical protocol written for your hand therapist: bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your therapist may adjust the plan depending on how your recovery progresses.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect
A total wrist fusion is done for a wrist that is worn out across all of its joints (end-stage, or "pancarpal", arthritis) and is painful with movement. Rather than trying to keep a worn joint moving, the operation takes the movement away on purpose: the forearm bone (the radius) is joined to the hand bones (the metacarpals) with a dorsal plate running along the back of the wrist, setting the wrist solid in a position of slight backward tilt (slight extension) that is best for gripping. Over the following weeks the bones knit together (unite) into one solid block.
The key idea of this recovery is the opposite of most operations: the wrist is meant to stop moving: that is the cure, not a complication. So there is no goal of regaining wrist movement, and no exercises to bend or straighten the wrist. Instead, the whole rehabilitation protects two things that the fusion does not touch and that matter enormously for hand function:
- Your fingers and thumb must stay fully mobile. Stiff fingers are the main thing that lets a wrist fusion down, so finger and thumb movement starts from day one.
- Forearm rotation (turning your palm up and down) is preserved. The fusion does not involve this movement, and it takes over a lot of what the wrist used to do (turning keys, taps and doorhandles) so it is kept supple from the start.
Because the dorsal plate holds the bones firmly (stable fixation), a splint is worn for about six weeks while the bone unites, and early finger and forearm movement is encouraged rather than held back. Once the surgeon confirms union, grip strengthening begins. Many people function very well after a wrist fusion, and because gripping is no longer painful, grip strength often improves compared with the painful wrist before surgery.
Precautions and limitations
- Do NOT try to move the wrist itself: it is fused solid by design. There are no wrist-bending exercises, now or ever.
- Do keep your fingers, thumb and forearm rotation moving fully from day one: this is the single most important thing you can do for your hand.
- Wear your splint or dressing as directed for comfort and protection until the bone has united; keep it clean and dry.
- Do NOT load or grip hard, and avoid lifting more than a light cup, until the fusion has united and you are cleared (usually around six to eight weeks): heavy loading before union risks the plate or the fusion failing.
- Do NOT drive while you are in a splint or cannot safely control the car; driving resumes once you are out of the splint and can manage the wheel, as confirmed at your review.
For wound, swelling and scar management, see the practice's wound care guidance.
Your exercises
Kieran Hirpara 4.0
Finger and thumb movement
Keep your fingers and thumb moving fully from the very first days. Make a complete fist, then open the hand wide and stretch the fingers straight; then touch your thumb to the tip of each finger in turn. Your wrist does not move — that is normal and intended — but the fingers and thumb must stay loose and fully mobile, because stiffness here is the main thing that limits the hand after a wrist fusion.
10 times each, several times a day, from day one
Kieran Hirpara 4.0
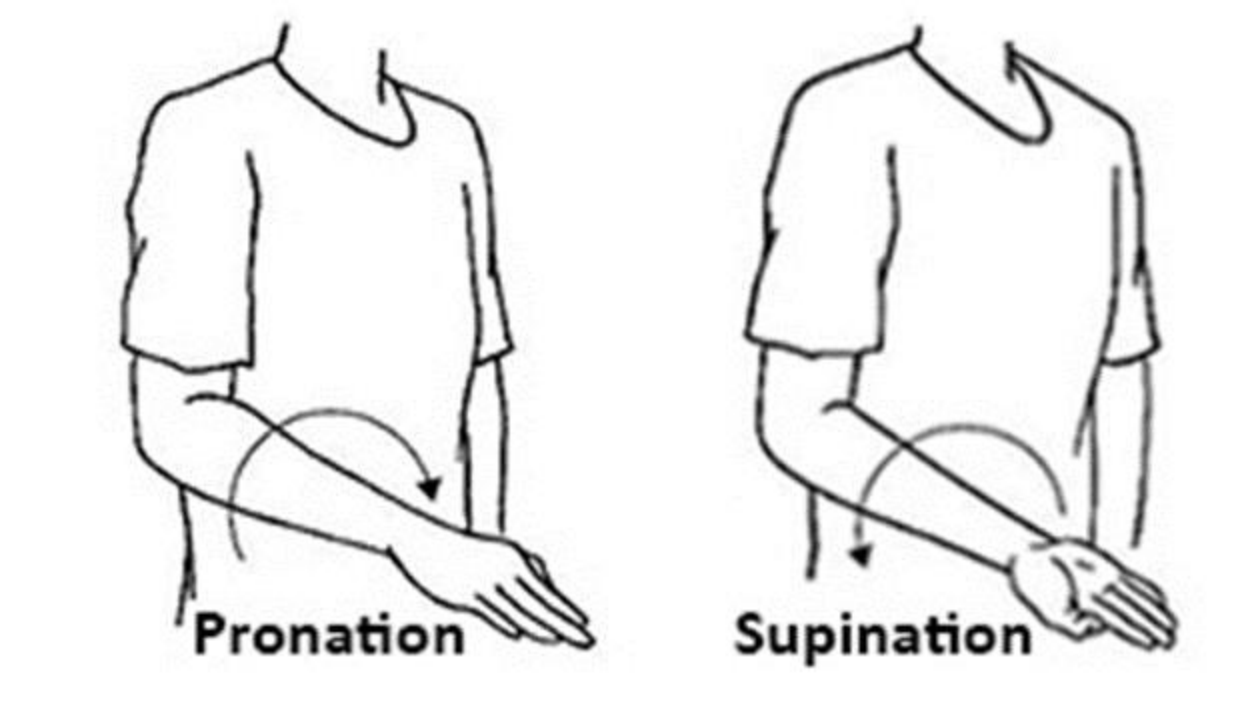
Forearm rotation (palm up / palm down)
With your elbow tucked at your side and bent to a right angle, gently turn your palm up towards the ceiling, then down towards the floor. The fusion does not involve these turning movements, so they stay free — keeping them supple is important, as turning the forearm does a lot of the work the wrist used to do (turning a key, a doorknob, a tap).
10 times each direction, 2–3 times a day

Kieran Hirpara 4.0
Swelling control
For the first couple of weeks, rest your hand raised up on pillows above the level of your heart whenever you sit or lie down, and pump your fingers gently open and closed. This drains the swelling that always follows hand surgery; less swelling means the fingers move more freely and the wound settles faster.
Elevate whenever resting; finger pumps 10 times, hourly while awake
Kieran Hirpara 4.0
Scar care
Once the wound has fully healed and there is no scab, massage the scar over the back of your wrist with a little moisturiser, using small firm circles. This keeps the scar soft and stops it sticking to the plate and tendons underneath. Your hand therapist will start this at the right time.
A few minutes, 2–3 times a day, once healed

Kieran Hirpara 4.0
Grip strengthening after union
A LATER exercise — only once the fusion has united (usually around six to eight weeks) and you are cleared. Squeeze a soft ball or therapy putty in your palm and hold, then release. The fused wrist gives the hand a stable, pain-free base to grip from, so grip strength usually improves over the following months. Build it up gradually.
10–15 squeezes, 2–3 times a day, once cleared after union
These are the exercises from your handout. Start them only as guided by Dr Hirpara and your hand therapist. The early exercises all protect what the fusion leaves free (finger and thumb movement, forearm rotation, and swelling control) and none of them involve the wrist, which stays solid. Grip strengthening belongs to a later phase and should not be started until the fusion has united and you are specifically cleared. Stop anything that causes sharp pain over the back of the wrist.
Your clinical protocol
The rest of this page is the staged clinical protocol for rehabilitation after total wrist arthrodesis. This section is to be provided to your hand therapist, and each phase opens with a plain-English explanation of what is happening. There is no wrist-ROM goal: the radiocarpal (and usually third carpometacarpal) joints are fused with a dorsal plate. The protocol exists to preserve digital range, forearm rotation and oedema control while the fusion unites, then build grip on the stable construct.
Prior to treatment, check the patient's operation report and past medical history, and liaise with the treating surgeon regarding the construct (dorsal arthrodesis plate; whether the third CMC joint is included or spared), the fused wrist position, any bone graft used, and the union status. Dr Hirpara fuses the wrist in slight extension with a dorsal plate; fixation is stable, so a light splint/dressing for comfort is used rather than prolonged rigid casting, and early digital and forearm motion is the priority.
Phase I — protect the construct, mobilise the free joints (weeks 0 to 6)
The first six weeks protect the healing fusion while keeping everything that is not fused fully mobile. A light splint or dressing is worn for comfort. There is no wrist motion (the construct is rigid by design) and the focus is entirely on the fingers, thumb, forearm and swelling.
For your hand therapist:
Education and precautions - Splint/dressing for comfort and protection until clinical and radiographic union; no rigid prolonged casting required given stable plate fixation - No wrist mobilisation: the radiocarpal/CMC construct is fused; there is no ROM target - No loaded grip or lifting beyond a light cup until union confirmed - Watch for digital stiffness: the principal threat to outcome after wrist fusion
Management - Wound: surgical dressings as directed; sutures out and splint/X-ray review at around 10–14 days; monitor for infection - Oedema: elevation above heart level, gentle digital pumping, ice as needed - Exercises: full active finger and thumb AROM (composite fist → full extension, thumb opposition) from day one; active forearm pronation/supination; active shoulder and elbow ROM; no wrist motion, no resisted grip
Criteria to progress - Wound healed; full or near-full digital ROM maintained; early radiographic signs of union at around six weeks
Phase II — confirm union, begin grip loading (weeks 6 to 12)
From about six weeks the fusion is usually uniting on X-ray, and once the surgeon confirms this the splint is discarded and grip strengthening begins. Forearm and finger work continues; the wrist remains fused and unloaded only until union is confirmed.
For your hand therapist:
Assessments - Confirm union status with the treating surgeon before loading; digital ROM; forearm rotation arc; grip baseline; wound/scar review
Education and precautions - Begin grip and light loading only after the surgeon confirms union (commonly six to eight weeks) - Hardware over the dorsal wrist is subcutaneous; watch for prominence/irritation and report it - Continue to prioritise full digital ROM throughout
Management - Exercises: progressive grip strengthening (soft ball → putty → graded grippers) once union confirmed; commence scar management once wound healed; continue forearm rotation and full digital ROM; introduce light functional hand use - Educate that forearm rotation now substitutes for lost wrist motion in daily tasks (keys, taps, turning)
Criteria to progress - Confirmed union; pain-free light grip; full digital ROM; scar mobile
Phase III — strengthening and return to load (weeks 12 and beyond)
Once the fusion is solid, there are no movement restrictions to protect; the hand can be loaded as tolerated and built up. Grip and overall hand strength continue improving for several months, often to better than before surgery because gripping is now pain-free.
For your hand therapist:
Assessments - Grip strength versus the other side; functional and work-/task-specific testing; hardware tolerance
Education and precautions - No movement restrictions once united; progress load as tolerated - Heavy/manual loading built up gradually; full strength gains continue up to around twelve months
Management - Exercises: progressive resisted grip and forearm strengthening; graded return to functional and work tasks; continue any residual digital mobility work - Consider discharge once grip is functional and improving and daily tasks are managed; refer back to the treating doctor if digital stiffness, persistent hardware irritation, or a poor outcome develops
Criteria for return to load - Solid union; functional, improving grip; pain-free task-specific loading
Getting back to work and activity
Light everyday hand use (eating, writing, light self-care) is encouraged from the start, within comfort, as long as you are not gripping hard or lifting more than a light cup before the fusion has united. Because you must not drive while in a splint or unable to safely control the car, plan for help with transport in the early weeks; driving resumes once you are out of the splint and can manage the wheel, as confirmed at your review.
Loaded gripping, lifting and pulling wait until the fusion has united (usually around six to eight weeks) and you are cleared, and are then built up gradually. Most people are back to office or light work by around three months, with heavier or manual work later, on a criterion-based progression judged by Dr Hirpara and your hand therapist rather than the calendar alone. Strength keeps improving for up to a year, and because the worn-out wrist is no longer painful, many people grip more strongly and use the hand more freely than they could before surgery.
After your protocol
This protocol works alongside the practice's general recovery advice: see managing post-operative pain, wound care and scar management. The phased plan above reflects published outcomes and rehabilitation guidance after total wrist arthrodesis, and your ongoing recovery is guided individually by Dr Hirpara and your hand therapist according to how your fusion and hand progress.
Evidence & references
Topic scope: post-operative rehabilitation after total wrist arthrodesis — permanent surgical fusion of the radiocarpal (and usually the third carpometacarpal) joints with a dorsal arthrodesis plate, for end-stage pancarpal (panarticular) arthritis of the wrist. This is a salvage reconstruction that deliberately abolishes wrist motion, not a motion-preserving operation, so the rehabilitation has no wrist-ROM goal. It is built around preserving the joints the fusion leaves free — the fingers, thumb and forearm rotation — and controlling oedema while the fusion unites, then progressive grip loading once united.
Defining principle of the rehab here: total wrist fusion trades motion for a stable, pain-free wrist. The whole wrist is set solid (radius → metacarpals) in slight extension; loss of wrist movement is the intended endpoint, not a deficit to be rehabilitated. Modern dorsal locking-plate fixation is rigid enough that prolonged casting is unnecessary — so the deliberate priorities are early digital and forearm-rotation motion (digital stiffness is the principal threat to a good result) and swelling control, with grip strengthening deferred until radiographic union (typically 6–8 weeks). The single branch point is union status: loading is gated on the surgeon confirming the fusion has consolidated, after which there are no motion restrictions to protect.
A. PROCEDURE OUTCOMES (total wrist arthrodesis, dorsal plate)
Total wrist arthrodesis is a reliable, durable salvage for the painful, arthritic wrist that has failed non-operative care: the great majority of patients obtain lasting pain relief and a stable hand, accepting the loss of wrist motion in exchange.
- High union rates and durable pain relief. Plate arthrodesis is a well-established, reproducible operation; published series and the JAAOS review of indications and outcomes report reliable fusion, good pain relief and high patient satisfaction, with most patients willing to undergo it again [Wei & Feldon, JAAOS 2017; Shah et al., J Hand Surg Am 2022 — technique/modifications]. Moderate–strong (review + technique series).
- Grip strength is preserved or improves. Because gripping is no longer painful and the wrist is a stable platform, grip strength after fusion is typically equal to or better than the painful pre-operative wrist. A 2026 systematic review and meta-analysis of long-term grip strength after total wrist fusion (comparing inclusion vs sparing of the third CMC joint) confirms maintained long-term grip with comparable complication profiles between the two constructs [Lawson-Smith et al., J Hand Surg Glob Online 2026]. Moderate (SR/meta-analysis).
- Function is good for daily tasks; forearm rotation compensates for lost wrist motion. Patients adapt well because forearm pronation/supination (unaffected by the fusion) substitutes for much of the lost wrist arc in activities such as turning keys, taps and handles. Carpometacarpal-joint– sparing plate designs aim to retain a small amount of motion and reduce distal hardware issues [Briotti et al., HAND 2022 — Medartis CMC-sparing plate]. Moderate (cohort).
- Complications are defined and manageable. Principal complications are nonunion, hardware prominence/irritation requiring plate removal (the dorsal plate is subcutaneous), wound issues, and adjacent-segment problems (distal radioulnar joint / digital stiffness). These are recognised, generally treatable, and informed-consent staples rather than common catastrophes [Wei & Feldon, JAAOS 2017; Kalb & Prommersberger, Oper Orthop Traumatol 2009 — AO plate technique]. Moderate.
B. REHABILITATION / THERAPY EVIDENCE
The rehab questions after total wrist fusion are different from a motion-preserving operation: there is no wrist arc to recover. The evidence and consensus instead converge on early mobilisation of the unfused joints, oedema control, and union-gated grip loading, exploiting the stability of modern plate fixation.
- Stable plate fixation permits early digital and forearm motion. Rigid dorsal locking-plate constructs are robust enough that prolonged rigid immobilisation is unnecessary; a light splint or dressing for comfort, with immediate finger, thumb and forearm-rotation motion, is the intended default [Shah et al., J Hand Surg Am 2022; Kalb & Prommersberger, Oper Orthop Traumatol 2009]. Moderate (technique consensus).
- Preserving digital range is the priority — stiffness is the main avoidable failure. Because the hand's function after fusion depends entirely on the joints left mobile, full active finger and thumb range from day one, plus preserved forearm rotation, is the core therapeutic aim. This is a mechanistic/consensus position rather than one from comparative rehab trials. Weak–moderate (mechanism strong, dedicated rehab RCTs absent).
- Grip strengthening is deferred to union, then progressed freely. Loaded grip is withheld until the surgeon confirms radiographic union (commonly 6–8 weeks), after which there are no motion restrictions and strengthening is progressed as tolerated; grip continues to improve for several months. Consensus / protocol-based.
- Hand therapy targets the free joints, not the wrist. Published patient-guidance protocols and surgical references describe early referral to a hand therapist for finger and forearm mobility and later putty-based grip strengthening — there is no wrist-ROM component by design [AAOS OrthoInfo — Wrist Fusion; institutional post-op protocols]. Consensus (patient-guidance).
Recovery trajectory (expected, evidence-anchored)
| Phase | Window | Restraint | Hand use / therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Protect construct, mobilise free joints | Week 0–6 | Light splint/dressing for comfort; no wrist motion (fused) | Elevate; immediate full finger + thumb AROM; forearm pronation/supination; elbow/shoulder ROM; oedema control | Light functional use only; no loaded grip / lifting > a light cup | Sutures + splint/X-ray review ~10–14 days. Digital stiffness is the chief threat |
| II — Confirm union, begin grip loading | Week 6–12 | Loading gated on surgeon-confirmed union (≈6–8 wk) | Splint discarded at union; progressive grip (ball → putty → grippers); scar massage once healed; continue forearm + digital ROM | Grip introduced light → graded after union | Forearm rotation substitutes for lost wrist motion. Watch dorsal hardware prominence |
| III — Strengthening & return to load | Week 12 → 12 months | None once united | Progressive resisted grip/forearm strengthening; work-/task-specific loading | Full load as tolerated; heavy/manual built up gradually | Office/light work ~3 months; strength improves up to ~12 months, often exceeding pre-op (pain-free grip) |
(Phase windows mirror the precautions and recovery structure in the patient protocol; they are typical guides anchored to union, not trial-derived deadlines.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY
- Fusion vs total wrist arthroplasty. The central modern controversy. Systematic review of total wrist arthroplasty versus arthrodesis (originally in rheumatoid disease) found insufficient evidence to declare either superior, with arthroplasty preserving some motion at the cost of higher revision/implant-related complications, and fusion offering durability at the cost of motion [Cavaliere & Chung, Plast Reconstr Surg 2008]. A cost-utility analysis found arthrodesis and arthroplasty both reasonable, with trade-offs in motion, complications and cost [Cavaliere & Chung, J Hand Surg Am 2010]. The "where are we now" synthesis frames the choice as patient-specific (demand, bilateral disease, expectations) rather than a settled winner [Jump, Trail & Talwalkar, J Hand Surg Eur 2025]. Moderate; genuine equipoise.
- Arthrodesis as salvage for failed arthroplasty. Total wrist fusion reliably salvages a failed total wrist arthroplasty, though such salvage fusions behave somewhat differently (bone loss, grafting) from primary arthrodesis [Zijlker et al., J Hand Surg Eur 2021]. Moderate.
- Include or spare the third CMC joint. Constructs differ in whether the plate crosses the third carpometacarpal joint. Long-term grip and complication outcomes are broadly comparable between inclusion and sparing, with CMC-sparing designs aiming to reduce distal hardware issues and retain a trace of motion [Lawson-Smith et al., J Hand Surg Glob Online 2026; Briotti et al., HAND 2022]. Moderate.
- Hardware prominence and removal. The subcutaneous dorsal plate is a recognised source of irritation and a common reason for elective hardware removal once the fusion is solid — expected, not a failure of the operation [Wei & Feldon, JAAOS 2017]. Moderate.
- Special populations. In spastic/neurological wrists (e.g. cerebral palsy), fusion changes hand function in nuanced ways — improving positioning but with task-specific trade-offs — underlining that the goal is a useful stable position, not motion [Hargreaves, Warwick & Tonkin, J Hand Surg Br 2000]. Moderate (specialised cohort).
D. EVIDENCE STRENGTH FLAGS (summary)
- STRONG (SR / meta-analysis): preserved-to-improved long-term grip strength after total wrist fusion; comparable outcomes between CMC-inclusion and CMC-sparing constructs [Lawson-Smith et al. 2026].
- MODERATE: reliable union, durable pain relief and high satisfaction with plate arthrodesis [Wei & Feldon 2017; Shah et al. 2022]; genuine equipoise between fusion and arthroplasty with motion-vs-durability/complication trade-offs [Cavaliere & Chung 2008, 2010; Jump et al. 2025]; fusion as salvage for failed arthroplasty [Zijlker et al. 2021]; defined complication set (nonunion, hardware removal, DRUJ/digital adjacent issues).
- WEAK / CONSENSUS: the specific early digital/forearm-motion, union-gated grip rehabilitation programme (mechanistically rationalised — stiffness avoidance — with no dedicated rehab RCTs); exact phase timings (typical, anchored to union rather than trial-derived); stable-fixation early-motion default from technique consensus [Shah et al. 2022; Kalb & Prommersberger 2009].
CITATIONS
RAG corpus (180,000+ Orthopaedic articles)
- Total Wrist Arthrodesis: Indications and Clinical Outcomes. J Am Acad Orthop Surg. 2017. DOI: 10.5435/jaaos-d-15-00424
- Radiocarpal Fusion: Indications, Technique, and Modifications. J Hand Surg Am. 2022. DOI: 10.1016/j.jhsa.2022.04.002
- Long-term Grip Strength and Complications After Total Wrist Fusion With and Without Inclusion of the Third Carpometacarpal Joint: A Systematic Review and Meta-analysis. J Hand Surg Glob Online. 2026. DOI: 10.1016/j.jhsg.2026.101022
- Wrist Arthrodesis Using the Medartis Carpometacarpal Joint Sparing Plate. HAND. 2022. DOI: 10.1177/15589447221141474
- A Systematic Review of Total Wrist Arthroplasty Compared with Total Wrist Arthrodesis for Rheumatoid Arthritis. Plast Reconstr Surg. 2008. DOI: 10.1097/prs.0b013e318180ece3
- A Cost-Utility Analysis of Nonsurgical Management, Total Wrist Arthroplasty, and Total Wrist Arthrodesis in Rheumatoid Arthritis. J Hand Surg Am. 2010. DOI: 10.1016/j.jhsa.2009.12.013
- Arthrodesis or arthroplasty, complete or partial: where are we at in the 21st century? J Hand Surg Eur Vol. 2025. DOI: 10.1177/17531934241296758
- Comparative outcomes of total wrist arthrodesis for salvage of failed total wrist arthroplasty and primary wrist arthrodesis. J Hand Surg Eur Vol. 2021. DOI: 10.1177/17531934211057389
- Die vollständige Versteifung des Handgelenks mit der AO-Handgelenk-Arthrodesenplatte (Complete wrist arthrodesis with the AO wrist arthrodesis plate). Oper Orthop Traumatol. 2009. DOI: 10.1007/s00064-009-1905-2
- Changes in Hand Function Following Wrist Arthrodesis in Cerebral Palsy. J Hand Surg Br. 2000. DOI: 10.1054/jhsb.2000.0366
Wrist-fusion rehabilitation / patient-guidance literature (URLs)
- American Academy of Orthopaedic Surgeons — Wrist Fusion (Wrist Arthrodesis), OrthoInfo (recovery timeline; fusion heals ~8–12 weeks; the fused wrist no longer moves; therapy for joints not fused). https://orthoinfo.aaos.org/en/treatment/wrist-fusion-wrist-arthrodesis/
- Wrist Arthrodesis Technique — postoperative care and approach considerations. Medscape eMedicine. https://emedicine.medscape.com/article/1241236-technique
- Total Wrist Arthrodesis (Wrist Fusion) — procedure and rehabilitation overview. Resurgens Orthopaedics. https://www.resurgens.com/hand-wrist/procedures/wrist-fusion-total-wrist-arthrodesis
- Full Wrist Fusion — Post-Operative Rehabilitation Protocol (institutional hand-therapy protocol; early digital/forearm motion, union-gated grip strengthening). Alaska Orthopedic. https://www.akortho.com/wp-content/uploads/Full-Wrist-Fusion.pdf





