பகுதியளவு மணிக்கட்டு ஒன்றிணைப்பு
Patients › Rehabilitation
சுமார் ஆறு முதல் எட்டு வாரங்களில் எலும்புகள் பிணைக்கப்படும் வரை அணிந்துபோன மணிக்கட்டுக்கு ஒரு பகுதியளவு மணிக்கட்டு இணைப்புக்குப் பிறகு ஒரு பாதுகாக்கப்பட்ட மீட்பு திட்டம் (கேபிடோலூனட் இணைப்பு, பொதுவாக ஸ்காஃபோய்டை அகற்றுவதன் மூலம்), பின்னர் படிப்படியாக ஒரு பயனுள்ள ஆனால் வேண்டுமென்றே குறைக்கப்பட்ட மணிக்கட்டு இயக்க வளைவு மற்றும் பிடியின் வலிமையை மீட்டெடுக்கிறது.
இந்த நடைமுறை ஒரு பிறகு உங்கள் மீட்பு வழிகாட்டுகிறது பகுதியளவு மணிக்கட்டு இணைப்பு (ஒரு அறுவை சிகிச்சையானது, கழுத்து எலும்புகளின் நடுப்பகுதியில் உள்ள சிறிய எலும்புகளை இணைத்து, பெரும்பாலும் lunate க்கு தலைமை ஒரு தலைநகர இணைப்புஇது உங்கள் வீட்டு உடற்பயிற்சி திட்டத்துடன் தொடங்குகிறது, அதைத் தொடர்ந்து கட்டமைக்கப்பட்ட மருத்துவ நெறிமுறை எழுதப்பட்டுள்ளது உங்கள் கை சிகிச்சையாளர்: இந்த பக்கத்தை அல்லது அதன் PDF ஐ உங்கள் முதல் சிகிச்சை வருகைக்கு எடுத்துச் செல்லுங்கள், இதனால் உங்கள் மறுவாழ்வு ஒருங்கிணைந்ததாக இருக்கும். உங்கள் கை சிகிச்சையாளர் உங்கள் மீட்பு எவ்வாறு முன்னேறுகிறது என்பதைப் பொறுத்து திட்டத்தை சரிசெய்யலாம்.
அறுவை சிகிச்சைக்குப் பிறகு உங்கள் காயத்தைப் பற்றி ஏதேனும் கவலைகள் இருந்தால், அறைகளைத் தொடர்பு கொள்ளுங்கள். காயத்தின் புகைப்படத்தை எடுத்து அதை மதிப்பாய்வு செய்ய மின்னஞ்சல் அனுப்புவது பெரும்பாலும் உதவியாக இருக்கும்.
எதிர்பார்ப்பது என்ன
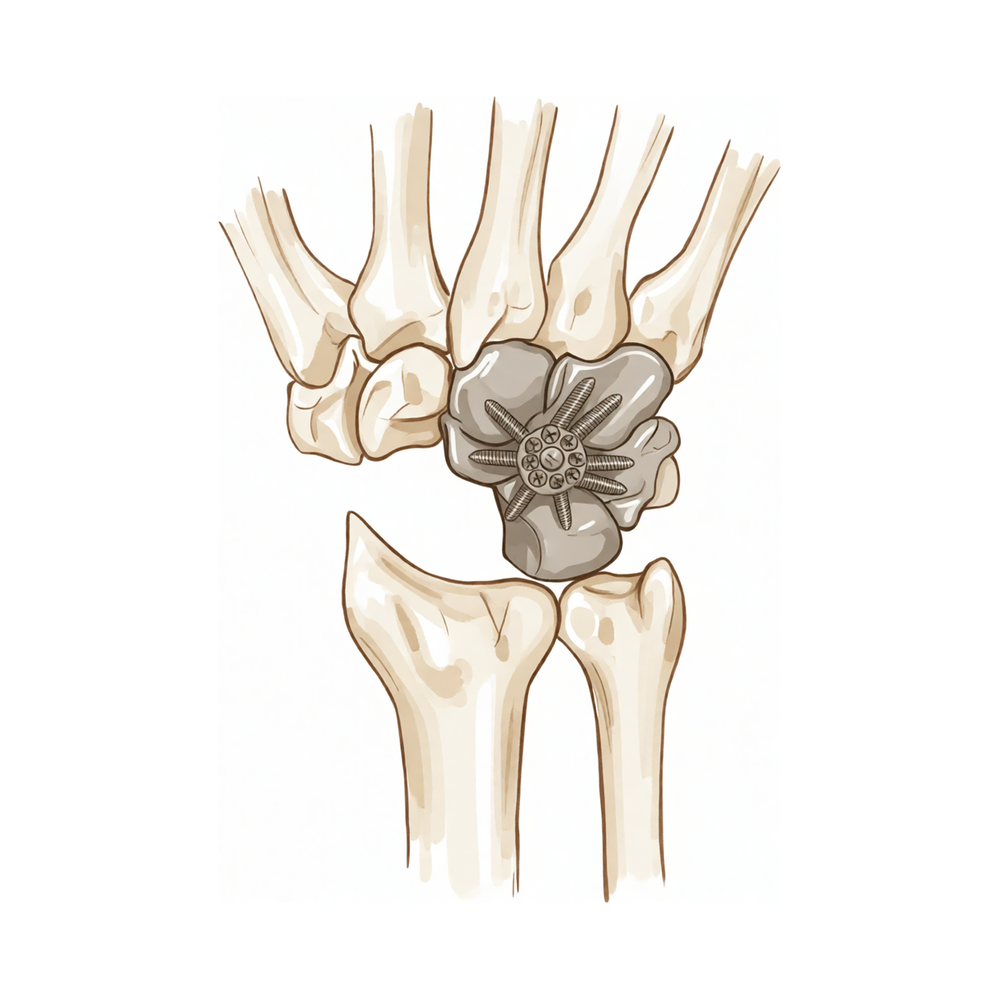
ஒரு பகுதி மணிக்கட்டு இணைப்பு ஒரு பழைய ஸ்காஃபோய்டு சிக்கலைப் பின்பற்றும் பாதையில் அணிந்திருக்கும் ஒரு மணிக்கட்டை (இரத்தப்போக்கு) சிகிச்சையளிக்கிறதுஃ ஸ்காஃபோலூனட் லிகிமெண்ட் காயம் (ஒரு "SLAC" மணிக்கட்டு) அல்லது பழைய ஒருபோதும் குணமடையாத ஸ்காஃபோயிட் முறிவு ("SNAC" மணிக்கட்டு). சேதமடைந்த ஸ்காஃபோய்டு அகற்றப்பட்டு, மார்பகத்தின் நடுத்தர எலும்புகள் ஒன்றாக இணைக்கப்படுகின்றன, இதனால் அவை இனி தேய்க்காது. lunate க்கு தலைமை சில நேரங்களில் அண்டை எலும்புகள் உட்பட (ஒரு capitolunate இணைவு); lunate, capitate, triquetrum மற்றும் hamate அனைத்தும் இணைந்தால் இது ஒரு நான்கு மூலை இணைப்பு, அதே மீட்பு கொள்கைகளை பின்பற்றுகிறது.
இந்த நடவடிக்கையின் பின்னணியில் உள்ள முக்கிய யோசனை என்னவென்றால், மணிக்கட்டில் ஒரு பகுதி மட்டுமே உருகியுள்ளது, அது அனைத்து இல்லை. முதுகெலும்பிற்கும் முதுகெலும்பிற்கும் இடையில் உள்ள மூட்டு (ரேடியஸ்) வேண்டுமென்றே தனியாக விடப்படுகிறது. அந்த பாதுகாக்கப்பட்ட மூட்டுதான் மணிக்கட்டு தொடர்ந்து நகர அனுமதிக்கிறது:
- உடைந்துபோன மேற்பரப்புகளை இணைப்பது வலியை நீக்குகிறது: அதுதான் முக்கிய இலக்கு, அது நம்பகத்தன்மையுடன் அடையப்படுகிறது.
- ரேடியஸ் லூனட் கூட்டு வைத்து நீங்கள் பயனுள்ள இயக்கம் வைத்து அர்த்தம். சமரசம் என்பது இயக்கம் குறைக்கப்படுகிறது: பெரும்பாலான மக்கள் தங்கள் முன்னாள் வளைக்கும் வரம்பில் ஏறக்குறைய பாதி முதல் மூன்றில் இரண்டு பங்கு வரை முடிவடைகிறார்கள், மற்ற பக்கத்தின் மூன்றில் நான்கு பங்கு பற்றும் வலிமை. இது ஒரு சாதாரண, எதிர்பார்க்கப்படும் விளைவு (ஒரு சிக்கல் அல்ல) மற்றும் வலி, அணிந்த மணிக்கட்டுக்கு இது பொதுவாக மிகவும் பயனுள்ளதாக இருக்கும்.
ஒன்றிணைந்த எலும்புகள் ஒரு முறிவைப் போலவே திடமாக ஒன்றாக இணைவதற்கு நேரம் தேவைப்படுகிறது. முதல் ஆறு முதல் எட்டு வாரங்கள் இது நடக்கும் போது மணிக்கட்டு ஒரு கட்டி அல்லது ஸ்பிளெண்டில் அமைதியாக வைக்கப்படுகிறது. அந்த நேரத்தில் விரல்கள், கட்டைவிரல் மற்றும் முதுகெலும்புகள் சுதந்திரமாக நகரும், ஆனால் மணிக்கட்டு தன்னை ஓய்வெடுக்கிறது. அறுவை சிகிச்சை நிபுணர் எக்ஸ்-ரே மூலம் எலும்புகள் உறுதிப்படுத்தியவுடன் ஒன்றுபட்டது, மணிக்கட்டு இயக்கம் மற்றும் பின்னர் வலுவூட்டல் ஆகியவை கவனமாக கட்டங்களாக திறக்கப்படுகின்றன. உங்கள் எதிர்பார்ப்புகளை ஆரம்பத்தில் அமைப்பது (முழுமையாக நகரும் ஒன்றை விட வசதியான, பயனுள்ள மணிக்கட்டு) மீட்பின் ஒரு முக்கிய பகுதியாகும்.
முன்னெச்சரிக்கைகள் மற்றும் வரம்புகள்
- உங்கள் அறுவை சிகிச்சை நிபுணர் இணைப்பு குணமடைந்துள்ளதை உறுதிப்படுத்தும் வரை (வழக்கமாக ஆறு முதல் எட்டு வாரங்கள் வரை) உங்கள் மணிக்கட்டை அதன் அறுவை சிகிச்சை அல்லது அறுவை சிகிச்சை முறையில் அமைதியாக வைத்திருங்கள்ஃ மணிக்கட்டை நகர்த்துவதற்கு முன் எலும்புகள் பிணைக்கப்பட வேண்டும்.
- உங்கள் விரல்கள், கட்டைவிரல் மற்றும் முன்கை முதல் நாள் இருந்து நகரும் வைத்து, ஆனால் செய்ய இல்லை சுத்தம் செய்யப்படும் வரை மணிக்கட்டை நகர்த்தவும்.
- செய் இல்லை குணமடையும் எலும்பையும் எந்தவொரு தட்டு, திருகுகள் அல்லது கிராப்பர்களையும் பாதுகாக்க இது உறுதிப்படுத்தப்படும் வரை, மண்டை வழியாக வலுவாகப் பிடிக்கவும், தூக்கவும், தள்ளவும், இழுக்கவும் அல்லது சுமக்கவும்.
- குறைக்கப்பட்ட இறுதி இயக்க வரம்பை எதிர்பார்க்கலாம்: இது மணிக்கட்டில் ஒரு பகுதியை உருகுவதன் திட்டமிடப்பட்ட விளைவாகும், ஏதேனும் தவறு நடந்ததற்கான அறிகுறியாக இல்லை.
- பிசின் அல்லது டிரெஸிங்கை சுத்தமாகவும் உலர்ந்ததாகவும் வைத்திருக்கவும், இல்லை வாகனத்தை ஓட்டுவது அல்லது ஓட்டுநரை பாதுகாப்பாக கட்டுப்படுத்த இயலாமல் இருப்பது.
காயம், வீக்கம் மற்றும் வடுக்கள் மேலாண்மை, நடைமுறையில் பார்க்க காயம் பராமரிப்பு வழிகாட்டல்.
உங்கள் பயிற்சிகள்
இவை உங்கள் கையேட்டில் உள்ள பயிற்சிகள். டாக்டர் ஹிர்பாரா மற்றும் உங்கள் கை சிகிச்சையாளரின் வழிகாட்டுதலின்படி மட்டுமே அவற்றைத் தொடங்குங்கள், உங்களுக்கு வழங்கப்பட்ட வரம்புகள் மற்றும் வரம்புகளுக்குள் இருங்கள். ஆரம்ப பயிற்சிகள் குணப்படுத்தும் இணைப்புக்கு இடையூறு விளைவிக்காமல் விரல்கள், கட்டைவிரல் மற்றும் முதுகெலும்புகளை நகர்த்த வைக்கின்றன; மணிக்கட்டு தன்னை அதன் நடிப்பு அல்லது அடுக்கில் இன்னும் உள்ளது. மணிக்கட்டு இயக்கம் மற்றும் பிடியை வலுப்படுத்துதல் ஆகியவை பிற்கால கட்டங்களைச் சேர்ந்தவை உங்கள் அறுவை சிகிச்சையாளர் எலும்புகள் ஒன்றிணைந்திருப்பதை உறுதிப்படுத்தும் வரை தொடங்கக்கூடாது.
உங்கள் மருத்துவ நெறிமுறை
இந்த பக்கத்தின் மீதமுள்ள பகுதி, ஒரு பகுதி மணிக்கட்டு இணைப்பிற்குப் பிறகு மறுவாழ்வுக்கான படிப்படியான மருத்துவ நெறிமுறை ஆகும். இந்த பிரிவு உங்கள் கை சிகிச்சையாளருக்கு வழங்கப்பட வேண்டும், ஒவ்வொரு கட்டமும் என்ன நடக்கிறது என்பதற்கான எளிய ஆங்கில விளக்கத்துடன் தொடங்குகிறது. இடுப்பு பழுது போலல்லாமல், இந்த கட்டமைப்பானது எலும்புடையது, மேலும் முன்னேற்றம் ஒரு நிலையான காலண்டர் மூலம் அல்ல, இணைப்பின் ரேடியோகிராஃபிக் ஒன்றிணைப்பால் மூடப்படுகிறது. அறுவை சிகிச்சையாளர் ஒன்றிணைப்பை உறுதிப்படுத்தும் வரை, மணிக்கட்டு அசைவில்லாமல் உள்ளது மற்றும் விரல்கள், கட்டைவிரல் மற்றும் முன்கை மட்டுமே இயக்கப்படுகின்றன; அதன்பிறகு மணிக்கட்டு வரம்பு மற்றும் சுமை மீட்டமைக்கப்படுகின்றன, ஏறக்குறைய 5065% எதிர் பக்க வளைவு நீட்டி மற்றும் ~ 7080% பிடியின் யதார்த்தமான உச்சவரம்புடன்.
சிகிச்சைக்கு முன்னர், நோயாளியின் செயல்பாட்டு அறிக்கையை சரிபார்த்து, பயன்படுத்தப்பட்ட உறுதிப்படுத்தலை (சுற்று / முதுகு தகடு, தலை இல்லாத சுருக்க திருகுகள், ஸ்டேப்லஸ் அல்லது கே-கம்பிகள்) மற்றும் ஸ்காஃபோய்ட் அகற்றப்பட்டதா என்பதை உறுதிப்படுத்தவும். சிகிச்சையளிக்கும் அறுவை சிகிச்சை நிபுணர் ரேடியோகிராஃபிக் இணைப்பை உறுதிப்படுத்தும் வரை மணிக்கட்டு இயக்கத்தைத் தொடங்க வேண்டாம் (வழக்கமாக 68 வாரங்கள், சில நேரங்களில் திருகு அல்லது ஸ்டேப்லஸ் உறுதிப்படுத்தலுடன்). நோயாளிக்கு முதல் வருகையிலிருந்து நோயாளியை அறிவுறுத்துங்கள் நோக்கம் வலி இல்லாத, செயல்பாட்டு மணிக்கட்டு, வேண்டுமென்றே குறைக்கப்பட்ட வில், முழு இயக்கம் அல்ல.
கட்டம் I பாதுகாக்கப்பட்ட இயலாமை ஒற்றுமை வரை (வாரங்கள் 0 முதல் ~ 68)
எலும்புகள் பிணைக்கப்படும்போது கைத்தடி அமைதியாக வைக்கப்படுகிறது. கை மற்றும் முதுகெலும்புகள் இறுக்கம் மற்றும் தசை ஒட்டுதல் ஆகியவற்றைத் தடுக்க முழுமையாக நகர்த்தப்படுகின்றன, ஆனால் கைத்தடி நகர்த்தப்படவில்லை.
உங்கள் கை சிகிச்சையாளருக்கு:
கல்வி மற்றும் முன்னெச்சரிக்கைகள் - மணிக்கட்டு இயலாமை அறுவை சிகிச்சை நிபுணர் ரேடியோகிராஃபிக் இணைப்பை உறுதி செய்யும் வரை (வழக்கமாக 68 வாரங்கள்) - சுறுசுறுப்பான அல்லது செயலற்ற மணிக்கட்டு இயக்கம் இல்லை இந்த கட்டத்தில் - பிடிக்கவோ, தூக்கவோ, தள்ளவோ, இழுக்கவோ அல்லது எடை தாங்கவோ கூடாது அறுவை சிகிச்சை செய்யப்பட்ட மணிக்கட்டு வழியாக - ஆரம்பத்தில் எதிர்பார்ப்பை அமைக்கவும்: இறுதி நடவடிக்கை இருக்கும் குறைக்கப்பட்டது (ரேடியோலூனட் மூட்டு பாதுகாக்கப்படுகிறது; midcarpal மூட்டு உருகியுள்ளது)
நிர்வாகம் - காயம்: பரிந்துரைப்படி அறுவை சிகிச்சை பாண்டேஜ்கள்; ~1014 நாட்களுக்கு கனமான பாண்டேஜ் / ஸ்பிளின்ட், பின்னர் குறுகிய கை நடிப்பு அல்லது தெர்மோபிளாஸ்டிக் ஸ்பிளின்ட்; தொற்றுநோயைக் கண்காணிக்கவும் - வீக்கம்: இதய மட்டத்திற்கு மேலே உயர்வு, மென்மையான கை பம்ப், தேவைக்கேற்ப பனி - பயிற்சிகள்: முழு செயலில் உள்ள விரல், கட்டைவிரல் மற்றும் MCP/IP ROM; முதுகெலும்பு உச்சரிப்பு/சூபினேஷன்; மென்மையான தோள்பட்டை மற்றும் முழங்கை ROM; மணிக்கட்டு இயக்கம் இல்லை
முன்னேற்றத்திற்கான அளவுகோல்கள் - அறுவை சிகிச்சையாளரால் உறுதிப்படுத்தப்பட்ட ரேடியோகிராஃபிக் சங்கம் காயம் குணமடைந்தது; வீக்கம் கட்டுப்படுத்தப்பட்டது
கட்டம் II மணிக்கட்டு இயக்கத்தை மீட்டெடுப்பது (இணைப்பிலிருந்து, ~68 முதல் 12 வாரங்கள் வரை)
அறுவை சிகிச்சை நிபுணர் இணைப்பு திடமானது என்பதை உறுதிப்படுத்தியவுடன், மணிக்கட்டு அறுவை சிகிச்சையிலிருந்து வெளியேறுகிறது மற்றும் மெல்லிய மணிக்கட்டு இயக்கம் தொடங்குகிறது. முன்னேற்றம் படிப்படியானது; உருகிய பகுதி நகராது என்பதையும், அடையக்கூடிய வளைவு முன்பை விட சிறியது என்பதையும் நோயாளிக்கு நினைவூட்டப்படுகிறது.
உங்கள் கை சிகிச்சையாளருக்கு:
மதிப்பீடுகள் - மணிக்கட்டு செயலில் மற்றும் செயலற்ற ROM (வளைவு / நீட்டிப்பு, ரேடியல் / அல்னார் விலகல்), முதுகெலும்பு சுழற்சி, பிடியின் அடிப்படை, வலி மற்றும் வீக்கம், காயம் / ஸ்கார் ஆய்வு
கல்வி மற்றும் முன்னெச்சரிக்கைகள் - தொடங்கு சுறுசுறுப்பான மற்றும் சுறுசுறுப்பான உதவியுடன் மணிக்கட்டு ROM ஆறுதலுடன்; அமர்வுகளுக்கு இடையில் ஆறுதல்/பாதுகாப்பிற்காக அகற்றக்கூடிய மணிக்கட்டு அடுக்குக்கு மாற்றம் - கனமான கைப்பிடிப்பு, சுமைகளை தூக்குதல் மற்றும் சுமைகளை சுமப்பதைத் தவிர்க்கவும் வலுவூட்டலுக்காக அழிக்கப்படும் வரை மணிக்கட்டில் - வலுப்படுத்தவும் குறைக்கப்பட்ட இயக்கம் எதிர்பார்ப்பு (இலக்கு ~5065% எதிர் பக்க வளைவு வளைவு வளைவு வளைவு வளைவு)
நிர்வாகம் - உடற்பயிற்சிகள்ஃ சுறுசுறுப்பான/சுறுசுறுப்பான உதவியுடன் மணிக்கட்டு வளைவு, நீட்டிப்பு, ரேடியல் மற்றும் அல்னார் விலகல்; தொடங்குதல் ஸ்கார் மசாஜ் மற்றும் உணர்திறன் குறைப்பு காயம் முழுமையாக குணமடைந்தவுடன்; முழு விரல் / கட்டைவிரல் ROM மற்றும் முதுகெலும்பு சுழற்சியைத் தொடரவும்; தேவைக்கேற்ப வீக்கம் மேலாண்மை
முன்னேற்றத்திற்கான அளவுகோல்கள் - எதிர்பார்த்த குறைந்த வரம்பிற்குள் வசதியான, கட்டுப்படுத்தப்பட்ட மணிக்கட்டு வளைவு; வலி குறைப்பு; வலுவூட்டலுக்கான அறுவை சிகிச்சை அனுமதி
கட்டம் III வலுவூட்டல் மற்றும் செயல்பாட்டுக்கு திரும்புதல் (~12 வாரங்களில் இருந்து)
உருகும் திடப்பொருள் மற்றும் இயக்கம் அதன் பயனுள்ள உச்சவரம்பிற்கு மீட்டெடுக்கப்பட்டவுடன், வலுவூட்டல் மற்றும் படிப்படியான சுமை தொடங்குகிறது மற்றும் வாரங்களுக்குள் கட்டமைக்கப்படுகிறது. கை வேலை மற்றும் விளையாட்டுக்கு திரும்புவது அளவுகோல் அடிப்படையிலானது.
உங்கள் கை சிகிச்சையாளருக்கு:
மதிப்பீடுகள் - மற்ற பக்கத்துடன் ஒப்பிடும்போது பிடிப்பு மற்றும் பிஞ்ச் வலிமை; சுமைக்கு வலி / வீக்கம் பதில்; பணி மற்றும் வேலை-குறிப்பிட்ட செயல்பாட்டு சோதனை
கல்வி மற்றும் முன்னெச்சரிக்கைகள் - தொடங்கு படிப்படியான பிடிப்பு மற்றும் மணிக்கட்டு வலுவூட்டல் (கட்டி, பந்து, பின்னர் தரப்படுத்தப்பட்ட எதிர்ப்பு) ஒருமுறை அழிக்கப்பட்டது - அறிமுகம் சுமை மற்றும் எடை தாங்கி பணிகளை படிப்படியாக; ஒரே நேரத்தில் பல வாரங்களில் உருவாக்கப்படுவதை விட - எதிர்பார்க்கப்படும் இறுதி புள்ளிஃ பிடியில் மீட்பு நோக்கி ~70–80% மற்ற பக்க மற்றும் ஒரு பயனுள்ள, வலி இல்லாத, குறைக்கப்பட்ட வில்
நிர்வாகம் - உடற்பயிற்சிகள்ஃ படிப்படியான பிடிப்பு மற்றும் முதுகெலும்பு / மணிக்கட்டு வலுவூட்டல்; படிப்படியான செயல்பாட்டு மற்றும் வேலை உருவகப்படுத்துதல்; தொடர்ச்சியான வடுக்கள் மேலாண்மை மற்றும் ROM பராமரிப்பு - நீட்டிப்பில் முதுகெலும்பு மணிக்கட்டு வலி நீடித்தால், அறுவை சிகிச்சை நிபுணரிடம் சென்று ஆலோசனை பெறுங்கள். முதுகுத் தாக்கம்), சந்தேகம் தொழிற்சங்கம் இல்லாத, அல்லது மீட்பு சமவெளி - நோயாளியின் அன்றாட மற்றும் தொழில் தேவைகளுக்கு வலிமை மற்றும் செயல்பாடு போதுமானதாக இருக்கும்போது வெளியேற்றத்தை பரிசீலிக்கவும்
சுமைக்கு / வேலைக்கு திரும்புவதற்கான அளவுகோல்கள் - திடமான ஒருங்கிணைந்த இணைப்பு, மீட்டெடுக்கப்பட்ட வட்டத்திற்குள் வலி இல்லாதது, பணிக்கான போதுமான பிணைப்பு; கனமான கையேடு கோரிக்கைகள் ~ 46 மாதங்கள் வரை ஒத்திவைக்கப்பட்டு தரப்படுத்தப்பட்டன
வேலை மற்றும் செயற்பாட்டிற்கு திரும்புதல்
சுலபமான அன்றாட கை பயன்பாடு (உண்ணல், எழுதுதல், சுய-பராமரிப்பு) தொடக்கத்திலிருந்தே ஊக்குவிக்கப்படுகிறது, அது மார்பகத்தை சுமக்கவோ அல்லது திருகவோ செய்யாத வரை, அது வசதியாக இருக்கும். உங்கள் மார்பகத்தில் ஒரு மார்பகத்தில் இருக்கும்போது அல்லது சக்கரத்தை பாதுகாப்பாக கட்டுப்படுத்த முடியாதபோது நீங்கள் ஓட்டக்கூடாது என்பதால், ஆரம்ப வாரங்களில் போக்குவரத்து உதவிக்கு திட்டமிடவும்; நீங்கள் மார்பகத்திலிருந்து வெளியேறி, காரை நம்பிக்கையுடன் கட்டுப்படுத்த முடியும், உங்கள் மதிப்பாட்டில் உறுதிப்படுத்தப்பட்டபடி.
கைப்பிடி, தூக்குதல் மற்றும் சுமை சுமத்தல் ஆகியவை இணைவு திடமாக உறுதிப்படுத்தப்படும் வரை காத்திருக்க வேண்டும் (பொதுவாக ஆறு முதல் எட்டு வாரங்களுக்குப் பிறகு) பின்னர் படிப்படியாக கட்டமைக்கப்படுகின்றன. மேசை அடிப்படையிலான அல்லது ஒளி வேலை கொண்டவர்கள் பெரும்பாலும் சுமார் மூன்று மாதங்களில் திரும்புகிறார்கள்; கனமான கையேடு வேலை பொதுவாக நான்கு முதல் ஆறு மாதங்களுக்கு நெருக்கமாக உள்ளது மற்றும் கட்டங்களாக மீண்டும் அறிமுகப்படுத்தப்படுகிறது. முழுவதும், திட்டமிடப்பட்ட விளைவு ஒரு வசதியான, பயனுள்ள மணிக்கட்டு, குறைந்த அளவிலான இயக்கத்துடன், மணிக்கட்டு எவ்வாறு உணர்கிறது மற்றும் செயல்படுகிறது என்பதன் அடிப்படையில், டாக்டர் ஹிர்பாரா மற்றும் உங்கள் கை சிகிச்சையாளர் வேகத்தை வழிநடத்துகிறார்கள், காலண்டர் மட்டும் அல்ல.
உங்கள் நெறிமுறை பிறகு
இந்த நெறிமுறை நடைமுறையின் பொதுவான மீட்பு ஆலோசனையுடன் இணைந்து செயல்படுகிறதுஃ அறுவை சிகிச்சைக்குப் பிந்தைய வலியை நிர்வகித்தல், காயம் பராமரிப்பு மற்றும் வடு மேலாண்மைமேலே கொடுக்கப்பட்டுள்ள படிப்படியான திட்டம், உங்கள் மணிக்கட்டு பகுதியளவு இணைந்த பிறகு வெளியிடப்பட்ட மறுவாழ்வு வழிகாட்டுதல்களை பிரதிபலிக்கிறது, மேலும் உங்கள் மணிக்கட்டு எவ்வாறு குணமடைகிறது மற்றும் முன்னேறுகிறது என்பதைப் பொறுத்து, உங்கள் தற்போதைய மீட்பு டாக்டர் ஹிர்பாரா மற்றும் உங்கள் கை சிகிச்சையாளரால் தனித்தனியாக வழிநடத்தப்படுகிறது.
Evidence & references
Partial Wrist Fusion — Procedure Outcomes & Post-operative Rehabilitation (Capitolunate / Four-Corner Arthrodesis with Scaphoid Excision)
Topic scope: post-operative rehabilitation after midcarpal partial wrist arthrodesis for scapholunate advanced collapse (SLAC) or scaphoid nonunion advanced collapse (SNAC). The index procedure here is a capitolunate fusion (the capitate fused to the lunate, usually with excision of the worn scaphoid); the closely related four-corner fusion (lunate–capitate– triquetrum–hamate) follows the same rehabilitation principles. This is a bony arthrodesis, so the rehabilitation is a union-gated pathway: the mid-wrist is immobilised until the fusion consolidates, after which a deliberately reduced wrist arc and grip are restored.
Defining principle of the rehab here: a partial wrist fusion is a motion-preserving salvage. The arthritic midcarpal surfaces are fused to abolish pain, while the radiolunate joint is intentionally preserved to retain movement. The construct that needs protecting is healing bone (plate, headless screws, staples or K-wires across the fusion), not a soft-tissue repair — so progression is gated by radiographic union, not a calendar. Counselling the patient that the planned end-point is a pain-free, functional wrist with a reduced arc (~50–65% of normal flexion–extension, ~70–80% grip) is itself part of the treatment: the reduced motion is the intended trade-off, not a failure. The two principal branch points are the fixation method (which sets the immobilisation window and union risk) and whether scaphoid excision was performed (standard in the SLAC/SNAC setting).
A. PROCEDURE OUTCOMES (capitolunate / four-corner fusion for SLAC–SNAC)
Partial wrist fusion is a well-established, durable salvage for the SLAC/SNAC wrist. The dominant debate is which motion-preserving salvage (four-corner / capitolunate fusion vs proximal row carpectomy), not whether to operate; both reliably relieve pain at the cost of some motion.
- Reliable pain relief with a useful but reduced arc. Across series, midcarpal fusion abolishes the painful midcarpal arthritis while preserving radiolunate motion. Typical results are roughly 50–65% of contralateral flexion–extension and ~70–80% of contralateral grip strength, with high rates of pain relief and return to work — the expected, planned trade-off of a partial fusion [Enna Hand Clin 2005; Strauch J Hand Surg Am 2011; Merrell J Hand Surg Am 2008; long-term series J Wrist Surg 2015]. Moderate (cohort/consensus).
- Capitolunate fusion (± scaphoid excision) performs comparably to full four-corner fusion while fusing fewer joints, simplifying the construct. A systematic review of capitolunate arthrodesis and comparative work report comparable motion, grip and union to four-corner fusion, supporting it as a sound index choice [Dunn J Hand Surg Am 2020 (systematic review); lunocapitate series J Hand Surg Eur 2009; J Chin Med Assoc 2017]. Moderate.
- A meta-analysis of two-, three- and four-corner constructs finds the number of fused columns does not materially change motion, grip, union or complications — biomechanically consistent with the radiolunate joint being the motion-determining segment [Hundepool J Hand Surg Am 2025 (SR/meta-analysis); Hernandez-Soria J Hand Surg Am 2016 (capitate-position biomechanics)]. Moderate (SR) + mechanistic.
- Modern fixation is forgiving but union is not guaranteed. Circular dorsal plates, headless compression screws and nitinol staples all achieve consolidation in the great majority, with nonunion and dorsal impingement the characteristic failures to watch for [Merrell J Hand Surg Am 2008 (circular plate); Ahmady J Hand Surg Glob Online 2025 (nitinol staples)]. Moderate.
B. REHABILITATION / THERAPY EVIDENCE
The rehab questions are (1) how long to immobilise, (2) what gates the start of wrist motion, and (3) how to set the patient's expectation of reduced motion. The evidence and published surgeon protocols converge on a union-gated sequence: immobilise the wrist (mobilise the hand and forearm) for ~6–8 weeks, then restore a reduced arc, then strengthen.
- Immobilise until radiographic union, not by the calendar. Because the construct is bony, wrist motion is withheld until the surgeon confirms consolidation — typically 6–8 weeks, longer with some screw/staple fixations. Published institutional protocols use a bulky dressing/splint for ~10–14 days, a short-arm cast to ~4–6 weeks, then a removable splint as motion begins. Moderate (consensus protocols).
- Keep the hand and forearm fully mobile from day one. Immediate active finger, thumb and forearm rotation prevents stiffness and tendon adhesion without disturbing the fusion — the same glide-preserving logic used across hand rehab. Consensus.
- Restore motion gradually after union, against a realistic ceiling. Once united, active and active-assisted wrist ROM is introduced; patients should be counselled that the fused midcarpal segment will not move and the achievable arc is smaller than pre-operatively (the radiolunate joint alone supplies wrist motion). Consensus + mechanistic (capitate-position biomechanics, Hernandez-Soria 2016).
- Strengthen and load only once the fusion is solid. Grip and loaded/weight-bearing work begins after union and is built up gradually; heavy manual demands are deferred to ~4–6 months. Consensus.
Recovery trajectory (expected, evidence-anchored)
| Phase | Window | Restraint | Hand use / therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Immobilisation (union) | Week 0 to ~6–8 | Wrist immobilised (cast/splint) | Full active finger, thumb & forearm motion; oedema control, elevation; no wrist motion | None through the wrist | Fusion knits like a fracture; progress is gated by radiographic union, not the calendar |
| II — Restoring wrist motion | From union (~wk 6–8) to 12 | Heavy-load avoidance; removable splint | Begin active/active-assisted wrist flexion/extension & deviation; scar massage once healed | No loaded grip yet | Counsel the reduced-arc expectation (~50–65% of normal flexion–extension) |
| III — Strengthening & return | From ~12 weeks (post-union) | Restrictions lifted progressively | Progressive grip/wrist strengthening; graded job simulation | Grip recovers toward ~70–80% of the other side | Desk work ~3 months; heavy manual ~4–6 months. Watch for dorsal impingement / nonunion |
(Phase windows mirror the precautions in the patient protocol and published surgeon protocols; they are typical guides anchored to union, not trial-derived deadlines.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY
- Capitolunate vs four-corner vs proximal row carpectomy (PRC). All three are accepted motion-preserving salvages for SLAC/SNAC. PRC tends to give a slightly larger arc and avoids fusion-specific complications (nonunion, dorsal impingement, hardware), while fusion may give marginally better grip and is preferred where capitate-head or proximal-capitate cartilage is compromised. Systematic reviews and a meta-analysis find no consistent superiority of one over the other; choice is individualised [Mulford J Hand Surg Eur 2009; J Hand Surg Am 2024 meta-analysis; Strauch J Hand Surg Am 2011]. Moderate (SR/meta-analysis of mostly observational data).
- Capitolunate vs full four-corner construct. Fusing fewer columns (capitolunate) simplifies the construct without clearly compromising motion, grip or union versus four-corner — consistent with the radiolunate joint being the motion-determining segment [Dunn 2020 SR; Hundepool 2025 meta-analysis; Hernandez-Soria 2016]. Moderate.
- When can wrist motion safely start? Union timing varies with fixation, and protocols differ on exact cast duration. The defensible position is surgeon-confirmed radiographic union gates wrist ROM rather than a fixed week number. Weak–moderate (consensus; protocol variation).
- Reduced motion is the plan, not a complication. The preserved radiolunate joint supplies a smaller arc by design; mislabelling the expected ~50–65% range as a poor result drives unnecessary dissatisfaction. Strong mechanistically; cohort-supported.
- Characteristic failures: nonunion and dorsal impingement. Both are recognised, fixation-related complications; persistent dorsal wrist pain on extension or a non-progressing fusion warrants surgical review rather than more therapy [Merrell 2008; Ahmady 2025; long-term series 2015]. Moderate.
D. EVIDENCE STRENGTH FLAGS (summary)
- STRONG (mechanistic / well-supported): the reduced final arc is the planned consequence of preserving the radiolunate joint while fusing the midcarpal segment (capitate-position biomechanics); reliable pain relief from the fusion.
- MODERATE: typical outcome envelope (~50–65% flexion–extension, ~70–80% grip); equivalence of capitolunate and four-corner constructs; no consistent superiority of fusion vs PRC (SR/meta-analysis of largely observational data); modern fixation achieves high union with defined nonunion / dorsal impingement risk.
- WEAK / CONSENSUS: the specific union-gated immobilise → restore-motion → strengthen therapy sequence and exact phase timings (institutional/surgeon protocols, anchored to radiographic union rather than trial-derived).
CITATIONS
RAG corpus (180,000+ Orthopaedic articles)
- Enna M, Hoepfner P, Weiss AC. Scaphoid excision with four-corner fusion. Hand Clin. 2005. DOI: 10.1016/j.hcl.2005.08.012
- Dunn JC, Polmear MM, Scanaliato JP, et al. Capitolunate arthrodesis: a systematic review. J Hand Surg Am. 2020. DOI: 10.1016/j.jhsa.2019.10.007
- Hundepool CA, Duraku LS, Quanjel TJ, et al. Two-, three-, or four-corner arthrodesis for midcarpal osteoarthritis: a systematic review and meta-analysis. J Hand Surg Am. 2025. DOI: 10.1016/j.jhsa.2023.04.018
- Strauch RJ. Scapholunate advanced collapse and scaphoid nonunion advanced collapse arthritis — update on evaluation and treatment. J Hand Surg Am. 2011. DOI: 10.1016/j.jhsa.2011.01.018
- Merrell GA, McDermott EM, Weiss AC. Four-corner arthrodesis using a circular plate and distal radius bone grafting: a consecutive case series. J Hand Surg Am. 2008. DOI: 10.1016/j.jhsa.2008.02.001
- Hernandez-Soria A, Das De S, Model Z, et al. The effect of capitate position on coronal plane wrist motion after simulated 4-corner arthrodesis. J Hand Surg Am. 2016. DOI: 10.1016/j.jhsa.2016.07.101
- Ahmady AA, Zalzaleh M, Riedel BB. Midterm outcomes of four-corner fusion surgery using nitinol staples. J Hand Surg Glob Online. 2025. DOI: 10.1016/j.jhsg.2025.100805
- Mulford JS, Ceulemans LJ, Nam D, Axelrod TS. Proximal row carpectomy vs four corner fusion for scapholunate (SLAC) or scaphoid nonunion advanced collapse (SNAC) wrists: a systematic review of outcomes. J Hand Surg Eur Vol. 2009. DOI: 10.1177/1753193408100954
- Four-corner fusion versus proximal row carpectomy for scapholunate advanced collapse and scaphoid nonunion advanced collapse wrist: a systematic review and meta-analysis. J Hand Surg Am. 2024. DOI: 10.1016/j.jhsa.2024.01.011
- Long-term results of lunocapitate arthrodesis with scaphoid excision for SLAC and SNAC wrists. J Hand Surg Eur Vol. 2009. DOI: 10.1177/1753193409105683
- Lunocapitate fusion with scaphoid excision for the treatment of scaphoid nonunion advanced collapse or scapholunate advanced collapse wrist. J Chin Med Assoc. 2017. DOI: 10.1016/j.jcma.2016.10.001
- The long-term outcome of four-corner fusion. J Wrist Surg. 2015. DOI: 10.1055/s-0035-1549277
Partial wrist fusion rehabilitation literature (protocols & guidance — basis for the union-gated phase structure)
- University of Virginia Department of Orthopaedic Surgery. Wrist Partial Fusion (4-Corner) Rehabilitation Guidelines. https://med.virginia.edu/orthopaedic-surgery/wp-content/uploads/sites/242/2024/09/Wrist-Partial-Fusion-4-corner.pdf
- Oregon Health & Science University (OHSU). Four-Corner Partial Wrist Fusion — Surgery Guide. https://www.ohsu.edu/sites/default/files/2020-12/Four-Corner%20Partial%20Wrist%20Fusion.pdf
- Alaska Orthopedic Specialists. Four-Corner Fusion with Scaphoid Excision — Post-operative Protocol. https://www.akortho.com/wp-content/uploads/Four-Corner-Fusion-with-Scaphoid-Excision-1.pdf
- Twin Cities Orthopedics (Olson). Scaphoid Excision 4-Corner Fusion Post-operative Protocol. https://www.toportho.com/wp-content/uploads/2024/10/olson-_4-Corner-Fusion-Protocol.pdf
- The long-term outcome of four-corner fusion (open-access full text). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC4408128/





