部分腕关节融合术
Patients › Rehabilitation
腕关节部分融合术(通常是舟骨切除后的头月骨融合术)治疗磨损性腕关节损伤后的保护性康复计划:固定至骨骼愈合(约6~8周),随后逐步恢复实用但有意受限的腕关节活动范围及握力。
本方案指导您在部分腕关节融合术(一种切除磨损的舟骨并将腕部中间的小骨进行融合的手术,最常见的是头状骨与月骨之间的融合,即头月骨融合术)后由基兰·希尔帕拉(Kieran Hirpara)医生在罗克汉普顿 Mater 私人医院进行的康复过程。方案从您的家庭锻炼计划开始,随后是专为您的手部治疗师编写的结构化临床方案:请将此页面或其 PDF 文件带给您的首次治疗就诊,以确保您的康复过程协调一致。您的手部治疗师可能会根据您的康复进展调整计划。
如果您对术后伤口有任何疑虑,请联系诊所。拍摄伤口照片并发送电子邮件以供审查通常很有帮助。
预期情况
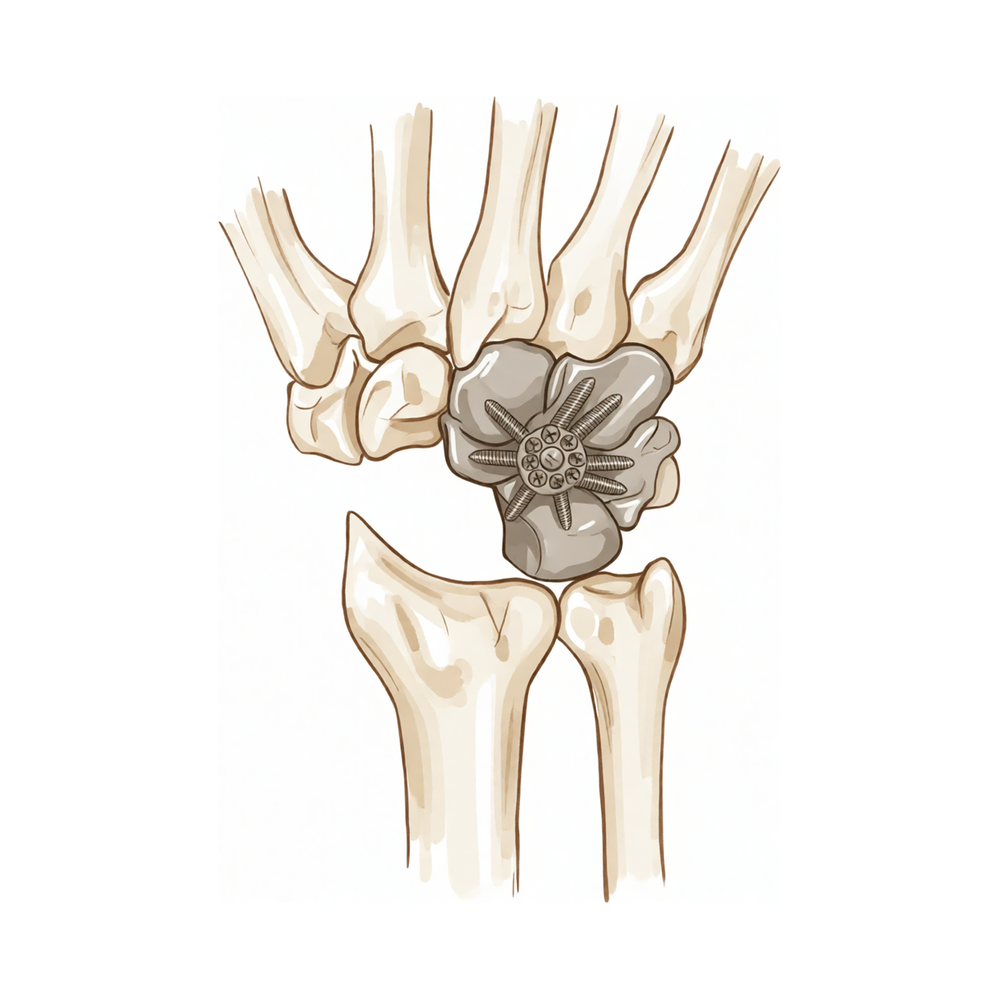
部分腕关节融合术用于治疗沿陈旧性舟骨病变路径发展的腕关节磨损(关节炎):即舟月韧带损伤(“SLAC”腕)或未愈合的陈旧性舟骨骨折(“SNAC”腕)。受损的舟骨被切除,腕中部的骨骼被融合在一起,使其不再相互摩擦。Hirpara 医生最常进行头状骨与月骨融合(头月融合),有时包括邻近骨骼;当月骨、头状骨、三角骨和钩骨全部融合时,称为四角融合,其康复原则相同。
该手术的关键理念是仅融合腕关节的一部分,而非全部。月骨与前臂骨(桡骨)之间的关节被刻意保留。正是这个保留的关节使腕关节能够继续活动:
- 融合磨损表面可消除疼痛: 这是主要目标,且可可靠实现。
- 保留桡月关节意味着保留有用活动度。 代价是活动度减少:大多数人最终保留约原来屈曲范围的一半至三分之二,握力约为对侧的四分之三。这是正常且预期的结果(而非并发症),对于疼痛且磨损的腕关节而言,这通常是非常值得的交换。
融合后的骨骼需要时间牢固愈合,就像骨折一样。在最初六至八周内,腕关节在石膏或夹板固定下保持静止,以便愈合。在此期间,手指、拇指和前臂保持自由活动,但腕关节本身得到休息。一旦外科医生通过 X 线确认骨骼已愈合,腕关节活动度及随后的力量训练将分阶段谨慎开展。早期建立合理预期(获得一个舒适、有用的腕关节,而非完全灵活的腕关节)是康复的重要组成部分。
注意事项与限制
- 在您的外科医生确认融合已愈合之前(通常为六至八周),请保持手腕在石膏或夹板中静止不动:手腕活动前,骨骼必须完成愈合。
- 从第一天起,请保持手指、拇指和前臂活动,但在获得许可前,切勿活动手腕本身。
- 在确认融合牢固之前,切勿用力握持、提举、推动、拉动或通过手腕承重:这有助于保护愈合中的骨骼以及任何钢板、螺钉或钉合装置。
- 预期最终活动范围会减小:这是部分腕关节融合术的预期结果,而非出现问题的迹象。
- 保持石膏或敷料清洁干燥,在佩戴石膏或无法安全控制方向盘期间,切勿驾驶车辆。
有关伤口、肿胀和瘢痕管理,请参阅诊所的伤口护理指南。
您的练习
这些是您讲义中的练习。仅在 Hirpara 医生和您的手部治疗师的指导下开始练习,并严格遵循您被给予的活动范围和限制。早期练习旨在保持手指、拇指和前臂的活动,同时不干扰愈合中的骨融合;腕关节本身在石膏或夹板固定下保持静止。腕关节活动和握力强化属于后期阶段,必须在您的外科医生确认骨骼愈合后才能开始。如果腕部出现尖锐疼痛,请立即停止任何相关动作。
您的临床方案
本页面其余部分为部分腕关节融合术(头状骨-月骨融合 ± 舟骨切除术;四角融合术遵循相同原则)后的分阶段康复临床方案。本节内容旨在提供给您的手治疗师,每个阶段均以通俗语言解释当前的治疗目标。与肌腱修复不同,此处的固定结构为骨性结构,进展取决于融合处的影像学骨性愈合,而非固定的日历时间。在外科医生确认骨性愈合之前,腕关节需保持制动,仅活动手指、拇指和前臂;此后逐步恢复腕关节活动度,最后恢复负重,其功能上限大致为对侧腕关节屈伸活动度的 50–65%,握力约为 70–80%。
治疗前,请查阅患者的手术记录,确认使用的固定方式(环形/背侧钢板、空心加压螺钉、 staples 或克氏针)以及是否进行了舟骨切除术。在治疗医师确认影像学骨性愈合之前(通常为 6–8 周,使用螺钉或 staples 固定时可能更长),切勿开始腕关节活动。从首次就诊起即应向患者说明,治疗目标是一个无痛且功能良好的腕关节,其活动弧是有意受限的,而非完全的活动自如。
第一阶段——保护性固定直至骨性愈合(第0周至约6–8周)
融合过程类似于骨折愈合,因此在骨骼连接期间需保持腕关节静止。手部及前臂需保持完全活动,以防止僵硬和肌腱粘连,但腕关节不得活动。
致手治疗师:
教育与注意事项 - 腕关节在石膏或夹板中固定,直至外科医生确认影像学上的骨性愈合(通常为6–8周) - 此阶段禁止主动或被动腕关节活动 - 禁止通过患侧腕关节进行抓握、提举、推、拉或负重 - 早期建立预期:最终活动度将降低(桡月关节得以保留;中腕关节已融合)
管理措施 - 伤口:按医嘱更换手术敷料;术后约10–14天使用厚敷料/夹板,随后改为短臂石膏或热塑夹板;监测感染迹象 - 水肿:抬高至心脏水平以上,进行轻柔的手部泵血运动,必要时冰敷 - 锻炼:手指、拇指及掌指/指间关节的完全主动活动范围(ROM);前臂旋前/旋后;肩肘关节轻柔活动范围(ROM);禁止腕关节活动
进阶标准 - 外科医生确认影像学骨性愈合(不可仅依据日历时间而进阶);伤口愈合;肿胀得到控制
第二阶段——恢复腕关节活动度(从骨性愈合开始,约第6–8周至12周)
一旦外科医生确认融合牢固,腕关节将取出石膏,并开始轻柔的腕关节活动。进展是渐进的;需提醒患者,融合部分将不会活动,且可实现的关节活动弧小于术前。
供您的手部治疗师参考:
评估 - 腕关节主动和被动关节活动度(屈曲/伸展,桡偏/尺偏),前臂旋转,握力基线,疼痛和肿胀,伤口/瘢痕复查
教育和注意事项 - 在舒适范围内开始腕关节主动和主动辅助活动;在疗程之间过渡至使用可拆卸腕部夹板以提供舒适/保护 - 继续避免通过腕关节进行用力抓握、负重提物和承重,直至获得加强训练的许可 - 强化活动度受限的预期(目标为对侧屈伸活动弧的约50–65%)
管理 - 练习:腕关节主动/主动辅助屈曲、伸展、桡偏和尺偏;伤口完全愈合后开始瘢痕按摩和脱敏;继续全手指/拇指关节活动度和前臂旋转;根据需要管理水肿
进展标准 - 在预期的受限范围内,腕关节活动弧舒适且可控;疼痛缓解;获得外科医生关于加强训练的许可
第三阶段——强化与功能恢复(约12周起)
随着骨融合牢固且活动度恢复至实用上限,开始进行强化训练和分级负荷,并在数周内逐步增加。重返体力劳动和运动以达标为依据。
供您的手部治疗师参考:
评估 - 与健侧对比的握力和捏力;负荷下的疼痛/肿胀反应;任务及职业特异性功能测试
教育与注意事项 - 获得许可后,开始渐进性握力和腕部强化训练(使用治疗泥、球类,随后进行分级阻力训练) - 逐步引入负重和承重任务;在数周内逐步增加,而非一次性完成 - 预期终点:握力恢复至健侧的约70–80%,且具备实用、无痛、活动范围减小的特点
管理 - 练习:渐进性抓握和前臂/腕部强化训练;分级功能及工作模拟;持续的瘢痕管理和活动度维持 - 若出现伸腕时持续性背侧腕部疼痛(可能为背侧撞击)、疑似骨不连或恢复平台期,需警惕并转诊回外科医生 - 一旦力量和功能满足患者日常及职业需求,可考虑出院
重返负荷/工作的标准 - 骨融合牢固,在恢复的活动范围内无痛,握力满足任务需求;重度体力劳动需求推迟至约4–6个月,并逐步增加
重返工作与活动
从开始阶段起,鼓励在舒适范围内进行日常手部轻度活动(如进食、书写、轻度自我护理),前提是不得对腕关节施加负荷或扭转。由于腕关节处于石膏固定或无法安全控制方向盘时不得驾驶,请在早期数周安排交通协助;待拆除石膏并经复查确认您可自信控制车辆后,方可恢复驾驶。
握持、提举及经腕关节负重需待骨性融合确认牢固(通常在约六至八周后)方可进行,并随后逐步增加。从事办公室工作或轻度劳动者通常在约三个月后返岗;较重的体力劳动通常在四至六个月左右,并分阶段逐步恢复。在整个过程中,请记住,预期结果是获得一个舒适且实用的腕关节,尽管其活动范围有所减少;评估标准基于腕关节的主观感受与功能表现,恢复节奏由Hirpara医生及您的手部治疗师根据临床情况指导,而非仅依据日历时间。
术后方案
本方案与诊所的一般康复建议并行:请参阅术后疼痛管理、伤口护理和疤痕管理。上述分阶段计划反映了腕关节部分融合术后的康复指南,您的持续康复将由Hirpara医生和您的手部治疗师根据您腕关节的愈合和进展情况个体化指导。
Evidence & references
Partial Wrist Fusion — Procedure Outcomes & Post-operative Rehabilitation (Capitolunate / Four-Corner Arthrodesis with Scaphoid Excision)
Topic scope: post-operative rehabilitation after midcarpal partial wrist arthrodesis for scapholunate advanced collapse (SLAC) or scaphoid nonunion advanced collapse (SNAC). The index procedure here is a capitolunate fusion (the capitate fused to the lunate, usually with excision of the worn scaphoid); the closely related four-corner fusion (lunate–capitate– triquetrum–hamate) follows the same rehabilitation principles. This is a bony arthrodesis, so the rehabilitation is a union-gated pathway: the mid-wrist is immobilised until the fusion consolidates, after which a deliberately reduced wrist arc and grip are restored.
Defining principle of the rehab here: a partial wrist fusion is a motion-preserving salvage. The arthritic midcarpal surfaces are fused to abolish pain, while the radiolunate joint is intentionally preserved to retain movement. The construct that needs protecting is healing bone (plate, headless screws, staples or K-wires across the fusion), not a soft-tissue repair — so progression is gated by radiographic union, not a calendar. Counselling the patient that the planned end-point is a pain-free, functional wrist with a reduced arc (~50–65% of normal flexion–extension, ~70–80% grip) is itself part of the treatment: the reduced motion is the intended trade-off, not a failure. The two principal branch points are the fixation method (which sets the immobilisation window and union risk) and whether scaphoid excision was performed (standard in the SLAC/SNAC setting).
A. PROCEDURE OUTCOMES (capitolunate / four-corner fusion for SLAC–SNAC)
Partial wrist fusion is a well-established, durable salvage for the SLAC/SNAC wrist. The dominant debate is which motion-preserving salvage (four-corner / capitolunate fusion vs proximal row carpectomy), not whether to operate; both reliably relieve pain at the cost of some motion.
- Reliable pain relief with a useful but reduced arc. Across series, midcarpal fusion abolishes the painful midcarpal arthritis while preserving radiolunate motion. Typical results are roughly 50–65% of contralateral flexion–extension and ~70–80% of contralateral grip strength, with high rates of pain relief and return to work — the expected, planned trade-off of a partial fusion [Enna Hand Clin 2005; Strauch J Hand Surg Am 2011; Merrell J Hand Surg Am 2008; long-term series J Wrist Surg 2015]. Moderate (cohort/consensus).
- Capitolunate fusion (± scaphoid excision) performs comparably to full four-corner fusion while fusing fewer joints, simplifying the construct. A systematic review of capitolunate arthrodesis and comparative work report comparable motion, grip and union to four-corner fusion, supporting it as a sound index choice [Dunn J Hand Surg Am 2020 (systematic review); lunocapitate series J Hand Surg Eur 2009; J Chin Med Assoc 2017]. Moderate.
- A meta-analysis of two-, three- and four-corner constructs finds the number of fused columns does not materially change motion, grip, union or complications — biomechanically consistent with the radiolunate joint being the motion-determining segment [Hundepool J Hand Surg Am 2025 (SR/meta-analysis); Hernandez-Soria J Hand Surg Am 2016 (capitate-position biomechanics)]. Moderate (SR) + mechanistic.
- Modern fixation is forgiving but union is not guaranteed. Circular dorsal plates, headless compression screws and nitinol staples all achieve consolidation in the great majority, with nonunion and dorsal impingement the characteristic failures to watch for [Merrell J Hand Surg Am 2008 (circular plate); Ahmady J Hand Surg Glob Online 2025 (nitinol staples)]. Moderate.
B. REHABILITATION / THERAPY EVIDENCE
The rehab questions are (1) how long to immobilise, (2) what gates the start of wrist motion, and (3) how to set the patient's expectation of reduced motion. The evidence and published surgeon protocols converge on a union-gated sequence: immobilise the wrist (mobilise the hand and forearm) for ~6–8 weeks, then restore a reduced arc, then strengthen.
- Immobilise until radiographic union, not by the calendar. Because the construct is bony, wrist motion is withheld until the surgeon confirms consolidation — typically 6–8 weeks, longer with some screw/staple fixations. Published institutional protocols use a bulky dressing/splint for ~10–14 days, a short-arm cast to ~4–6 weeks, then a removable splint as motion begins. Moderate (consensus protocols).
- Keep the hand and forearm fully mobile from day one. Immediate active finger, thumb and forearm rotation prevents stiffness and tendon adhesion without disturbing the fusion — the same glide-preserving logic used across hand rehab. Consensus.
- Restore motion gradually after union, against a realistic ceiling. Once united, active and active-assisted wrist ROM is introduced; patients should be counselled that the fused midcarpal segment will not move and the achievable arc is smaller than pre-operatively (the radiolunate joint alone supplies wrist motion). Consensus + mechanistic (capitate-position biomechanics, Hernandez-Soria 2016).
- Strengthen and load only once the fusion is solid. Grip and loaded/weight-bearing work begins after union and is built up gradually; heavy manual demands are deferred to ~4–6 months. Consensus.
Recovery trajectory (expected, evidence-anchored)
| Phase | Window | Restraint | Hand use / therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Immobilisation (union) | Week 0 to ~6–8 | Wrist immobilised (cast/splint) | Full active finger, thumb & forearm motion; oedema control, elevation; no wrist motion | None through the wrist | Fusion knits like a fracture; progress is gated by radiographic union, not the calendar |
| II — Restoring wrist motion | From union (~wk 6–8) to 12 | Heavy-load avoidance; removable splint | Begin active/active-assisted wrist flexion/extension & deviation; scar massage once healed | No loaded grip yet | Counsel the reduced-arc expectation (~50–65% of normal flexion–extension) |
| III — Strengthening & return | From ~12 weeks (post-union) | Restrictions lifted progressively | Progressive grip/wrist strengthening; graded job simulation | Grip recovers toward ~70–80% of the other side | Desk work ~3 months; heavy manual ~4–6 months. Watch for dorsal impingement / nonunion |
(Phase windows mirror the precautions in the patient protocol and published surgeon protocols; they are typical guides anchored to union, not trial-derived deadlines.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY
- Capitolunate vs four-corner vs proximal row carpectomy (PRC). All three are accepted motion-preserving salvages for SLAC/SNAC. PRC tends to give a slightly larger arc and avoids fusion-specific complications (nonunion, dorsal impingement, hardware), while fusion may give marginally better grip and is preferred where capitate-head or proximal-capitate cartilage is compromised. Systematic reviews and a meta-analysis find no consistent superiority of one over the other; choice is individualised [Mulford J Hand Surg Eur 2009; J Hand Surg Am 2024 meta-analysis; Strauch J Hand Surg Am 2011]. Moderate (SR/meta-analysis of mostly observational data).
- Capitolunate vs full four-corner construct. Fusing fewer columns (capitolunate) simplifies the construct without clearly compromising motion, grip or union versus four-corner — consistent with the radiolunate joint being the motion-determining segment [Dunn 2020 SR; Hundepool 2025 meta-analysis; Hernandez-Soria 2016]. Moderate.
- When can wrist motion safely start? Union timing varies with fixation, and protocols differ on exact cast duration. The defensible position is surgeon-confirmed radiographic union gates wrist ROM rather than a fixed week number. Weak–moderate (consensus; protocol variation).
- Reduced motion is the plan, not a complication. The preserved radiolunate joint supplies a smaller arc by design; mislabelling the expected ~50–65% range as a poor result drives unnecessary dissatisfaction. Strong mechanistically; cohort-supported.
- Characteristic failures: nonunion and dorsal impingement. Both are recognised, fixation-related complications; persistent dorsal wrist pain on extension or a non-progressing fusion warrants surgical review rather than more therapy [Merrell 2008; Ahmady 2025; long-term series 2015]. Moderate.
D. EVIDENCE STRENGTH FLAGS (summary)
- STRONG (mechanistic / well-supported): the reduced final arc is the planned consequence of preserving the radiolunate joint while fusing the midcarpal segment (capitate-position biomechanics); reliable pain relief from the fusion.
- MODERATE: typical outcome envelope (~50–65% flexion–extension, ~70–80% grip); equivalence of capitolunate and four-corner constructs; no consistent superiority of fusion vs PRC (SR/meta-analysis of largely observational data); modern fixation achieves high union with defined nonunion / dorsal impingement risk.
- WEAK / CONSENSUS: the specific union-gated immobilise → restore-motion → strengthen therapy sequence and exact phase timings (institutional/surgeon protocols, anchored to radiographic union rather than trial-derived).
CITATIONS
RAG corpus (180,000+ Orthopaedic articles)
- Enna M, Hoepfner P, Weiss AC. Scaphoid excision with four-corner fusion. Hand Clin. 2005. DOI: 10.1016/j.hcl.2005.08.012
- Dunn JC, Polmear MM, Scanaliato JP, et al. Capitolunate arthrodesis: a systematic review. J Hand Surg Am. 2020. DOI: 10.1016/j.jhsa.2019.10.007
- Hundepool CA, Duraku LS, Quanjel TJ, et al. Two-, three-, or four-corner arthrodesis for midcarpal osteoarthritis: a systematic review and meta-analysis. J Hand Surg Am. 2025. DOI: 10.1016/j.jhsa.2023.04.018
- Strauch RJ. Scapholunate advanced collapse and scaphoid nonunion advanced collapse arthritis — update on evaluation and treatment. J Hand Surg Am. 2011. DOI: 10.1016/j.jhsa.2011.01.018
- Merrell GA, McDermott EM, Weiss AC. Four-corner arthrodesis using a circular plate and distal radius bone grafting: a consecutive case series. J Hand Surg Am. 2008. DOI: 10.1016/j.jhsa.2008.02.001
- Hernandez-Soria A, Das De S, Model Z, et al. The effect of capitate position on coronal plane wrist motion after simulated 4-corner arthrodesis. J Hand Surg Am. 2016. DOI: 10.1016/j.jhsa.2016.07.101
- Ahmady AA, Zalzaleh M, Riedel BB. Midterm outcomes of four-corner fusion surgery using nitinol staples. J Hand Surg Glob Online. 2025. DOI: 10.1016/j.jhsg.2025.100805
- Mulford JS, Ceulemans LJ, Nam D, Axelrod TS. Proximal row carpectomy vs four corner fusion for scapholunate (SLAC) or scaphoid nonunion advanced collapse (SNAC) wrists: a systematic review of outcomes. J Hand Surg Eur Vol. 2009. DOI: 10.1177/1753193408100954
- Four-corner fusion versus proximal row carpectomy for scapholunate advanced collapse and scaphoid nonunion advanced collapse wrist: a systematic review and meta-analysis. J Hand Surg Am. 2024. DOI: 10.1016/j.jhsa.2024.01.011
- Long-term results of lunocapitate arthrodesis with scaphoid excision for SLAC and SNAC wrists. J Hand Surg Eur Vol. 2009. DOI: 10.1177/1753193409105683
- Lunocapitate fusion with scaphoid excision for the treatment of scaphoid nonunion advanced collapse or scapholunate advanced collapse wrist. J Chin Med Assoc. 2017. DOI: 10.1016/j.jcma.2016.10.001
- The long-term outcome of four-corner fusion. J Wrist Surg. 2015. DOI: 10.1055/s-0035-1549277
Partial wrist fusion rehabilitation literature (protocols & guidance — basis for the union-gated phase structure)
- University of Virginia Department of Orthopaedic Surgery. Wrist Partial Fusion (4-Corner) Rehabilitation Guidelines. https://med.virginia.edu/orthopaedic-surgery/wp-content/uploads/sites/242/2024/09/Wrist-Partial-Fusion-4-corner.pdf
- Oregon Health & Science University (OHSU). Four-Corner Partial Wrist Fusion — Surgery Guide. https://www.ohsu.edu/sites/default/files/2020-12/Four-Corner%20Partial%20Wrist%20Fusion.pdf
- Alaska Orthopedic Specialists. Four-Corner Fusion with Scaphoid Excision — Post-operative Protocol. https://www.akortho.com/wp-content/uploads/Four-Corner-Fusion-with-Scaphoid-Excision-1.pdf
- Twin Cities Orthopedics (Olson). Scaphoid Excision 4-Corner Fusion Post-operative Protocol. https://www.toportho.com/wp-content/uploads/2024/10/olson-_4-Corner-Fusion-Protocol.pdf
- The long-term outcome of four-corner fusion (open-access full text). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC4408128/





