How Wounds and Scars Heal Info In-depth
Last reviewed
Every cut, graze and surgical incision heals through the same remarkable, predictable sequence, and every one leaves a scar, because healed skin is repaired, not perfectly regrown. Understanding how wounds heal explains why a fresh scar is red and firm before it fades, why a healed wound is never quite as strong as the skin it replaced, and why things like smoking and diabetes matter so much. This page explains, in plain language, how skin mends and scars settle; for the curious, it then goes deeper into the biology of repair and why scars behave as they do.
What a wound is and how skin heals
A wound is simply a break in the skin's protective barrier. Healing it happens in overlapping steps: first the bleeding stops and a clot/scab forms; then the area becomes inflamed (red, warm, a little swollen) as clean-up cells move in; then the body fills the gap with new tissue and pulls the edges together; and finally, over months, that new tissue is reorganised and strengthened into a scar.
A surgically closed incision (edges stitched neatly together) heals faster and with a finer scar than a wound left open to fill in from the bottom up, but both follow the same underlying process.
How scars form and mature
A scar is the patch the body lays down to close a wound. Fresh scars are typically raised, firm, red or pink because they are full of new blood vessels and disorganised collagen. Over the following months to a year, the scar remodels: blood vessels regress and the collagen reorganises, so a mature scar becomes flatter, paler, softer and less noticeable. This is why you should judge a scar at a year, not at a month.
Two honest truths about scars: they never regain the full strength of the original skin (about 80% at best), and how a scar turns out depends partly on you (wound care, not smoking) and partly on factors you can't control (genetics, skin type, where on the body it is, and tension across the wound).
What helps a wound heal well
- Keep it clean and protected, and follow your dressing/wound-care instructions; infection is a major derailer.
- Don't smoke. Nicotine narrows blood vessels and starves the wound of oxygen, one of the strongest controllable risks for wound breakdown.
- Eat well. Adequate protein, vitamin C and zinc, and good blood-sugar control if diabetic, supply the raw materials.
- Protect the scar while it matures: minimise tension, and shield a new scar from the sun (which can darken it permanently) for the first year.
Advanced reading: the deeper science (optional)
This section steps up to a more detailed, student-level explanation. It isn't needed to look after a wound, but if you're curious about how repair actually works and why scars are the way they are, read on.
The four phases of wound healing
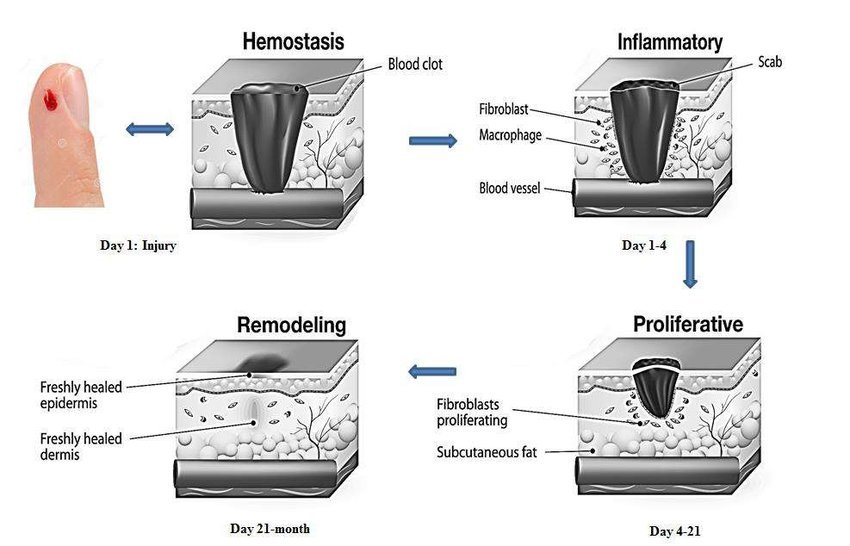
Repair runs through four overlapping phases:
- Haemostasis (minutes). Blood vessels constrict and a clot forms, plugging the wound and laying down a temporary fibrin scaffold.
- Inflammation (days). Immune cells (neutrophils then macrophages) clear bacteria and debris and release signals that summon repair cells. This is the red, swollen, tender phase.
- Proliferation (days to weeks). Fibroblasts pour in and lay down new collagen; new blood vessels sprout (forming pink "granulation tissue"); skin cells migrate across the surface to re-seal it.
- Remodelling (weeks to ~a year). The hasty early collagen is broken down and replaced with stronger, better-organised collagen, blood vessels regress, and the scar matures.
Why scars are weaker than skin
The key is collagen type. Early repair lays down a lot of type III collagen, which is quick to deposit but mechanically weak and disorganised. During remodelling this is gradually replaced by stronger, aligned type I collagen and cross-linked. Tensile strength climbs accordingly: roughly half of normal by six weeks, peaking around 80% by about three months, but never reaching 100%. A scar is also missing the original skin's neat architecture (and its hair follicles and sweat glands). So a healed wound is a strong, serviceable patch, not a perfect replacement.
Myofibroblasts and wound contraction
A specialised repair cell, the myofibroblast, is part fibroblast and part muscle cell: it grips the wound matrix and physically contracts, pulling the edges of the wound together to shrink the area that needs covering. This is helpful; it closes wounds faster. But in the wrong place it causes problems: across a joint or the palm, excessive contraction can pull tissues into a tight contracture that limits movement, which is why wounds and burns over flexion creases are managed so carefully.
When scarring goes wrong: hypertrophic and keloid scars
Sometimes the balance between laying down collagen and breaking it down tips too far toward deposition, giving an overgrown scar:
- A hypertrophic scar is raised and red but stays within the boundary of the original wound, and often improves over time.
- A keloid grows beyond the original wound margins, behaving almost like a benign overgrowth; keloids are commoner in certain skin types and body areas (chest, shoulders, earlobes) and are much harder to treat.
Both reflect an exaggerated, prolonged proliferative response: too much collagen, too little remodelling.
Primary versus secondary healing
Surgeons distinguish two routes. Healing by primary intention is a clean wound with edges held directly together (a sutured incision): fast, with a thin scar. Healing by secondary intention is a wound left open (because of tissue loss or infection) that fills from the base up with granulation tissue and contracts closed: slower, with a broader scar. Choosing between them (and when to close a contaminated wound) is a core surgical judgement.
What helps and harms wound healing
- Blood supply and oxygen are essential, which is exactly what smoking impairs.
- Diabetes, poor nutrition, advanced age, and steroids/immunosuppression all slow healing and raise infection risk.
- Infection stalls a wound in the inflammatory phase and can break a closed wound down.
- Tension and movement across a wound widen the scar; protecting and supporting it produces a finer result.
- Time and sun protection determine the final cosmetic outcome: a scar judged at a year looks far better than at a month.
See also
- How bone heals and remodels — the same repair phases, in bone
- Smoking and musculoskeletal healing — why smoking is so damaging to healing
- How tendons work and heal — repair-by-scar in another tissue





