MCP Joint Replacement Info Evidence
Reviewed by Dr Kieran Hirpara, Specialist Orthopaedic Surgeon Last reviewed
This protocol guides your recovery after silicone (Swanson) replacement of the knuckle joints (the metacarpophalangeal or "MCP" joints) with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It begins with your home exercise program, followed by the structured clinical protocol written for your hand therapist: bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your hand therapist may adjust the plan depending on how your recovery progresses.
This is a hand-therapy-intensive, splint-driven recovery. The dynamic splint and your daily exercises are not optional extras: they are how the new joints are shaped into a corrected, straight position. Your result depends heavily on doing the splinting and movement faithfully.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect
The knuckle joints can become worn, painful and badly deformed, most often in rheumatoid arthritis, where the fingers drift towards the little-finger side (ulnar drift) and the bases of the fingers slip down towards the palm (volar subluxation); they can also wear out from osteoarthritis. In this operation the worn knuckle joint is removed and replaced with a flexible silicone spacer (the classic Swanson implant). The aims are to relieve pain, correct the drift and the droopy knuckles (extensor lag), and restore a useful arc of bending.
The implant is not a rigid hinge. It works as a flexible spacer while a new lining (a "capsule") forms around it over the first weeks, and the whole point of the rehabilitation is to make that capsule form with your fingers held straight and corrected, not drifted. That is why the splint and the early movement matter so much.
The recovery is therefore built around a dynamic extension outrigger splint, usually fitted within the first few days:
- At rest, the splint holds your knuckles straight and pulled gently towards the thumb side (radial deviation), directly opposing the old ulnar drift.
- Within the splint you do early controlled active bending of the knuckles against soft elastic loops, which spring the fingers back out straight. Moving early (but only in this protected, corrected position) shapes the new capsule correctly and keeps the joints from stiffening.
You wear the dynamic splint almost continuously for about six weeks, then wean to a resting / night splint, with graded strengthening added later. Light hand function returns over the first weeks; most people are back to most everyday activities by around three months, with the final result continuing to settle over several more months.
Precautions and limitations
- Wear your dynamic extension splint as directed: day and night for about the first six weeks. It holds the correction; taking it off too much lets the drift come back.
- Do NOT let your fingers drift back towards the little-finger side. Every exercise guides them the other way, towards the thumb.
- Do NOT do any strong gripping, pinching or heavy lifting early: hard grip pushes the fingers into ulnar drift and stresses the new joints before they are stable. Strengthening waits until your hand therapist clears it.
- Keep your thumb, wrist and the tips of your fingers moving from the start, and use the hand for light everyday tasks within comfort.
- Watch the wound for signs of infection (increasing redness, heat, swelling or discharge) and contact the rooms if you are concerned; infection around an implant is uncommon but important to catch early.
For wound, swelling and scar management, see the practice's wound care guidance.
Your exercises
Kieran Hirpara 4.0
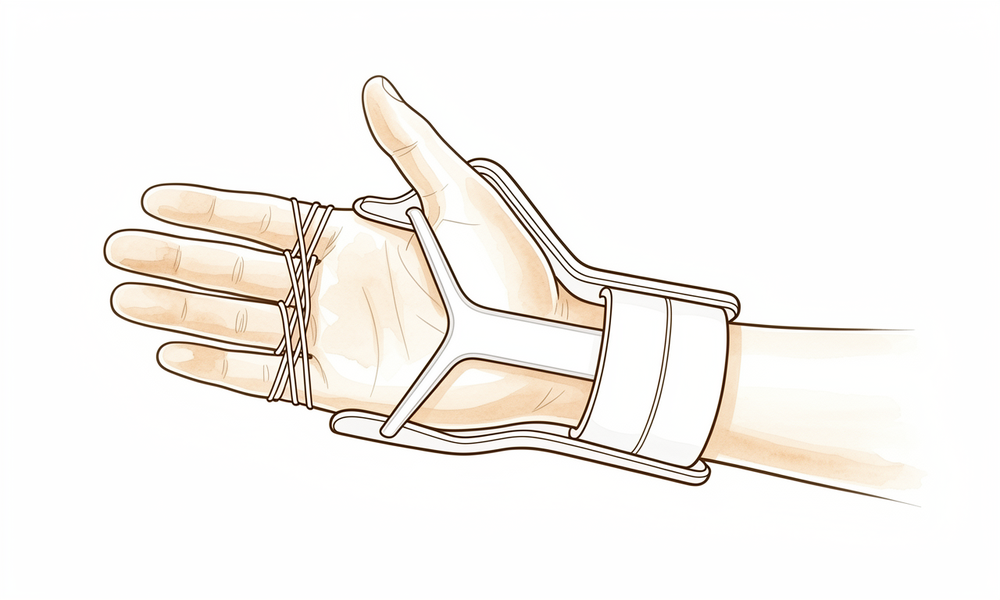
Wearing your dynamic splint
Your dynamic extension splint does the protecting for you: at rest it holds your knuckles straight and pulled gently towards the thumb side (radial), correcting the old drift. Wear it as directed — day and night for about the first six weeks — taking it off only for washing and for the exercises your hand therapist allows out of the splint. The loops on your fingers should sit comfortably; tell your therapist if anything rubs or pinches.
Worn continuously for ~6 weeks, then nights/rest as guided
Kieran Hirpara 4.0
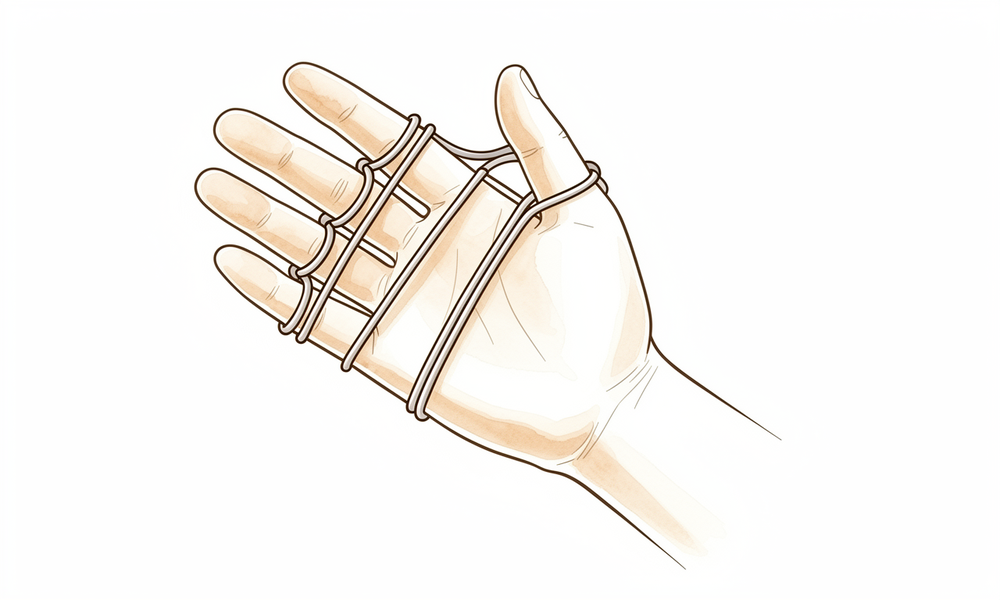
Controlled knuckle bending in the splint
While wearing the splint, gently bend your fingers down at the knuckles, pulling against the elastic loops, then relax and let the splint spring them back out straight. This early controlled movement is what shapes the healing capsule around the new joints in a good position. Move smoothly and stop short of pain — you are guiding the joint, not forcing it.
10 bends each hour you are awake, within the splint, as guided
Kieran Hirpara 4.0
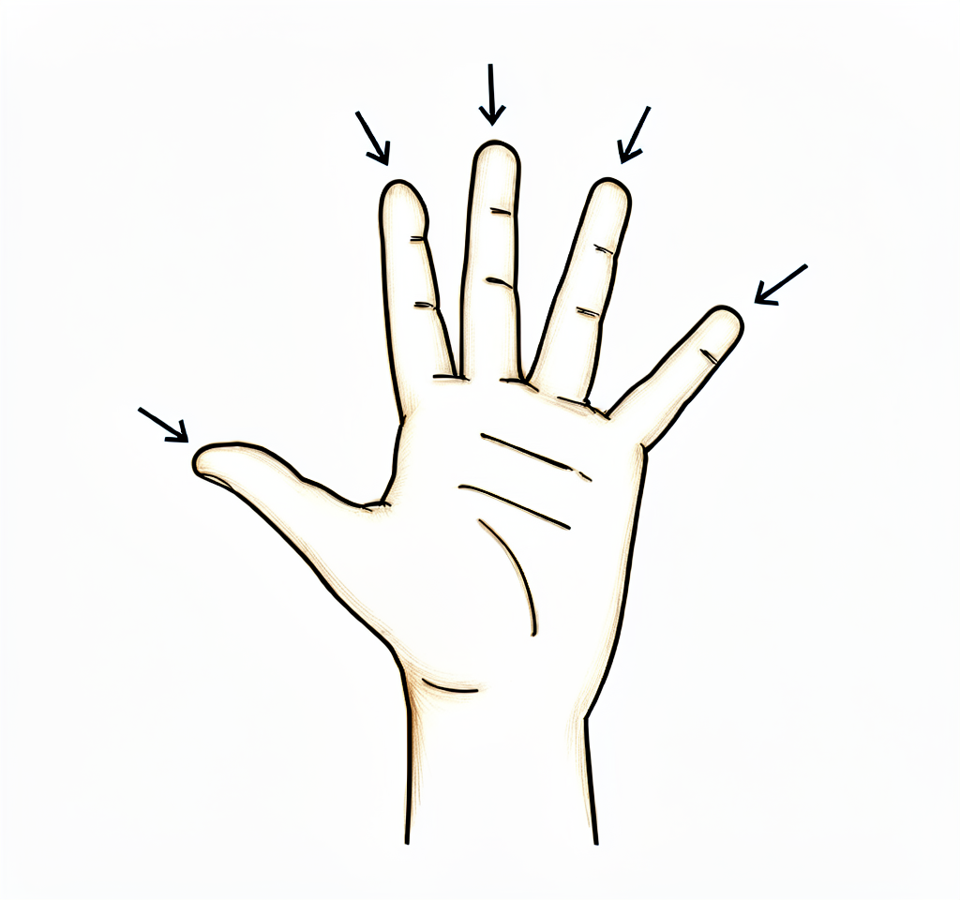
Active straightening (lifting the knuckles)
Work on fully straightening your knuckles under your own power — lift the fingers up level. After surgery the knuckles can tend to droop (an extensor lag), so actively lifting them keeps the straightening tendons gliding and helps hold the correction. Your therapist will start this within the splint, then progress it out of the splint.
10 lifts, several times a day, as guided
Kieran Hirpara 4.0
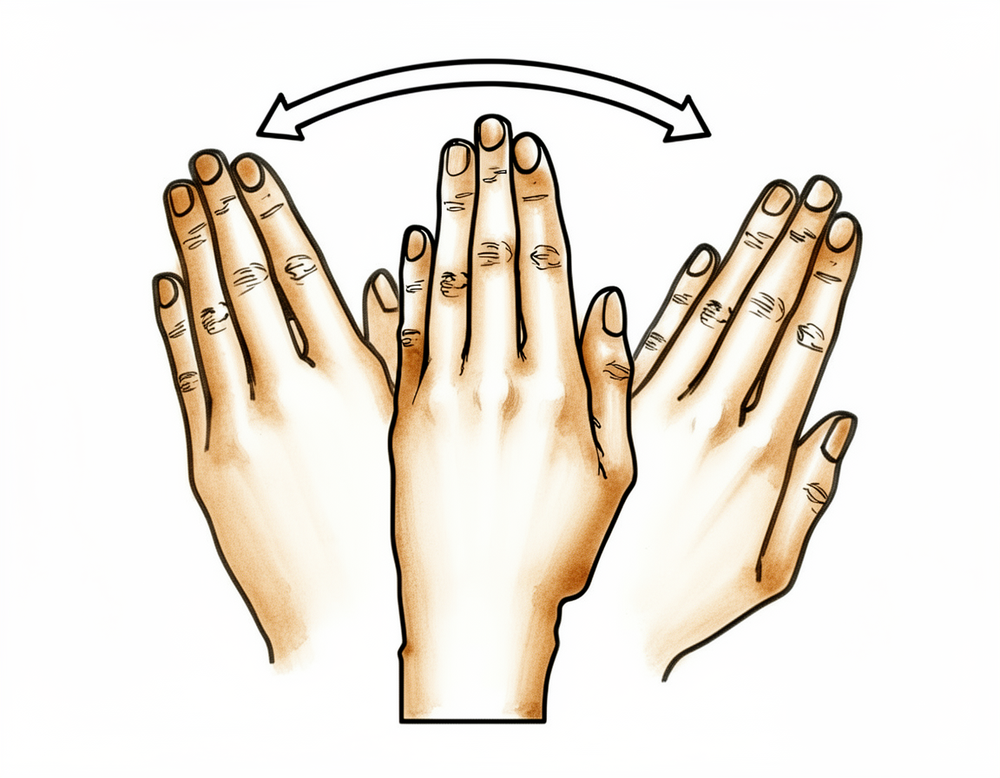
Finger walking towards the thumb (radial)
Gently guide your fingers across towards your thumb (the radial direction) — the opposite way to the old drift. You can help with your other hand or walk the fingertips along a tabletop towards the thumb. This re-trains the fingers to line up straight and is the key correction this whole protocol is built around. Never let them drift back the other way.
10 times, several times a day, as guided
Kieran Hirpara 4.0
Scar care
Once your wounds are fully healed and your therapist says it is safe, massage the scars over the back of your hand with a little plain cream, using small firm circles for a few minutes. This keeps the scars soft and stops the skin sticking down over the tendons, so the knuckles move more freely.
A few minutes, 2-3 times a day, once healed

Kieran Hirpara 4.0
Grip strengthening (later)
A LATER exercise — only once your hand therapist clears strengthening, usually from around eight to twelve weeks. Gently squeeze a soft ball or therapy putty, then release. Build it up slowly. This is held back early because hard gripping pushes the fingers towards ulnar drift and stresses the new joints before the capsule is strong — so it is always the last thing to start.
As guided by your hand therapist (from ~8-12 weeks only)
These are the exercises from your handout. Start them only as guided by Dr Hirpara and your hand therapist, staying within whatever range and limits you have been given. The early work is all done with the dynamic splint on: controlled bending against the loops, active straightening, and gently walking the fingers towards the thumb to hold the correction. Scar care begins once the wounds have healed, and grip strengthening belongs to a later phase and should not be started until you are specifically cleared. Stop anything that causes sharp pain in the knuckles.
Your clinical protocol
The rest of this page is the staged clinical protocol for rehabilitation after silicone (Swanson) MCP joint arthroplasty. This section is to be provided to your hand therapist, and each phase opens with a plain-English explanation of what is happening. The defining principle is that the new MCP capsule remodels around the implant in whatever position you hold it, so the splint and exercises hold the joints in extension with slight radial deviation while permitting early controlled active flexion, re-shaping the joints in a corrected position and reversing the ulnar drift.
Prior to treatment, check the patient's operation report and past medical history, and liaise with the treating surgeon regarding the diagnosis (rheumatoid vs osteoarthritis), the soft-tissue reconstruction performed (radial collateral ligament reefing, ulnar intrinsic release, extensor centralisation / crossed-intrinsic transfer), and the achieved intra-operative correction and arc. The rheumatoid hand drifts and recurs more readily than the osteoarthritic hand and warrants particularly diligent radial-deviation splinting. The protocol below assumes the standard dynamic-extension-outrigger regime.
Phase I — dynamic extension splint with early controlled motion (weeks 0 to ~6)
The first six weeks are the decisive window: the capsule forms around the implant now, and the dynamic splint dictates the position it forms in. Fit a forearm-based dynamic MCP extension outrigger splint, typically within the first 3-5 days. At rest it holds the MCPs in full extension with the proximal phalanges pulled into slight radial deviation (correcting the old ulnar drift); the outrigger slings sit on the proximal phalanges and the elastic tension permits controlled active flexion, then returns the digits to extension. The patient performs early controlled active MCP flexion within the splint every waking hour. The wrist and IP joints are left free.
For your hand therapist:
Education and precautions - Fit and tension the dynamic extension outrigger splint: MCPs held in extension + slight radial deviation, slings on the proximal phalanges, radial pull to counter ulnar drift - Worn continuously (day and night) for ~6 weeks, off only for hygiene and supervised exercise - No strong grip, pinch or lateral (ulnar-directed) loading: these recreate the deforming forces - Protect any soft-tissue reconstruction (radial collateral / intrinsic balancing): avoid forced ulnar-deviating stress at all times - Keep the thumb, wrist and IP joints mobile; light unloaded hand use only
Management - Wound: surgical dressings as directed; monitor for infection (implant present) - Oedema: elevation, gentle retrograde massage, light compression as tolerated - Exercises: controlled active MCP flexion within the splint against the loops, aiming to develop a useful flexion arc (target the surgeon's intra-operative arc, commonly up to ~70 degrees at the index-to-little MCPs) with full passive return to extension via the outrigger; active MCP extension (correct extensor lag); radial-deviation re-education (guide digits towards the thumb); free IP and wrist ROM
Criteria to progress - Wound healed; settling oedema; emerging active flexion arc with maintained extension and corrected (radial) alignment at around six weeks
Phase II — weaning the splint and consolidating correction (weeks ~6 to ~12)
From about six weeks the capsule is maturing and the dynamic splint is weaned to a resting / night extension splint (often continued to ~12 weeks, and at night longer in rheumatoid hands prone to recurrence). Out-of-splint active motion is progressed, always biased towards extension and radial alignment. Light functional use expands; heavy grip and pinch remain withheld.
For your hand therapist:
Assessments - Active and passive MCP flexion/extension arc; extensor lag; ulnar-deviation (compare with intra-operative correction); pain and swelling; wound/scar review
Education and precautions - Wean the dynamic splint; continue a night / resting extension splint to ~12 weeks (longer at night in rheumatoid patients) - Continue to avoid strong grip/pinch and any ulnar-deviating load - Vigilantly preserve the radial correction; recurrence of drift is the principal late failure
Management - Exercises: progress active and gentle active-assisted MCP flexion/extension out of the splint; ongoing extensor-lag work and radial-deviation re-education; commence scar management once healed; light functional tasks within comfort, kept off the ulnar-deviating patterns
Criteria to progress - Stable correction (minimal recurrent ulnar deviation, acceptable extensor lag) on a maturing capsule; comfortable functional arc; pain settling
Phase III — strengthening and return (weeks ~12 and beyond)
Once the capsule is robust and alignment is holding (around twelve weeks), graded strengthening is introduced, late and cautiously, because grip drives ulnar drift. Strength and the final functional result continue to improve over several more months.
For your hand therapist:
Assessments - Grip/pinch versus the other side and versus pre-operative; maintained arc, extension and alignment under load; functional and task-specific testing
Education and precautions - Begin graded grip/strengthening from around 8-12 weeks only, building load gradually - Coach grip patterns that do not drive ulnar deviation; ongoing night splinting as indicated, especially in rheumatoid hands - Set realistic expectations: the aim is pain relief, a corrected position and a functional arc rather than a normal or powerful hand
Management - Exercises: progressive putty/ball grip and pinch, isometric MCP control, functional strengthening; continue mobility and any residual extensor-lag/alignment work - Consider discharge once correction is stable, a useful arc is achieved and the patient manages daily function; provide a long-term night-splint and joint-protection plan - Refer back to the treating doctor if alignment deteriorates, the arc is lost, or implant problems are suspected
Criteria for discharge - Stable corrected alignment, functional pain-free arc, adequate functional grip, sound joint-protection and night-splint routine
Getting back to work and activity
Light everyday hand use (eating, writing, light self-care) is encouraged from the start within comfort, as long as it avoids strong gripping, pinching and any sideways (ulnar) stress on the fingers. Plan for the dynamic splint to be on almost all the time for the first six weeks, which limits two-handed and heavy tasks; arrange help accordingly. Driving resumes once you can safely control the car and are out of the dynamic splint for driving (typically around six weeks), as confirmed at your review.
Strengthening and heavier hand use wait until about twelve weeks and are then built up gradually under your hand therapist's guidance. Most people return to most everyday activities by around three months, with the final result (comfort, alignment and a useful arc) continuing to settle over several more months. Progression is judged by Dr Hirpara and your hand therapist on how your hand is correcting and functioning, not by the calendar alone. Heavier or repetitive manual work follows the same criterion-based progression, with joint-protection advice to keep the correction long-term.
After your protocol
This protocol works alongside the practice's general recovery advice: see managing post-operative pain, wound care and scar management. The phased plan above reflects the long-standing Swanson-style rehabilitation regime after silicone MCP arthroplasty, and your ongoing recovery is guided individually by Dr Hirpara and your hand therapist according to how your hand corrects and progresses.
Evidence & references
Topic scope: post-operative rehabilitation after silicone (Swanson) replacement of the metacarpophalangeal (MCP) joints — flexible silicone-elastomer spacer arthroplasty of the knuckle joints, most often for the rheumatoid hand with ulnar drift and volar subluxation, and less commonly for MCP osteoarthritis. This is a resection-replacement with soft-tissue rebalancing, not a simple decompression: the deforming forces that destroyed the joint (ulnar drift, extensor subluxation, intrinsic tightness) are still present, so the rehabilitation is an active, splint-driven re-shaping programme, not a rest-and-protect pathway.
Defining principle of the rehab here: a silicone MCP implant is a flexible spacer around which a new fibrous capsule ("encapsulation") forms over the first weeks — and that capsule remodels in whatever position the hand is held. The classic post-operative regime therefore uses a dynamic extension outrigger splint that holds the MCPs in extension with slight radial deviation (opposing the ulnar drift) while permitting early controlled active flexion against elastic loops. Move early, but only in the corrected position: this is what reverses the drift and builds a functional flexion arc. The single biggest branch point is the diagnosis — the rheumatoid hand drifts and recurs far more readily than the osteoarthritic hand and warrants more diligent, more prolonged radial-deviation splinting.
A. PROCEDURE OUTCOMES (rheumatoid and osteoarthritis)
Silicone MCP arthroplasty is a deformity-correcting, pain-relieving operation rather than a motion- or strength-restoring one. Its great strength is reliable correction of alignment and relief of pain; its accepted limitations are a modest final arc, gradual implant fracture over years, and—in rheumatoid hands—a tendency to recurrent drift.
- In rheumatoid arthritis it produces durable improvement in deformity, appearance and patient-reported function. The multicentre prospective SARA (Silicone Arthroplasty in Rheumatoid Arthritis) cohort compared 70 surgical with 93 non-surgical RA patients with severe MCP deformity: the surgical group showed significant, sustained gains in the Michigan Hand Outcomes Questionnaire and in ulnar deviation, extensor lag and arc of motion, maintained at 1 year, at long-term (3-year) follow-up, and out to 7 years, whereas the non-surgical cohort did not improve [Chung 2009; Chung 2012; Chung 2017]. Moderate–strong (prospective comparative cohort; not randomised).
- Correction of ulnar drift and extensor lag is the headline result; arc and grip gains are modest. Series consistently report large reductions in ulnar deviation and extensor lag with a re-centred, more functional arc (commonly a final arc on the order of ~40–50° centred nearer extension), with grip strength only modestly changed. The operation buys alignment, pain relief and hand appearance/function, not power [Goldfarb & Dovan 2006; Rizzo 2011; Kirschenbaum 1993]. Moderate.
- For MCP osteoarthritis, long-term results are favourable and durable. A long-term series of silicone MCP arthroplasty for OA reported lasting pain relief and satisfactory function, with better-preserved bone stock and less recurrent deforming force than the rheumatoid hand [Morrell & Weiss 2018]. Moderate.
- Implant fracture accrues with time but is often clinically silent. Long-term radiographic follow-up shows implant fracture rates rising over the years, yet many fractured implants remain asymptomatic and revision is driven by symptoms/instability rather than radiographic fracture alone [Koenuma 2024; Kirschenbaum 1993]. Moderate.
- Revision is uncommon but defined, most often for recurrent deformity, implant fracture/instability or infection; revision MCP arthroplasty is feasible but technically demanding with poorer results than primary surgery [Wagner 2019; Carlson Strother 2023]. Moderate.
B. REHABILITATION / THERAPY EVIDENCE
The central rehab questions are (1) which splint regime, and (2) does adding continuous passive motion or particular splint variants change the outcome. The evidence base is dominated by a strong heritage regime (Swanson-style dynamic extension splinting) supported mostly by expert consensus and low-level studies, with the few controlled comparisons failing to show benefit from add-ons. The rehabilitation is nonetheless indispensable — it is integral to the operation, not an optional adjunct.
- The standard regime is a dynamic extension outrigger splint with early controlled motion. Fitted within the first few days, it holds the MCPs in extension and slight radial deviation at rest and permits active flexion against finger slings, worn essentially continuously for ~6 weeks then weaned to night/rest splinting. The shared aim across published regimes is to encourage MCP flexion and extension without recurrence of flexion contracture or ulnar deviation while the capsule encapsulates the implant in a corrected position [Goldfarb & Dovan 2006; Massy-Westropp Cochrane 2008]. Consensus / heritage — widely practised, low-level evidence.
- Adding continuous passive motion (CPM) to dynamic splinting does not help. The Cochrane review identified a single small controlled trial (22 participants) comparing dynamic splinting ± CPM and concluded CPM is not effective at increasing motion or strength after MCP arthroplasty (controls actually gained more motion); it rated the evidence "silver level" and called for well-designed RCTs given wide practice variation [Massy-Westropp Cochrane 2008]. Moderate (Cochrane SR of low-certainty primary evidence).
- A static-splint alternative achieves comparable correction in small studies. A prospective series using alternating static flexion/extension splints (rather than a dynamic outrigger) reported improved total active arc (21.6°→47.2°) and corrected ulnar deviation (30.4°→9.7°), suggesting the position held and active motion matter more than the specific splint mechanism [Burr/Massy-Westropp J Hand Ther 2002]. Weak (small prospective cohort).
- The specific dynamic-splint protocol has not been shown superior to simpler regimes in controlled comparison. A randomised study found no clear added value of dynamic splinting over a simpler post-operative regime for MCP replacement, reinforcing that the dynamic outrigger is a sound, traditional default rather than a proven optimum [Delaney 2003]. Weak–moderate (small RCT).
Recovery trajectory (expected, evidence-anchored)
| Phase | Window | Splint / position | Hand-therapist focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Dynamic extension splint + early controlled motion | Week 0–~6 | Dynamic extension outrigger worn day & night; MCPs in extension + slight radial deviation | Controlled active MCP flexion within the splint (toward the surgeon's arc, often up to ~70°); active extension (correct extensor lag); radial-deviation re-education; free IP/wrist; oedema control | Light unloaded use only; no grip/pinch, no ulnar load | Capsule forms now — position held = position kept. Rheumatoid hands need the most diligent radial pull |
| II — Wean to night/rest splint, consolidate correction | Week ~6–12 | Wean dynamic splint → night/resting extension splint (longer at night in RA) | Progress active/active-assisted flexion–extension out of splint, biased to extension + radial; scar massage once healed; preserve correction | Still no strong grip/pinch; light functional tasks | Recurrent ulnar drift is the main late failure — guard alignment |
| III — Strengthening & return | Week ~12+ | Night splint as indicated (esp. RA) | Graded putty/ball grip and pinch, isometric MCP control, functional/task strengthening | Begin grip strengthening ~8–12 wk, build gradually; coach non-ulnar-deviating grip | Most everyday activity by ~3 months; alignment/comfort/arc settle over several more months |
(Phase windows mirror the patient protocol; they are typical, heritage-based guides — not trial-derived deadlines.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY
- Heritage regime, modest evidence. The Swanson-style dynamic extension outrigger with early controlled motion is deeply established and near-universally taught, but its supporting evidence is largely expert consensus and small/low-level studies. The defensible position is to follow the heritage regime faithfully while acknowledging its evidence tier [Goldfarb & Dovan 2006; Massy-Westropp Cochrane 2008]. Consensus.
- Which splint? Dynamic outrigger vs alternating static splints vs simpler regimes give broadly similar correction in small studies; CPM adds nothing. What matters is holding the MCPs in extension + radial deviation while moving early — the mechanism of the splint is secondary [Massy-Westropp Cochrane 2008; Burr 2002; Delaney 2003]. Weak–moderate.
- Rheumatoid vs osteoarthritis. The rheumatoid hand has ongoing deforming forces (tendon subluxation, intrinsic tightness, soft-tissue laxity) and recurs, demanding more prolonged radial-deviation/night splinting and joint protection; the osteoarthritic hand has better bone and soft tissue and a more durable correction [Morrell & Weiss 2018; Rizzo 2011]. Moderate.
- Realistic goals. The operation reliably delivers pain relief, corrected alignment and a functional arc, not a normal or powerful hand. Mis-set expectations (large grip gains) are a common source of dissatisfaction [Chung patient-expectations 2015; SARA cohort]. Moderate.
- Implant fracture ≠ failure. Radiographic implant fracture accrues over years but is frequently asymptomatic; revision is symptom-driven. Counsel accordingly rather than revising on imaging alone [Koenuma 2024; Wagner 2019]. Moderate.
D. EVIDENCE STRENGTH FLAGS (summary)
- MODERATE–STRONG: silicone MCP arthroplasty improves deformity, alignment (ulnar deviation, extensor lag), MHQ and arc versus non-surgical care in severe rheumatoid MCP disease, durable to 7 years (SARA prospective cohort — comparative, not randomised).
- MODERATE: correction-over-power outcome profile; favourable long-term OA results; time-related implant fracture (often asymptomatic); defined but uncommon revision rate; greater recurrence in rheumatoid than osteoarthritic hands.
- WEAK / CONSENSUS / HERITAGE: the specific dynamic-extension-outrigger + early-controlled- flexion + radial-deviation rehabilitation programme (strong heritage, low-level evidence; CPM shown unhelpful; dynamic vs static vs simpler regimes not clearly differentiated); exact phase timings (typical, not trial-derived).
CITATIONS
RAG corpus (180,000+ Orthopaedic articles)
- Kirschenbaum D, Schneider LH, Adams DC, et al. Arthroplasty of the metacarpophalangeal joints with use of silicone-rubber implants in patients who have rheumatoid arthritis. Long-term results. J Bone Joint Surg Am. 1993;75(1):3-12. DOI: 10.2106/00004623-199301000-00002
- Goldfarb CA, Dovan TT. Rheumatoid arthritis: silicone metacarpophalangeal joint arthroplasty indications, technique, and outcomes. Hand Clin. 2006;22(2):177-188. DOI: 10.1016/j.hcl.2006.02.001
- Rizzo M. Metacarpophalangeal joint arthritis. J Hand Surg Am. 2011;36(2):345-353. DOI: 10.1016/j.jhsa.2010.11.035
- Morrell NT, Weiss AC. Silicone metacarpophalangeal arthroplasty for osteoarthritis: long-term results. J Hand Surg Am. 2018;43(3):229-233. DOI: 10.1016/j.jhsa.2017.10.010
- Koenuma N, Ikari K, Oh K, et al. Long-term implant fracture rates following silicone metacarpophalangeal joint arthroplasty in rheumatoid arthritis. J Hand Surg Am. 2024. DOI: 10.1016/j.jhsa.2024.01.009
- Wagner ER, Houdek MT, Packard B, et al. Revision metacarpophalangeal arthroplasty: a longitudinal study of 128 cases. J Am Acad Orthop Surg. 2019. DOI: 10.5435/JAAOS-D-17-00042
- Carlson Strother CR, Moran SL, Rizzo M. Small joint arthroplasty of the hand: an update on indications, outcomes, and complications. J Am Acad Orthop Surg. 2023;31(15):e739-e749. DOI: 10.5435/JAAOS-D-23-00034
- Blazar PE, Gancarczyk SM, Simmons BP. Rheumatoid hand and wrist surgery: soft tissue principles and management of digital pathology. J Am Acad Orthop Surg. 2019;27(21):e924-e933. DOI: 10.5435/JAAOS-D-17-00608
- Naniwa S, Nishida K, Nasu Y, et al. A comparative study of short-term outcomes between INTEGRA and AVANTA silicone implants for metacarpophalangeal joints in patients with rheumatoid arthritis. J Hand Surg Am. 2026. DOI: 10.1016/j.jhsa.2026.04.003
MCP arthroplasty outcomes & rehabilitation literature (URLs)
- Chung KC, Burns PB, Wilgis EFS, et al. A multicenter clinical trial in rheumatoid arthritis comparing silicone metacarpophalangeal joint arthroplasty with medical treatment. J Hand Surg Am. 2009;34(5):815-823. DOI: 10.1016/j.jhsa.2009.01.018 — https://pmc.ncbi.nlm.nih.gov/articles/PMC4381953/
- Chung KC, Burns PB, Kim HM, et al. Long-term followup for rheumatoid arthritis patients in a multicenter outcomes study of silicone metacarpophalangeal joint arthroplasty. Arthritis Care Res (Hoboken). 2012;64(9):1292-1300. DOI: 10.1002/acr.21705 — https://pubmed.ncbi.nlm.nih.gov/22511483/
- Burns PB, Zhong L, Chung KC. Seven-year outcomes of the Silicone Arthroplasty in Rheumatoid Arthritis (SARA) prospective cohort study. Arthritis Care Res (Hoboken). 2017. DOI: 10.1002/acr.23105 — https://pmc.ncbi.nlm.nih.gov/articles/PMC5376377/
- Chung KC, Burns PB, et al. Patient expectations and long-term outcomes in rheumatoid arthritis patients: results from the SARA study. Clin Rheumatol. 2015;34(4):641-651. DOI: 10.1007/s10067-014-2775-z — https://pubmed.ncbi.nlm.nih.gov/25267562/
- Massy-Westropp N, Johnston RV, Hill C. Post-operative therapy for metacarpophalangeal arthroplasty. Cochrane Database Syst Rev. 2008;(1):CD003522. DOI: 10.1002/14651858.CD003522.pub2 — https://pmc.ncbi.nlm.nih.gov/articles/PMC8715905/
- Burr N, Pratt AL, Stott D. An alternative splinting and rehabilitation protocol for metacarpophalangeal joint arthroplasty in patients with rheumatoid arthritis. J Hand Ther. 2002;15(1):41-47. DOI: 10.1053/hanthe.2002.v15.01541 — https://pubmed.ncbi.nlm.nih.gov/11866351/
- Delaney R, Trail IA, Nuttall D. Value of dynamic splinting after replacement of the metacarpophalangeal joint in patients with rheumatoid arthritis. Scand J Plast Reconstr Surg Hand Surg. 2003;37(4):232-233. DOI: 10.1080/02844310310005658 — https://pubmed.ncbi.nlm.nih.gov/12755512/





