Acromioclavicular Joint Injury (Shoulder Separation) Info
Last reviewed
Patients › Shoulder
A shoulder separation from a fall on the point of the shoulder — grading, the bump that may remain, and when surgery is needed.
What you're feeling
This injury almost always starts with a fall directly onto the point of the shoulder: coming off a bike, a tackle or heavy contact in sport, or a simple trip onto a hard surface. Straight away the top of the shoulder is sore, and over the next day or two a tender lump or step often appears right at the tip, where your collarbone meets the shoulder.
The area is painful to touch and to lift the arm, and reaching across your body or overhead can be especially uncomfortable. If you press on the lump, it can feel springy, as if pushing down on the end of the collarbone and feeling it bounce back up, a bit like a piano key. Many people instinctively cradle the arm, because letting it hang drags on the sore joint. This is what people mean by a "shoulder separation", and it is not the same as a dislocated shoulder, where the ball of the shoulder pops out of its socket.
What's actually happening
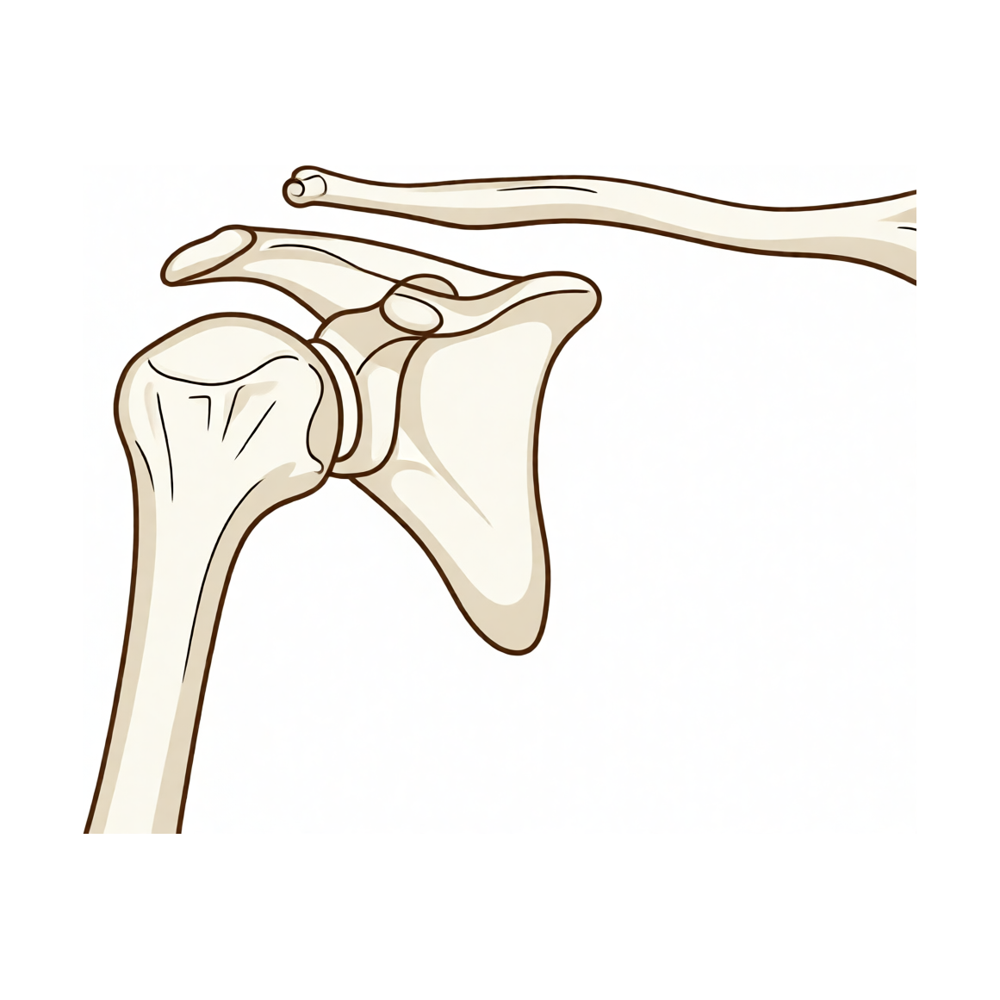
At the very top of your shoulder there is a small joint where the outer end of the collarbone (clavicle) meets a bony tip of the shoulder blade called the acromion. This is the acromioclavicular (AC) joint. It is held together by ligaments, both the ones around the joint itself and a set of strong ligaments a little lower down (the coracoclavicular, or CC, ligaments) that act like guy-ropes anchoring the collarbone down.
A fall onto the point of the shoulder drives the shoulder blade downwards while the collarbone stays put, straining or tearing those ligaments. When only the joint's own ligaments are sprained, the collarbone stays more or less in place. When the stronger guy-rope ligaments tear as well, the collarbone is no longer held down and rides up, which is what creates the visible bump and step.
Surgeons grade these injuries by how much damage there is, using a scale called the Rockwood classification, I to VI. Grades I and II are sprains with little or no displacement; grade III sits in between, with a noticeable bump but the shoulder still working reasonably well; and grades IV to VI are the high-grade injuries, where the collarbone is badly out of position. It is worth knowing this is a different problem from a worn-out, arthritic AC joint (wear-and-tear over years) and from a broken collarbone (both of which we cover separately).
What we can do about it
The good news is that most AC joint injuries do not need surgery.
Low-grade injuries (grades I, II and most grade III) are treated simply. A sling for comfort for a couple of weeks takes the drag off the joint and lets the irritation settle. Once the early pain eases, physiotherapy restores movement and rebuilds the muscles around the shoulder blade and shoulder. People generally regain good, often full, function and get back to work and sport. The one honest caveat is cosmetic: even after everything heals, the bump at the top of the shoulder often stays for good. It looks different from the other side, but it usually does not stop the shoulder working.
Surgery is reserved for the injuries that need it. That means the high-grade injuries (grades IV, V and VI), where the collarbone is badly displaced, and the smaller group of lower-grade injuries that stay painful, weak or unstable despite proper rehab, particularly in people who do heavy manual or overhead work, or in serious athletes. An operation reconstructs the torn ligaments to pull the collarbone back down into its proper position and hold it while it heals. We talk through that separately under the AC joint stabilisation procedure.
What to expect
For the great majority of people with a low-grade injury, the story is reassuring. The sharp pain settles within a few weeks, and with physiotherapy the shoulder steadily regains its strength and range. Most return to their normal activities and sport, accepting that the bump may be a permanent reminder of the injury without limiting what the shoulder can do. Even some grade III injuries that look dramatic at first do well without surgery.
The injuries that take longer are the high-grade ones, and the low-grade ones that simply don't settle. Here the question is whether reconstruction will give a more stable, stronger, less painful shoulder for the demands you place on it, and the answer depends a lot on your work, your sport and how the shoulder is behaving over the first weeks. There is good evidence that this decision is best made unhurried, giving the shoulder a fair trial before committing to surgery, while not leaving a clearly unstable, high-grade injury indefinitely.
When to see someone
- A fall onto the point of the shoulder that leaves it painful, with a tender lump or step at the top, worth having assessed, both to grade the injury and to rule out a broken collarbone.
- An obvious, prominent bump with the arm feeling like it is dragging down: this suggests a higher-grade injury that needs proper assessment.
- Pain or weakness that isn't settling after a few weeks of a sling and physiotherapy, especially if you do heavy or overhead work or play sport.
- Skin under tension over the bump, a change in skin colour over it, or any sense the bone is pushing hard against the skin: get this looked at sooner.





