How Pain Works Info In-depth
Last reviewed
Pain is the body's alarm system. It protects you by making you stop, withdraw and rest while something heals, and in the short term it is one of the most useful things the nervous system does. But pain is more complicated than a simple "damage meter." Understanding it genuinely helps, especially when pain lingers: the alarm system itself can become oversensitive, so that pain continues, or is felt out of all proportion to what's found on a scan, even after the tissues have healed. A central, evidence-based message runs through this page: hurt does not always equal harm. This page explains, in plain language, what pain is and how it works, then goes deeper for the curious into the biology of why pain can persist.
What pain is and what it's for
Pain is not measured by a sensor and piped unchanged to the brain like a thermometer reading. It is an output the brain produces after weighing many inputs: signals from the body, yes, but also context, past experience, mood, and how threatening the brain judges the situation to be. Its purpose is protection, to grab your attention and change your behaviour so an injury can heal.
This is why the same injury can hurt very differently on different days or in different people, and why pain is completely real even when it doesn't match what's visible on an X-ray.
Acute versus chronic pain
- Acute pain is the normal alarm: it comes with an injury, it is roughly proportional to the damage, and it settles as healing happens. This pain is doing its job.
- Chronic pain is pain that persists beyond the expected healing time (usually defined as more than about three months). Here the problem is often not ongoing tissue damage but an alarm system that has become over-sensitive and won't switch off. The pain is real and can be severe, but it is no longer a reliable signal that something is being harmed.
That distinction matters enormously, because the two need different approaches: acute pain is managed by treating the injury and providing short-term relief; chronic pain is managed by gradually calming and retraining the nervous system, not by chasing ever-stronger painkillers.
What helps with pain
- Understanding it. Learning that "hurt does not equal harm" genuinely reduces chronic pain and disability; fear and catastrophising amplify pain.
- Movement and pacing. Gentle, graded activity desensitises an over-sensitive system; prolonged rest and avoidance usually make chronic pain worse.
- Sleep, mood and stress. Poor sleep, low mood and stress all turn the pain volume up; addressing them turns it down.
- The right medicines for the right pain. Short courses of simple analgesics help acute pain; chronic pain responds better to nerve-targeted medicines, exercise and psychological strategies than to opioids.
Advanced reading: the deeper science (optional)
This section steps up to a more detailed, student-level explanation. It isn't needed to manage your pain, but if you're curious about how pain is generated and why it can persist, read on.
How a pain signal travels
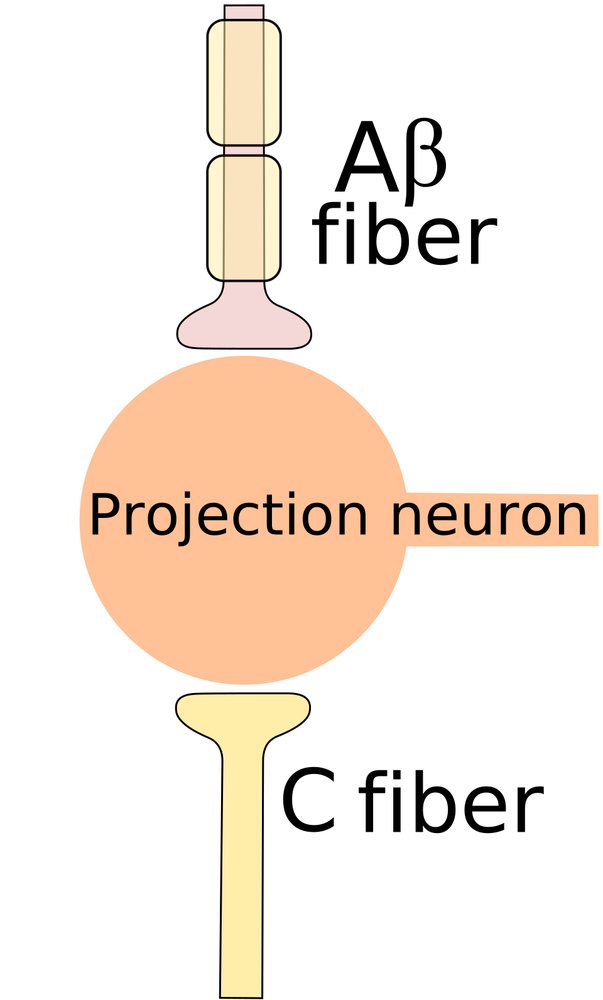
Specialised nerve endings called nociceptors detect potentially damaging stimuli: extreme pressure, heat, or chemicals released by injured tissue. They send signals up two kinds of fibre. Fast, insulated A-delta fibres carry the sharp, immediate "ouch" that makes you snatch your hand back; slower, bare C fibres carry the dull, aching, lingering pain that follows. These signals reach the spinal cord, where they are relayed (and already modulated) before travelling up to the brain. There is no single "pain centre"; many brain regions together decide whether to produce pain, and how much. So pain is constructed, not simply received.
The gate control idea
The spinal cord acts like a gate that can turn incoming pain signals up or down. Non-painful input can "close the gate" on pain, which is why rubbing a knock, or a TENS machine, eases it. The brain also sends signals downward to the spinal cord that dial pain up or down depending on attention, mood and context (descending modulation). This is the real mechanism behind everyday observations: a sports injury barely felt mid-game, pain that worsens when you're anxious or exhausted, relief from distraction or reassurance. The gate is not metaphorical; it is physiology.
Peripheral and central sensitisation
After an injury the system deliberately turns up its own gain so you protect the area:
- Peripheral sensitisation: chemicals released at the injury make local nociceptors more excitable, so the sore area hurts more (this is why sunburnt skin screams at a warm shower).
- Central sensitisation: the spinal cord and brain themselves become more excitable, amplifying every incoming signal.
The hallmarks are hyperalgesia (painful things hurt more than they should) and allodynia (things that shouldn't hurt at all, such as light touch or clothing, become painful). In acute injury this is useful and reverses. In chronic pain it can persist and self-sustain.
When pain outlasts the injury: chronic and nociplastic pain
In some people the nervous system stays sensitised long after the tissues have healed; the alarm is stuck "on." Pain that arises from this altered processing, rather than from ongoing damage or nerve injury, is called nociplastic pain (central sensitisation is its main mechanism). It explains a common and once-baffling clinical picture: severe, genuine, disabling pain with little or nothing to find on imaging. Recognising this is not dismissing the pain as "in your head"; the changes are real, measurable nervous-system changes. It reframes the goal: not to hunt for more structural damage to fix, but to down-regulate an over-sensitive system. Conditions like fibromyalgia, and much persistent musculoskeletal pain, sit here.
Why stronger painkillers aren't the answer for chronic pain
Opioids are useful for short-term, severe acute pain, but they are a poor fit for chronic pain. With ongoing use the body develops tolerance (needing more for the same effect) and, paradoxically, opioid-induced hyperalgesia: the drugs can make the nervous system more pain-sensitive over time. Because chronic pain is largely a sensitised-system problem, the effective tools are the ones that retrain that system: graded exercise, sleep, psychological strategies, and nerve-targeted (rather than opioid) medicines.
What helps and harms
- Graded activity and pacing desensitise the system; fear-driven avoidance and prolonged rest sensitise it further.
- Sleep, mood, and stress management lower the gain; poor sleep and distress raise it.
- Education and reducing catastrophising measurably reduce pain and disability.
- Right medicine for the right pain: short-term simple analgesia for acute pain; exercise, psychological therapy and nerve-targeted drugs (not escalating opioids) for chronic pain.
See also
- How nerves work and heal — the wiring that carries pain signals
- Nerve pain medicines — the medicines used for nerve-related and sensitised pain
- Managing pain and opioids after surgery — short-term pain control done well





