Gout in the Hand, Wrist and Elbow Info In-depth
Last reviewed
Patients › General-Health
Gout in the upper limb — what causes the attacks and lumps (tophi), how flares and high urate are treated, and when surgery is needed.
What you're feeling
Gout often announces itself overnight. A joint (sometimes the base of the thumb, a knuckle, the wrist, or the point of the elbow) becomes intensely painful over just a few hours. It looks hot, red and swollen, and is so tender that even the weight of a bedsheet feels unbearable. This is a flare, and the first one frequently lands in the foot, but the hand and wrist are common sites too.
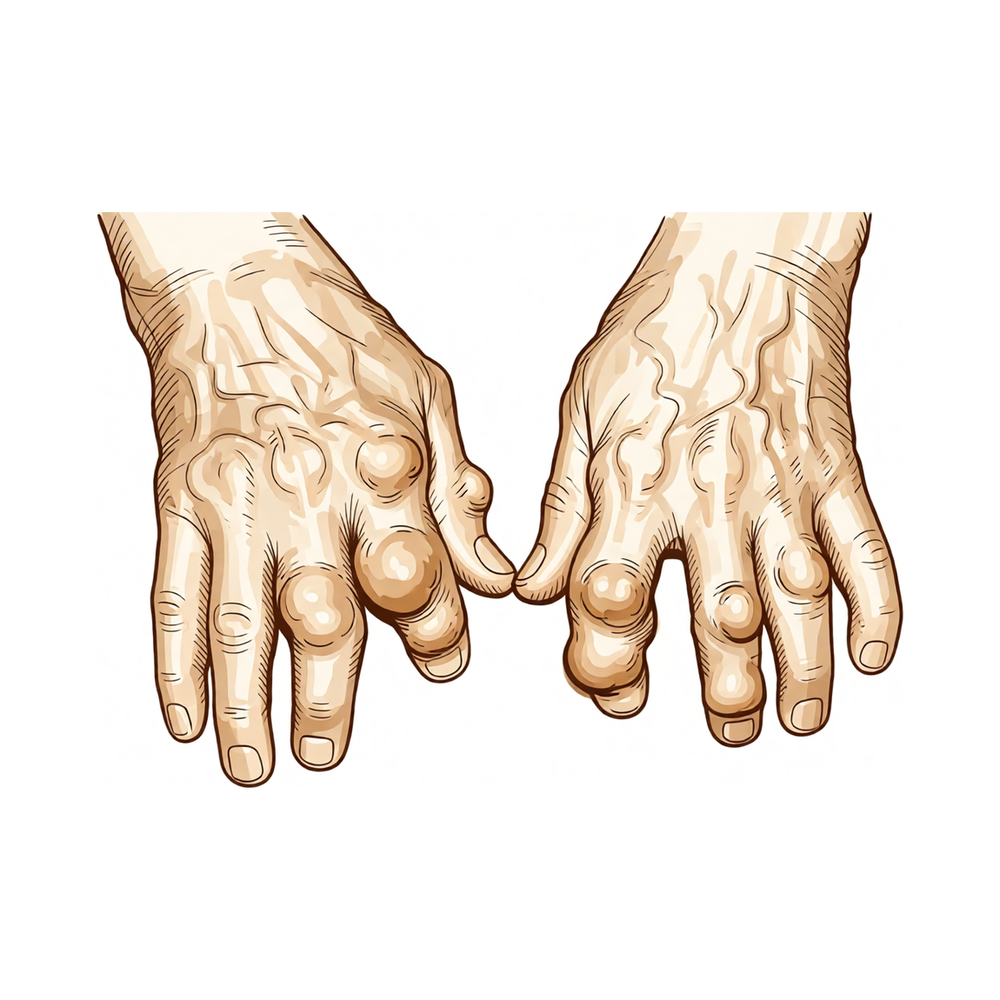
Between flares the joint may feel completely normal, which is why people often dismiss the first attack. Over months and years, though, gout can leave firm lumps under the skin, around the finger joints, the knuckles, or over the elbow. These are called tophi. They can be chalky or white beneath the skin, and as they grow they can make the hand stiff, weaken your grip, and make fine tasks like buttoning a shirt difficult. Some people also notice numbness or tingling in the fingers if a lump presses on a nerve at the wrist.
What's actually happening
Gout is a whole-body problem that shows up in your joints. Your body makes a waste product called uric acid (urate). When there is too much of it in the blood, it can form tiny, sharp crystals that settle inside joints and the soft tissues around them, including in the hand and wrist.
Your immune system treats those crystals as invaders and attacks them, and that reaction is the sudden, severe inflammation you feel as a flare. If the high urate level is left unchecked for years, the crystals build up into the firm deposits (tophi). Over time these deposits can wear away bone, damage tendons, and occasionally press on a nerve. The important point is that the flares and the lumps are two faces of the same thing: too much urate in the body. Control the urate, and you control the disease.
What we can do about it
Treatment has two separate halves, and both matter.
Settling the attack. A flare is calmed with anti-inflammatory medication, usually an anti-inflammatory tablet (an NSAID), colchicine, or a short course of steroids. These work best when started early, so it is worth having a plan agreed with your doctor before the next one strikes.
Lowering the urate for good. This is what actually cures gout over time. A daily tablet, most commonly allopurinol, gradually brings your blood urate down below a target level. Held there long enough, the crystals slowly dissolve, the flares stop, and the tophi shrink. Diet and lifestyle help (less beer and spirits, fewer sugary drinks, staying a healthy weight, good hydration), but for most people the daily tablet does the heavy lifting.
Surgery is only occasionally needed, for a large tophus that is breaking through the skin, interfering with a tendon, or pressing on a nerve (for example causing carpal tunnel symptoms). Even then, the medical treatment to lower urate still has to continue afterwards.
What to expect
Gout is one of the few forms of arthritis we can genuinely get on top of. If your urate is kept below target for the long term, flares become rare and then stop, and existing lumps gradually melt away. It is a slow process: months to years, and the urate-lowering tablet is usually for life, because stopping it lets the crystals reform.
The trade-off for that patience is real: the more tophus builds up in the hand, the more it limits what the hand can do, so getting the urate down early protects your grip and your function. People who stick with treatment do very well.
When to see someone
- A first hot, swollen, painful joint: see a doctor promptly. A joint infection can look identical to gout and is an emergency, so the two need to be told apart.
- Repeated attacks, or attacks that are becoming more frequent: this is the signal to start urate-lowering treatment.
- Lumps appearing around the joints, or a lump that breaks through the skin or leaks chalky material.
- Numbness, tingling or weakness in the hand: a deposit may be pressing on a nerve and is worth assessing.
Advanced reading: the deeper science (optional)
This section steps up to a more detailed, student-level explanation of the biology. It isn't needed to manage gout, but if you're curious about why an attack is so sudden and fierce, and why treatment has two separate jobs, read on.
What gout actually is: urate crystals
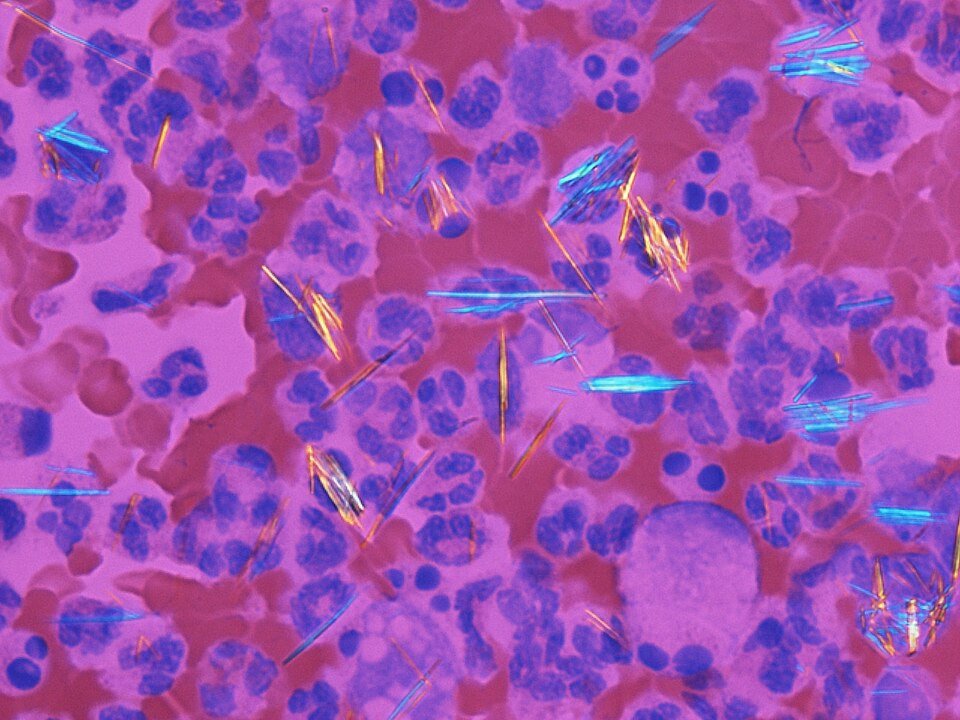
Uric acid is a normal waste product made when the body breaks down substances called purines (from cells and some foods). When the level of urate in the blood stays high, it can come out of solution and form tiny, needle-like monosodium urate (MSU) crystals in and around joints. Crystals form more readily where it is cooler; this is a large part of why the big toe, the body's coolest and most peripheral joint, is the classic first target.
The inflammasome: why an attack is so sudden and fierce
An attack begins when immune scavenger cells (macrophages) engulf MSU crystals. The crystals trip an internal alarm complex called the NLRP3 inflammasome, which switches on an enzyme (caspase-1) that releases a powerful inflammatory messenger, interleukin-1β (IL-1β). IL-1β floods the joint with inflammation, producing the rapid, intense redness, heat, swelling and pain of an acute attack within hours. The same crystals being driven to form by cold explains the night-time, peripheral-joint pattern. Attacks are self-limiting over days as the response burns out.
Why treatment has two separate jobs
- Treating the attack (colchicine, anti-inflammatories, steroids, or, in difficult cases, drugs that block IL-1) calms the inflammation but does nothing to the crystals.
- Long-term treatment (urate-lowering drugs such as allopurinol) lowers blood urate below the level at which crystals form, so existing crystals slowly dissolve and new ones stop forming. This is the actual cure, but it takes months, and can briefly trigger attacks as crystals dissolve, which is why it's started carefully and often with cover.
Tophi and long-term damage
If high urate persists for years, crystals build into chalky lumps called tophi and can erode the bone and cartilage of the joint. Getting urate down and keeping it down is what prevents this permanent damage.





