Blood Thinners Around Surgery Info
Last reviewed
Patients › Recovery
How anticoagulants and antiplatelets work, and why the timing of stopping each before surgery differs — platelet turnover, half-lives and clot risk.
"Blood thinner" covers two families of medicine that work in completely different ways, and that difference is exactly why some have to be stopped a week before an operation while others only need a day or two. Knowing which one you take, and how it actually works, makes the instructions you're given far less mysterious.
First, how does blood actually clot?
To make sense of the different blood thinners it helps to know how your blood normally seals a leak, because each medicine interrupts a different step.
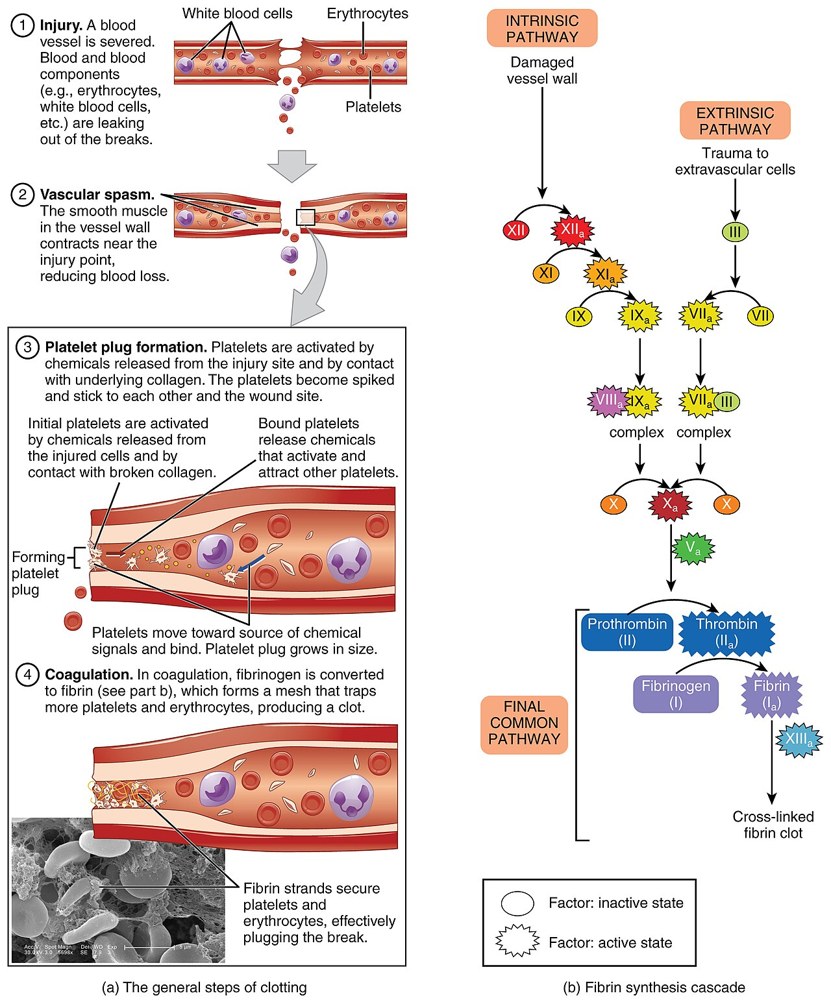
When a blood vessel is cut or damaged, your body plugs it in two stages:
-
Platelets plug the gap: the fast first responders. Platelets are tiny cell fragments that circulate in the blood doing nothing until they are needed. The instant they meet a damaged vessel wall they turn sticky, pile onto the injury and clump together, forming a soft, temporary plug within seconds to minutes. Think of it as the body's emergency patch.
-
The clotting cascade sets the plug solid. That platelet plug is fragile on its own. To reinforce it, the blood runs a chain reaction called the clotting cascade, a series of proteins called clotting factors (most made by the liver, several of them needing vitamin K) that switch one another on in sequence, like a row of dominoes. The cascade finishes by turning a protein called fibrinogen into fibrin, a mesh of fine threads that weaves through the platelet plug and locks it into a firm, stable clot.
So a finished clot is really platelets held together by a fibrin mesh. When it seals a wound that is exactly what you want; but the same process happening unwanted inside an artery or vein causes a heart attack, stroke or DVT. That is what blood thinners are prescribed to prevent.
Here is the key to everything below: the two families of blood thinner each jam a different stage. Antiplatelet medicines blunt the first step (the platelets); anticoagulant medicines interrupt the second (the clotting- factor cascade). That single difference also explains why the timing before surgery is so different, because "undoing" a platelet is not the same as "undoing" a clotting factor.
Antiplatelet medicines
(aspirin, clopidogrel/Plavix, ticagrelor/Brilinta, prasugrel/Effient)
These stop the tiny blood cells called platelets from sticking together to start a clot.
- Aspirin and clopidogrel (and prasugrel) work irreversibly: once the drug reaches a platelet, that platelet is switched off for the rest of its life. Your body cannot turn it back on. The only way back to normal clotting is to make brand-new platelets, and platelets live only about 7–10 days, with roughly 10% replaced each day. So after you stop, it takes about 5–7 days to build up enough fresh, working platelets for safe surgery. That platelet turnover is the whole reason these are usually stopped about a week beforehand.
- Ticagrelor is reversible; it lets go of the platelet rather than permanently disabling it, so it clears a little faster, but still needs a few days.
- Aspirin is often continued for operations with a low bleeding risk, or when it is protecting a heart stent, because the small bleeding risk is outweighed by the clot risk. Your surgeon makes that call.
Anticoagulants
These work further down the clotting chain, on the clotting factors in the blood rather than on the platelets.
Warfarin (Coumadin, Marevan). Warfarin stops your liver from making several vitamin-K-dependent clotting factors. It does not remove the factors already circulating; those have to be used up and cleared naturally, which takes about 5 days. That's why warfarin is usually stopped about 5 days before surgery and a blood test (the INR) is checked to confirm your blood has returned to normal. If you're at high risk of a clot during that gap, you may be "bridged" with short-acting heparin injections that can be stopped much closer to the operation.
The newer tablets: DOACs (apixaban/Eliquis, rivaroxaban/Xarelto, dabigatran/Pradaxa, edoxaban). Each blocks a single specific clotting factor, and the body clears them quickly, with a half-life of around 12 hours. Because they wash out so fast, they usually only need to be stopped 1–2 days before surgery. The wait is longer if your kidneys don't clear the drug well (especially dabigatran, which leaves mostly through the kidneys) or if the operation has a high bleeding risk. They need no INR monitoring and usually no bridging.
Heparin / low-molecular-weight heparin (enoxaparin/Clexane) injections. Short-acting; used to bridge warfarin or to prevent clots. Because they wear off in hours, the last dose is simply timed close to surgery (often around 24 hours before a treatment dose).
Why the timing is what it is — in one line
It comes down to how the drug works and how your body clears it: irreversible platelet drugs need you to grow new platelets (about a week); warfarin needs old clotting factors to clear (about 5 days); the DOACs simply wash out (a day or two). Every plan then also weighs your personal clot risk, which is why two people on the same drug can be given different instructions.
What you must do
- Bring an exact list of everything you take to your pre-operative assessment, including aspirin and supplements like fish oil, which also affect bleeding.
- Follow the specific written stop and restart dates you are given. They are tailored to your drug, your kidney function and your operation.
- Never stop, start or change a blood thinner on your own, and don't assume your timing matches a friend's.
- Tell every clinician involved that you take one.
After your operation
Blood thinners are restarted once the bleeding risk has settled, sometimes within a day, sometimes longer after higher-bleeding-risk surgery. You'll be told exactly when. The clot the medicine prevents doesn't disappear because you've had an operation, so restarting on time matters as much as stopping did.
Call us if
- You realise you took a dose you were told to skip, or skipped one you were told to take
- You have unusual or heavy bruising or bleeding, blood in the urine or stool, black tarry stools, or bleeding that won't stop
- You are unsure what to do with your blood thinner before your operation: always ask rather than guess





