PIP Joint Fusion Info Evidence
Reviewed by Dr Kieran Hirpara, Specialist Orthopaedic Surgeon Last reviewed
This protocol guides your recovery after fusion (arthrodesis) of the PIP joint (the middle joint of a finger) with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It begins with your home exercise program, followed by the structured clinical protocol written for your hand therapist: bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your hand therapist may adjust the plan depending on how your recovery progresses.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect
A PIP joint fusion takes a worn-out or unstable middle finger joint and joins it solid, so it no longer moves. The joint is set in a functional, slightly bent position rather than dead straight: the bend is gentle in the index and middle fingers (about 15–20°) and increases towards the little-finger side of the hand (about 25–40° in the ring and little fingers), following the natural cascade your fingers make when you curl them. The fused joint is held in place with a small implant (a tension-band wire, a headless screw, K-wires, or a small plate) which holds that angle steady until the bone joins across the fusion.
This operation is often chosen for the index and middle fingers, where a stable joint for pinch matters more than movement at the middle joint. The PIP joint is meant to be stiff afterwards: that is the point of the operation. So unlike a tendon or ligament repair, recovery is not about regaining movement at that joint; it is about protecting the fusion until the bone joins, while keeping every other joint of the hand moving freely.
The plan is built around four ideas:
- Protect the fusion until the bone unites. Bony union usually takes about six weeks, and sometimes up to nine to twelve weeks. Until then the fused joint is supported in a splint.
- Keep everything else moving from day one: the fingertip joint, the knuckle, the neighbouring fingers, the thumb and the wrist, so the tendons do not stick down and the rest of the hand does not stiffen.
- Manage swelling and the scar in the early weeks.
- Restore grip and pinch once the fusion has joined. Don't smoke: smoking is known to slow bone healing and delay a fusion uniting.
Precautions and limitations
- Do NOT load, grip or pinch hard through the operated finger until the fusion has united (usually about six weeks, sometimes longer): loading before the bone has joined risks the fusion not taking.
- Keep the fused joint completely still in its splint as directed; do not try to "test" or bend it.
- Keep every other joint moving from the first days: fingertip joint, knuckle, other fingers, thumb and wrist.
- Keep the splint clean and dry, wear it as directed, and look after the wound and any pin sites.
- Do NOT drive while you cannot safely control the wheel, usually until you are out of the splint at around four to six weeks.
- Don't smoke: it delays the bone joining.
For wound, swelling and scar management, see the practice's wound care guidance.
Your exercises

Kieran Hirpara 4.0
DIP movement of the operated finger
With your hand therapist's go-ahead, gently bend and straighten the very last (fingertip) joint of the operated finger. Steady the middle of the finger with your other hand so only the fingertip moves. The fused joint must stay completely still — only the tip bends. Keeping this joint moving stops the tendons sticking down while the fusion heals.
10 times, 3 times a day, fingertip joint only
Kieran Hirpara 4.0
MCP knuckle movement of the operated finger
Gently bend and straighten the big knuckle (where the finger meets the hand) of the operated finger. The fused middle joint stays still throughout — only the knuckle moves. This keeps the knuckle supple and stops the finger stiffening up while the fusion settles.
10 times, 3 times a day, knuckle joint only
Kieran Hirpara 4.0
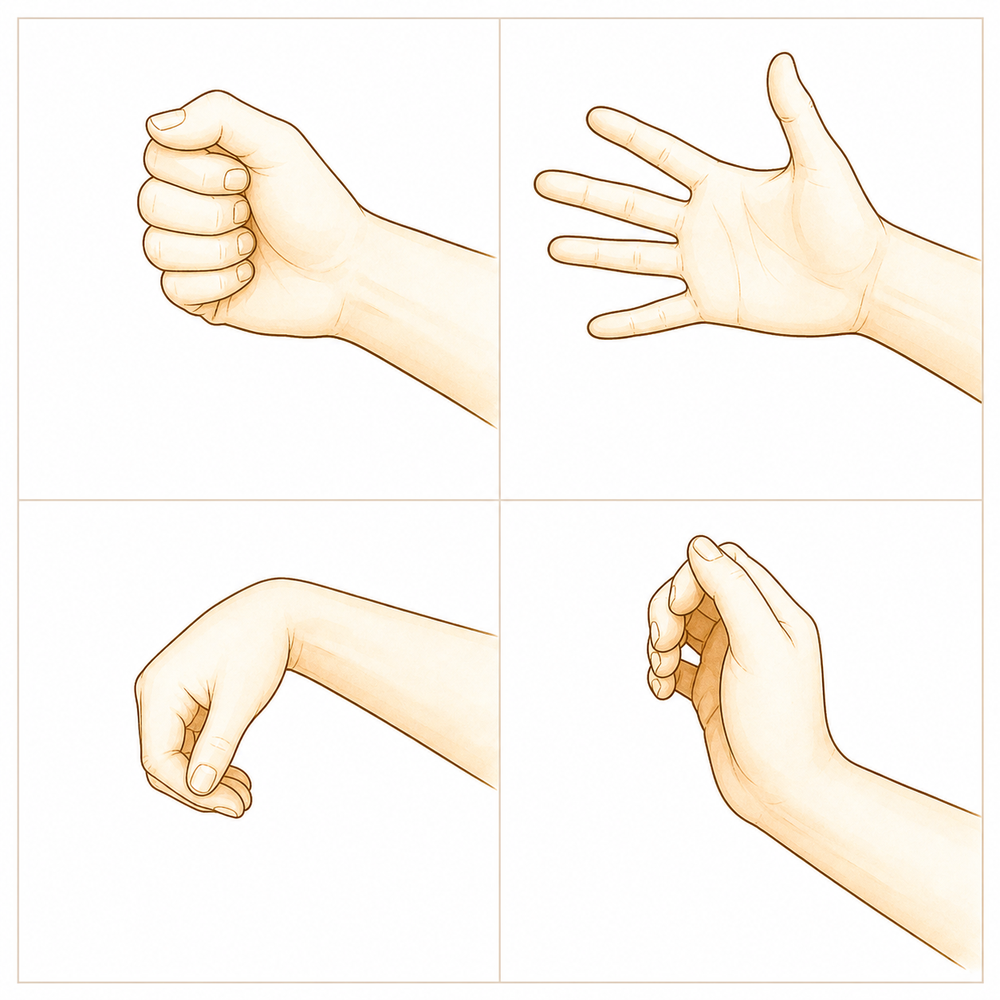
Move all your other fingers, thumb and wrist
From the very first days, keep every joint that was NOT operated on moving freely — make a full fist and open right out with your other fingers, move your thumb in all directions, and bend, straighten and circle your wrist. This is the single most important thing you can do to keep your hand supple and prevent stiffness while the fused joint is protected.
10 times each, several times a day

Kieran Hirpara 4.0
Tendon glides (hook, fist, straight)
Move your hand slowly through three shapes to keep the tendons gliding: a hook (bend the tip and middle joints, knuckles straight), a full fist, then a flat straight hand. Do this with your unoperated fingers fully, and let the operated finger move only as far as the free (non-fused) joints allow. This keeps the tendons running smoothly and stops them sticking down near the surgery.
5 of each shape, 3 times a day
Kieran Hirpara 4.0
Scar massage
Once the wound is fully healed and your hand therapist has checked it, rub a little moisturiser into the scar using firm small circles for a couple of minutes. This softens the scar, settles the tenderness, and stops it tethering to the tissues underneath. Do not start this until the skin is fully closed.
2–3 minutes, 2–3 times a day (after the wound has healed)

Kieran Hirpara 4.0
Pinch and grip strengthening (after union)
A LATER exercise — only once the fusion has united and your hand therapist starts you on strengthening (usually after about six weeks). Squeeze a soft ball or putty for grip, and pinch a small object between your thumb and the operated finger to build the lateral pinch the fusion was done to make stable. Build the effort up gradually. Do NOT do any resisted gripping or pinching before you are cleared — it loads the fusion before the bone has joined.
10 times, 2–3 times a day, as guided (after union only)
These are the exercises from your handout. Start them only as guided by Dr Hirpara and your hand therapist, staying within whatever limits you have been given. The early exercises keep the fingertip joint, the knuckle, and all your other fingers, thumb and wrist moving, without moving or loading the fused joint itself, which stays still in its splint. Scar massage begins once the wound is healed. Pinch and grip strengthening belongs to a later phase and should not be started until the fusion has united and you are specifically cleared. Stop anything that causes sharp pain over the fused joint.
Your clinical protocol
The rest of this page is the staged clinical protocol for rehabilitation after PIP joint arthrodesis. This section is to be provided to your hand therapist, and each phase opens with a plain-English explanation of what is happening. The fusion must be protected from load until bony union (typically ~6 weeks, up to 9–12 weeks); the governing principle is "protect the fused joint, mobilise everything else": DIP, MCP, adjacent digits, thumb and wrist move from day one to prevent tendon adhesion and stiffness, with oedema and scar managed early and grip/pinch restored only after union.
Prior to treatment, check the patient's operation report and past medical history, and liaise with the treating surgeon regarding the fixation used (tension-band wire, headless intramedullary screw, K-wires, or plate), the set fusion angle, and whether K-wires are buried or to be removed. Dr Hirpara fuses the PIP in a functional flexed position that increases ulnar-ward across the hand (index/middle ≈ 15–20°, ring/little ≈ 25–40°), most often for the index/middle finger where lateral pinch stability outweighs PIP motion. The fused joint is held in a splint until radiographic union; the evidence base is low-level (level-4 case series and expert consensus), so timings are individualised, not graded thresholds.
Phase I — protect and settle (weeks 0 to 2)
The first two weeks protect the fusion and settle swelling and the wound, while every other joint of the hand starts moving immediately.
For your hand therapist:
Immobilisation - Acute volar finger splint or cast spanning the MCP and PIP, but leaving the DIP free - Fused PIP held still; elevation for oedema
Education and precautions - No grip, pinch or loading through the operated finger - Keep the splint clean and dry; protect the wound and any pin sites
Management - Wound: surgical dressings as directed; monitor for infection and pin sites if K-wires used - Oedema: elevation, gentle pumping of the free joints, ice as needed - Exercises: from day one, active motion of all non-fused joints: adjacent fingers (full fist/extension), thumb, wrist; begin DIP active motion of the operated finger within days; tendon glides of the adjacent digits; no movement or loading of the fused PIP
Criteria to progress - Wound settling; swelling controlled; ready for a definitive custom splint at around 1–2 weeks
Phase II — custom thermoplastic splint and active motion of the free joints (weeks 2 to 6)
From about two weeks a custom thermoplastic splint supports the fused joint while freeing the adjacent joints for active motion. The operated finger's DIP and MCP are exercised out of the splint; the fused PIP remains protected. No resisted grip, pinch or loading yet.
For your hand therapist:
Assessments - Adjacent-joint ROM, oedema, wound/scar review; confirm fixation stable on clinical grounds and per surgeon
Immobilisation - Transition to a custom thermoplastic splint supporting the fused PIP while freeing adjacent joints; continuous protective splinting to ~6 weeks
Education and precautions - No resisted grip, pinch or loading of the operated finger until union - Out of the splint for exercises only
Management - Exercises: active DIP and MCP motion of the operated finger out of the splint (DIP started within days, MCP added here); tendon glides of adjacent digits; continued thumb/wrist/adjacent-finger motion; commence scar and oedema management once the wound is healed - No resisted grip/pinch/loading
Criteria to progress - Radiographic union (typically around 6 weeks, up to 9–12); fused joint clinically and radiologically stable before any loading
Phase III — wean the splint and progress light use (from ~6 weeks, once united)
Once the fusion has united (usually around six weeks), the splint is weaned and progressively cut down, light functional use is introduced, and pinch, opposition and gripping are gradually rebuilt. K-wires, if used, are typically removed around six weeks.
For your hand therapist:
Assessments - Confirm radiographic union with the surgeon; grip/pinch strength versus the other hand; ROM of the free joints; scar
Education and precautions - Wean and cut down the splint once union is confirmed; remove K-wire ~6 weeks if used - Progress loading gradually: light use first, then graded pinch/grip
Management - Exercises: progress light functional use → pinch, opposition and gripping; commence grip/pinch strengthening (ball/putty, lateral pinch) and build gradually; continue scar work - Splint weaned after radiographic union
Criteria to progress - United fusion tolerating light load pain-free; splint discontinued; ready for progressive strengthening
Phase IV — progressive strengthening and return (from ~8–12 weeks)
With the fusion united and light use restored, strengthening and loading are progressed, and return to sport, heavy or manual activity is built up. The final settled result is reached at around nine to twelve months.
For your hand therapist:
Assessments - Grip and pinch strength versus the other side; functional and work-/sport-specific testing as appropriate
Education and precautions - Build resisted loading up gradually; the fused joint is permanently stiff by design; focus strength on grip and lateral pinch
Management - Exercises: progressive strengthening and loading of grip and pinch; graded return to sport, heavy and manual tasks - Consider discharge once strength is functional and near-symmetrical; refer back to the treating doctor if recovery plateaus
Criteria for return - Pain-free, stable fused joint under load; adequate grip/pinch strength for the task, judged clinically not by the calendar; final settled result at 9–12 months
Getting back to work and activity
Light everyday hand use with the rest of the hand is encouraged from the start, within comfort; the key restriction is no gripping, pinching or loading through the operated finger until the fusion has joined. Because you must not drive while you cannot safely control the wheel, plan for help with transport in the early weeks; driving usually resumes at around four to six weeks, once you are out of the splint and can safely control the car.
After union (around six weeks) you can begin light use and gentle gripping. Lifting, gripping and pinch build up from about eight weeks, and full activity or sport from about twelve weeks. The fusion keeps settling for several months, so the final, fully settled result is at around nine to twelve months. These timings are expert-consensus single-clinic guides (typical and individualised, not graded thresholds) and your progress is judged by Dr Hirpara and your hand therapist according to how the fusion heals, not by the calendar alone.
After your protocol
This protocol works alongside the practice's general recovery advice; see also managing post-operative pain, wound care and scar management. The phased plan above reflects published guidance on rehabilitation after PIP joint arthrodesis, and your ongoing recovery is guided individually by Dr Hirpara and your hand therapist according to how your finger heals.
Evidence & references
Topic scope: post-operative rehabilitation after arthrodesis (fusion) of the proximal interphalangeal (PIP) joint of a finger — a worn, painful or unstable PIP joint is fused solid in a functional flexed position. This is a fusion, not a reconstruction or a motion- preserving procedure: the PIP is deliberately made stiff to trade motion for a stable, pain-free, load-bearing digit. The rehab is therefore not about regaining PIP motion but about protecting the construct until bony union while keeping every other joint of the hand moving, then restoring grip and pinch.
Defining principle of the rehab here: PIP arthrodesis eliminates motion at one joint by design to gain stability for pinch and grip. The fused joint is set in a functional flexed position that increases ulnar-ward across the hand (index/middle ≈ 15–20°, ring/little ≈ 25–40°, following the digital cascade) and held by internal fixation (tension-band wire, headless intramedullary screw, K-wires, or plate) until union. Because nothing here needs to move to heal — it needs to unite — the single governing rule is "protect the fused joint, mobilise everything else." DIP, MCP, adjacent digits, thumb and wrist move from day one to prevent tendon adhesion and stiffness; oedema and scar are managed early; grip and pinch are restored only after radiographic union (~6 weeks, up to 9–12). The branch point is the indication — primary degenerative/post-traumatic fusion versus salvage of a failed PIP arthroplasty, where union is slower and the construct more demanding.
A. PROCEDURE OUTCOMES (PIP arthrodesis)
PIP arthrodesis is a reliable, well-established salvage and reconstructive operation, but its evidence base is uniformly low-level — predominantly retrospective level-4 case series and expert opinion, with no randomised controlled trials. Outcomes are reported as union, complication and reoperation rates rather than from comparative trials.
- The evidence base is low-level and consensus-driven. A systematic review of PIP arthrodesis found the literature is overwhelmingly level-4 (~94%) with no RCTs; conclusions on fixation choice and outcomes rest on case series and expert consensus [EFORT Open Rev 2021, DOI 10.1530/eor-21-0102]. Low (level-4 SR, no RCTs).
- Fixation holds the angle to union; nonunion and reoperation are the principal concerns. Series reporting nonunion and reoperation identify patient factors (including smoking and comorbidity) as drivers of failure, underscoring that the rehab job is to protect the construct until the bone joins [HAND 2020, DOI 10.1177/1558944720939196]. Low–moderate (case series).
- The fusion angle is chosen for function, especially pinch. A biomechanical/kinematic study of index PIP fusion (simulated 30–50°) shows the set angle is a functional trade-off: fusing the index/middle PIP stabilises lateral (key) pinch at the cost of PIP motion, which is why these digits are common fusion sites [J Hand Surg Am 2011, DOI 10.1016/j.jhsa.2011.09.010]. Mechanistic / cadaveric.
- Arthrodesis is a dependable salvage for failed PIP arthroplasty, but union is slow. A series of arthrodesis for failed PIP joint replacement reported a mean time to union of 5.8 months, illustrating that salvage fusions unite more slowly than primary fusions and need correspondingly extended protection [J Hand Surg Am 2011, DOI 10.1016/j.jhsa.2010.10.030]. Low (case series).
- The biomechanics of digital loss/fusion frame the functional cost. Reviews of the biomechanics of digital amputation and fusion describe how eliminating an IP joint redistributes grip and pinch mechanics — the rationale for accepting a stiff joint when it buys stability [Hand Clin 2016, DOI 10.1016/j.hcl.2016.07.003]. Mechanistic / narrative.
B. REHABILITATION / THERAPY EVIDENCE
There are no trials of rehab regimens after PIP arthrodesis; the programme is built on sound surgical principle and expert consensus. The two evidence-anchored levers are the union timeline (which sets when load may be applied) and the modifiable risk factor of smoking (which delays union).
- Protect-until-union, mobilise-everything-else is the consensus regimen. The fused PIP is splinted continuously until radiographic union (~6 weeks, up to 9–12); from day one the DIP, MCP, adjacent digits, thumb and wrist are actively moved to prevent tendon adhesion and global hand stiffness. This is stable across sources (surgeon protocols, hand-therapy guidance and patient-education material) even though it is not trial-tested [Melbourne Arm Clinic protocol; OrthOracle PIPJ arthrodesis; OrthoInfo finger IP fusion]. Consensus / expert.
- Smoking is an evidence-supported delayed-union risk. A study of hand and wrist arthrodesis found smoking delays union, making smoking cessation the one rehab-adjacent intervention with direct supporting evidence in this setting [J Hand Surg Am 2022, DOI 10.1016/j.jhsa.2022.05.016]. Moderate (cohort, modifiable risk factor).
- Union timing governs progression — and is slower in salvage fusions. Primary fusions are typically protected to ~6 weeks; salvage of failed arthroplasty unites far more slowly (mean 5.8 months), so loading must be union-led rather than calendar-led [J Hand Surg Am 2011, DOI 10.1016/j.jhsa.2010.10.030]. Low (case series).
- The set fusion angle is the functional anchor of the rehab goal. Because the index/middle PIP is fused at ~15–20° (and ring/little at ~25–40°) specifically to stabilise lateral pinch, the Phase III–IV strengthening rightly targets pinch and grip rather than any attempt at PIP motion [J Hand Surg Am 2011, DOI 10.1016/j.jhsa.2011.09.010]. Mechanistic.
Recovery trajectory (expected, evidence-anchored)
| Phase | Window | Restraint | Hand use / therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Protect & settle | Week 0–2 | Volar finger splint/cast spanning MCP + PIP, DIP left free | Elevation, wound/pin-site care, oedema control; active DIP within days + full motion of all non-fused joints (adjacent digits, thumb, wrist) | No grip / pinch / loading | Fused PIP kept still; everything else mobilised from day one |
| II — Custom splint & free-joint motion | Week 2–6 | Custom thermoplastic splint supporting the fused PIP, freeing adjacent joints; continuous splinting to ~6 wk | Active DIP + MCP of operated finger out of splint; tendon glides of adjacent digits; scar/oedema once healed | No resisted grip / pinch / loading | Union typically at ~6 wk (up to 9–12); load only after radiographic union |
| III — Wean splint & light use | From ~6 wk (united) | Splint weaned/cut down after union; K-wire out ~6 wk if used | Progress light use → pinch, opposition, gripping; begin grip/pinch strengthening | Graded grip/pinch, build gradually | Restraints lifted only once union confirmed |
| IV — Strengthen & return | ~8–12 wk+ | Restrictions lifted | Progressive strengthening/loading; return to sport/heavy/manual work | Build load progressively; target lateral pinch | Final settled result 9–12 months |
(Phase windows mirror the precautions in the patient protocol; they are expert-consensus, single-clinic guides — typical and individualised, not graded or trial-derived thresholds. Return milestones: driving ~6 wk, light use/gentle grip ~6 wk after union, lifting/gripping/pinch ~8 wk, full activity/sport ~12 wk, final result 9–12 months.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY
- Whole topic is low-level evidence. PIP arthrodesis rests on level-4 case series and expert consensus with no RCTs (~94% level-4 in systematic review). All outcome and timing figures should be read as typical guides, not trial-validated thresholds [EFORT 2021]. Low.
- Fixation choice is unsettled. Tension-band wire, headless intramedullary screw, K-wires and plate all achieve union; comparative data are weak and selection is largely surgeon preference and bone/soft-tissue quality [EFORT 2021; HAND 2020]. Low.
- Fusion angle is a functional trade-off, not a fixed number. The ~15–20° (index/middle) to ~25–40° (ring/little) cascade is consensus-stable but individualised to the digit and the demands of pinch [J Hand Surg Am 2011 kinematics]. Mechanistic / consensus.
- Union timing is variable and indication-dependent. Primary fusions ~6 weeks; salvage of failed arthroplasty far slower (mean 5.8 months). Loading must be union-led [J Hand Surg Am 2011 salvage series]. Low.
- Smoking and patient factors drive nonunion/reoperation. Smoking is an evidence-supported delayed-union risk and a modifiable target [J Hand Surg Am 2022; HAND 2020]. Moderate (for the smoking association).
D. EVIDENCE STRENGTH FLAGS (summary)
- STRONG (RCT / SR): none — there are no RCTs in PIP arthrodesis; the best synthesis is a level-4 systematic review (~94% level-4 studies).
- MODERATE: smoking as a delayed-union risk after hand/wrist arthrodesis; patient factors driving nonunion/reoperation; cadaveric/kinematic basis for the functional fusion angle and pinch rationale.
- WEAK / CONSENSUS: the protect-until-union, mobilise-everything-else rehab regimen (mechanistically sound, not trial-tested); the specific fusion angles (consensus-stable); exact timelines (single-clinic, expert-consensus guides — typical, not graded thresholds); fixation choice (surgeon preference).
CITATIONS
RAG corpus (180,000+ Orthopaedic articles)
- Proximal interphalangeal joint arthrodesis: a systematic review (predominantly level-4 evidence; no RCTs). EFORT Open Rev. 2021. DOI: 10.1530/eor-21-0102
- Nonunion and reoperation after proximal interphalangeal joint arthrodesis: patient factors and outcomes. HAND. 2020. DOI: 10.1177/1558944720939196
- Index finger proximal interphalangeal joint arthrodesis and pinch kinematics (simulated 30–50° fusion). J Hand Surg Am. 2011. DOI: 10.1016/j.jhsa.2011.09.010
- Arthrodesis as salvage for failed proximal interphalangeal joint arthroplasty (mean time to union 5.8 months). J Hand Surg Am. 2011. DOI: 10.1016/j.jhsa.2010.10.030
- Smoking delays union after hand and wrist arthrodesis. J Hand Surg Am. 2022. DOI: 10.1016/j.jhsa.2022.05.016
- Biomechanics of digital loss and fusion. Hand Clin. 2016. DOI: 10.1016/j.hcl.2016.07.003
PIP arthrodesis rehabilitation & procedure literature (URLs)
- Melbourne Arm Clinic. PIP / DIP arthrodesis rehabilitation protocol. https://melbournearmclinic.com.au/orthopaedic-rehabilitation/shoulder-rehabilitation/pip-dip-arthrodesis-protocol/
- OrthOracle. Proximal interphalangeal joint (PIPJ) arthrodesis in the hand using the Apex system (Extremity Medical). https://www.orthoracle.com/library/proximal-interphalangeal-joint-pipj-arthrodesis-in-the-hand-using-the-apex-system-extremity-medical/
- EFORT Open Reviews. Proximal interphalangeal joint review (PMC). https://pmc.ncbi.nlm.nih.gov/articles/PMC6598614/
- American Academy of Orthopaedic Surgeons (OrthoInfo). Finger (interphalangeal) joint fusion. https://orthoinfo.aaos.org/en/treatment/finger-ip-joint-fusion/





