Partial Wrist Fusion Info Evidence
Reviewed by Dr Kieran Hirpara, Specialist Orthopaedic Surgeon Last reviewed
This protocol guides your recovery after a partial wrist fusion (an operation that removes the worn-out scaphoid bone and fuses the small bones in the middle of the wrist, most often the capitate to the lunate in a capitolunate fusion) with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It begins with your home exercise program, followed by the structured clinical protocol written for your hand therapist: bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your hand therapist may adjust the plan depending on how your recovery progresses.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect
A partial wrist fusion treats a wrist that has worn out (arthritis) along the path that follows an old scaphoid problem: either a scapholunate ligament injury (a "SLAC" wrist) or an old scaphoid fracture that never healed (a "SNAC" wrist). The damaged scaphoid is removed, and the bones of the mid-wrist are fused together so they no longer rub. Dr Hirpara most often fuses the capitate to the lunate (a capitolunate fusion), sometimes including the neighbouring bones; when the lunate, capitate, triquetrum and hamate are all fused this is called a four-corner fusion, and it follows the same recovery principles.
The key idea behind this operation is that only part of the wrist is fused, not all of it. The joint between the lunate and the forearm bone (the radius) is deliberately left alone. That preserved joint is what allows the wrist to keep moving:
- Fusing the worn surfaces takes the pain away: that is the main goal, and it is reliably achieved.
- Keeping the radius–lunate joint means you keep useful movement. The trade-off is that the movement is reduced: most people end up with roughly half to two-thirds of their former bending range, and grip strength of about three-quarters of the other side. This is a normal, expected result (not a complication) and for a painful, worn wrist it is usually a very worthwhile exchange.
The fused bones need time to knit solidly together, just like a fracture. For about the first six weeks the wrist is held still in a splint while this happens. During that time the fingers, thumb and forearm are kept moving freely, but the wrist itself is rested. Once the surgeon confirms on X-ray that the bones have united, wrist movement and then strengthening are opened up in careful stages. Setting your expectations early (a comfortable, useful wrist rather than a fully mobile one) is an important part of the recovery.
Precautions and limitations
- Keep your wrist still in its splint until your surgeon confirms the fusion has healed (usually about six weeks): the bones must knit before the wrist is moved.
- Keep your fingers, thumb and forearm moving from day one, but do NOT move the wrist itself until cleared.
- Do NOT grip hard, lift, push, pull or bear weight through the wrist until the fusion is confirmed solid: this protects the healing bone and any plate, screws or staples.
- Expect a reduced final range of movement: this is the planned result of fusing part of the wrist, not a sign anything has gone wrong.
- Keep the splint and dressing clean and dry, and do NOT drive while you are in the splint or cannot safely control the wheel.
For wound, swelling and scar management, see the practice's wound care guidance.
Your exercises
Kieran Hirpara 4.0
Finger and thumb movement
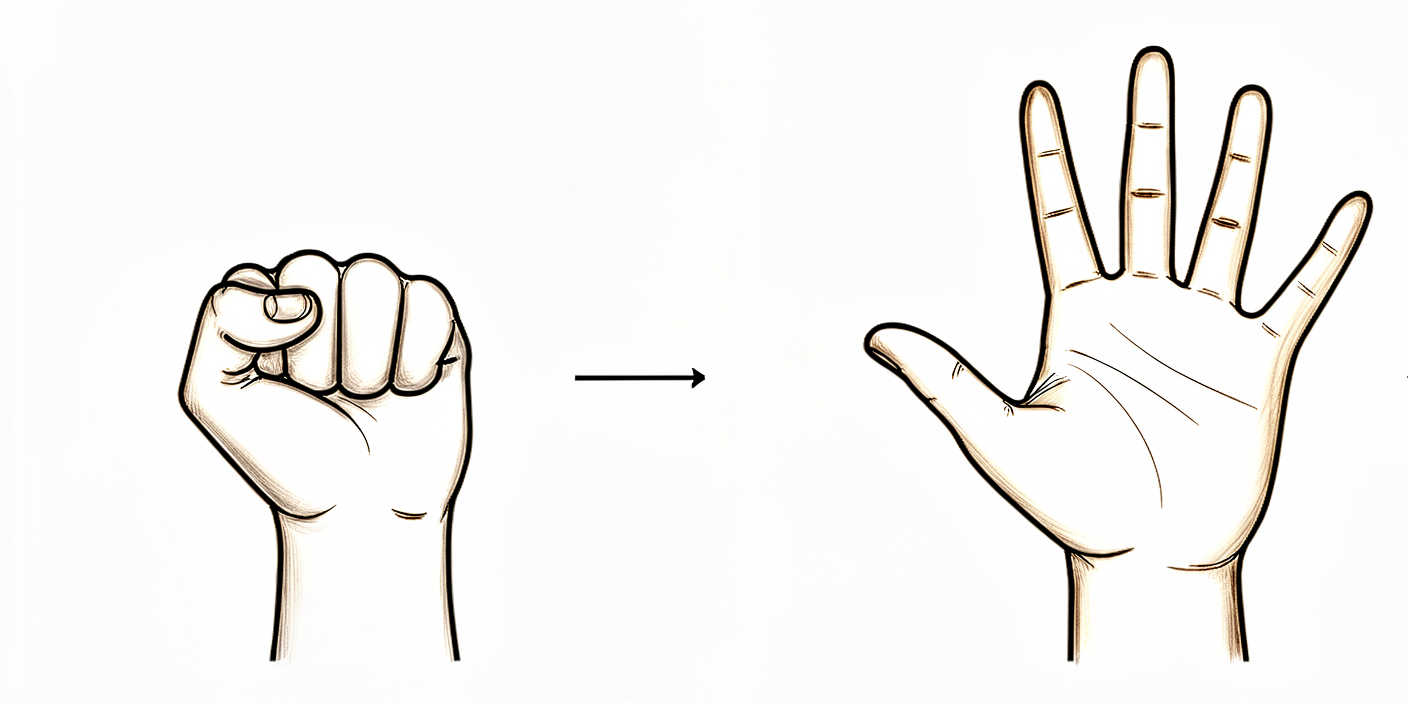
From the day of surgery, keep your fingers and thumb moving while the wrist itself rests in the cast or splint. Fully straighten all your fingers, then make a complete fist, then touch your thumb to the tip of each finger in turn. This stops the hand stiffening and keeps the tendons gliding while the wrist bones knit together. Do not move the wrist itself.
10 times each, several times a day, every day from the start
Kieran Hirpara 4.0
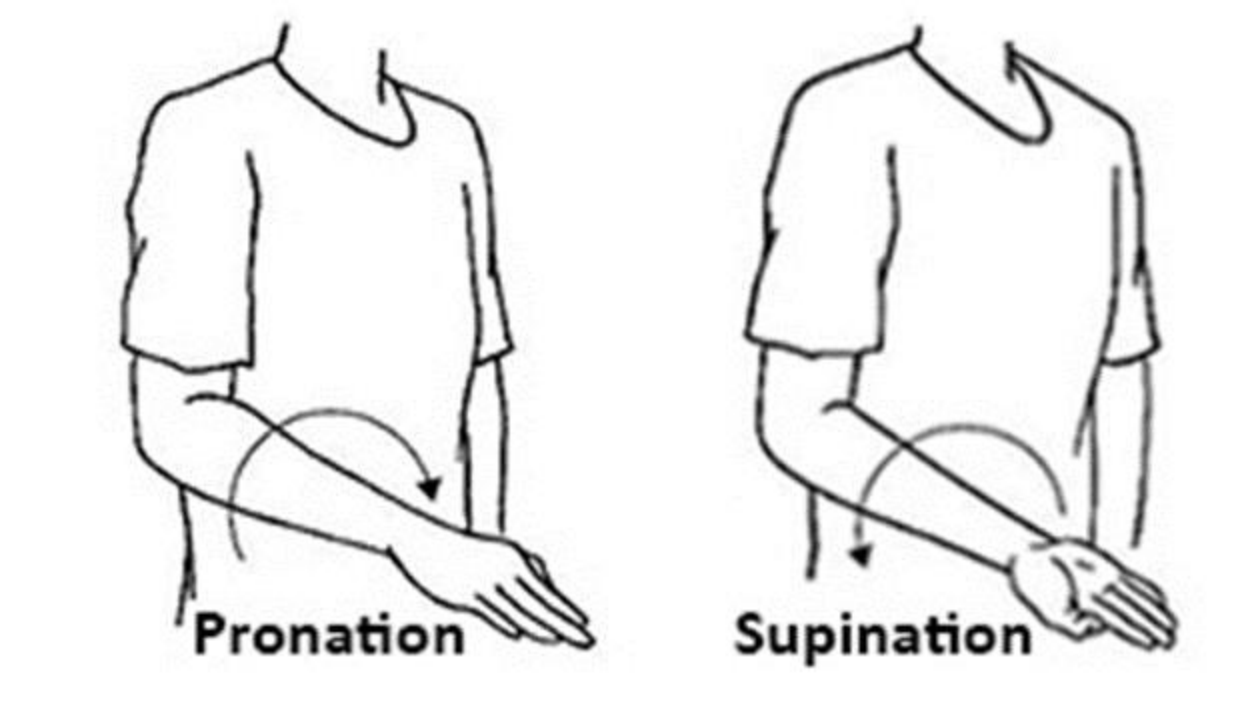
Forearm rotation (palm up / palm down)
With your elbow tucked in at your side and bent to a right angle, gently turn your palm up to face the ceiling, then down to face the floor. Keep the movement coming from the forearm, not the wrist. This keeps the forearm supple and does not disturb the healing fusion, so it can begin straight away.
10 times each direction, 2–3 times a day
Kieran Hirpara 4.0
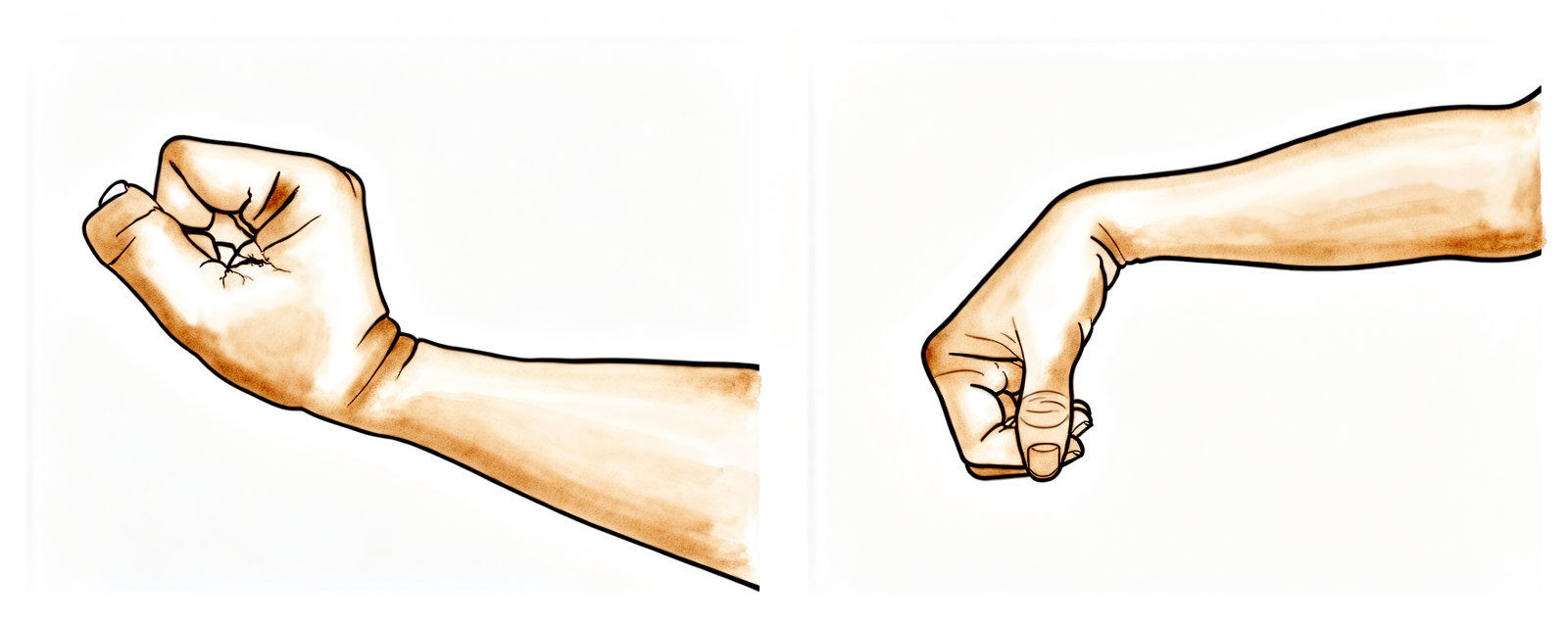
Wrist movement (after union)
A LATER exercise — only once the fusion has healed and your surgeon and hand therapist have cleared wrist movement (usually after about six to eight weeks). Gently bend the wrist up (back) and down (forwards), then tilt it towards the thumb and towards the little finger, moving only as far as is comfortable. Remember the fused part of the wrist will not move — you are restoring the movement that comes from the preserved joint, so the final range will be smaller than before, and that is expected.
10 times in each direction, 2–3 times a day, within comfort (after union)
Kieran Hirpara 4.0
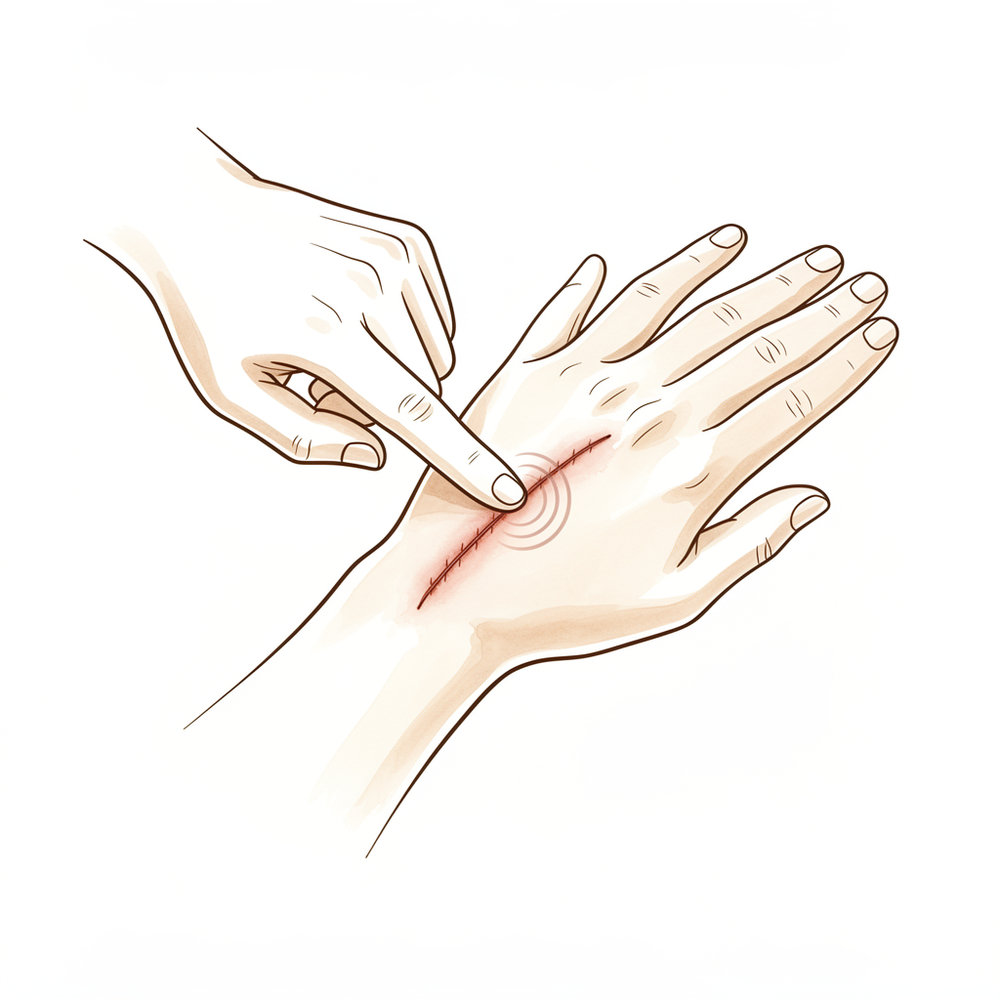
Scar care
Once the wound is fully healed and dry, massage the scar with a little non-perfumed moisturiser, using small firm circles with the opposite thumb for a couple of minutes. This softens the scar and reduces sensitivity. Do not start until the wound has sealed and your therapist is happy.
2–3 minutes, twice a day, once the wound is healed

Kieran Hirpara 4.0
Grip strengthening
A LATER exercise — begun only once the fusion is solid and strengthening has been cleared (usually from around eight to twelve weeks). Squeeze a soft ball or therapy putty in the palm, hold briefly, then release. Build the effort up gradually over several weeks. Heavy gripping, lifting and weight-bearing through the wrist are held back until your surgeon confirms the bones are fully united.
10–15 squeezes, 2–3 times a day, building gradually (later phase)
These are the exercises from your handout. Start them only as guided by Dr Hirpara and your hand therapist, staying within whatever range and limits you have been given. The early exercises keep the fingers, thumb and forearm moving without disturbing the healing fusion; the wrist itself stays still in its cast or splint. Wrist movement and grip strengthening belong to later phases and should not be started until your surgeon has confirmed the bones have united. Stop anything that causes sharp pain over the wrist.
Your clinical protocol
The rest of this page is the staged clinical protocol for rehabilitation after a partial wrist fusion (capitolunate ± scaphoid excision; the same principles apply to four-corner fusion). This section is to be provided to your hand therapist, and each phase opens with a plain-English explanation of what is happening. Unlike a tendon repair, the construct here is bony, and progression is gated by radiographic union of the fusion, not by a fixed calendar. Until the surgeon confirms union, the wrist is immobilised and only the fingers, thumb and forearm are mobilised; thereafter wrist range and then load are restored, with a realistic ceiling of roughly 50–65% of contralateral flexion–extension and ~70–80% grip.
Prior to treatment, check the patient's operation report and confirm the fixation used (circular/dorsal plate, headless compression screws, staples or K-wires) and whether the scaphoid was excised. Do NOT initiate wrist motion until the treating surgeon confirms radiographic union (typically 6–8 weeks, sometimes longer with screw or staple fixation). Counsel the patient from the first visit that the goal is a pain-free, functional wrist with a deliberately reduced arc, not full mobility.
Phase I — protected immobilisation until union (weeks 0 to ~6–8)
The fusion is healing like a fracture, so the wrist is held still while the bones knit. The hand and forearm are kept fully mobile to prevent stiffness and tendon adhesion, but the wrist is not moved.
For your hand therapist:
Education and precautions - Wrist immobilised in a cast or splint until the surgeon confirms radiographic union (typically 6–8 weeks) - No active or passive wrist motion during this phase - No gripping, lifting, pushing, pulling or weight-bearing through the operated wrist - Set the expectation early: final motion will be reduced (the radiolunate joint is preserved; the midcarpal joint is fused)
Management - Wound: surgical dressings as directed; bulky dressing/splint for ~10–14 days, then short-arm cast or thermoplastic splint; monitor for infection - Oedema: elevation above heart level, gentle hand pumping, ice as needed - Exercises: full active finger, thumb and MCP/IP ROM; forearm pronation/supination; gentle shoulder and elbow ROM; no wrist motion
Criteria to progress - Radiographic union confirmed by the surgeon (do not progress on calendar alone); wound healed; swelling controlled
Phase II — restoring wrist motion (from union, ~weeks 6–8 to 12)
Once the surgeon confirms the fusion is solid, the wrist comes out of the cast and gentle wrist movement begins. Progress is gradual; the patient is reminded that the fused portion will not move and the achievable arc is smaller than before.
For your hand therapist:
Assessments - Wrist active and passive ROM (flexion/extension, radial/ulnar deviation), forearm rotation, grip baseline, pain and swelling, wound/scar review
Education and precautions - Begin active and active-assisted wrist ROM within comfort; transition to a removable wrist splint for comfort/protection between sessions - Continue to avoid heavy gripping, loaded lifting and weight-bearing through the wrist until cleared for strengthening - Reinforce the reduced-motion expectation (target ~50–65% of the contralateral flexion–extension arc)
Management - Exercises: active/active-assisted wrist flexion, extension, radial and ulnar deviation; commence scar massage and desensitisation once the wound is fully healed; continue full finger/thumb ROM and forearm rotation; oedema management as needed
Criteria to progress - Comfortable, controlled wrist arc within the expected reduced range; pain settling; surgeon's clearance for strengthening
Phase III — strengthening and return to function (from ~12 weeks)
With the fusion solid and motion restored to its useful ceiling, strengthening and graded loading begin and are built up over weeks. Return to manual work and sport is criterion-based.
For your hand therapist:
Assessments - Grip and pinch strength versus the other side; pain/swelling response to loading; task- and job-specific functional testing
Education and precautions - Begin progressive grip and wrist strengthening (putty, ball, then graded resistance) once cleared - Introduce loaded and weight-bearing tasks gradually; build up over several weeks rather than all at once - Expected end-point: grip recovering toward ~70–80% of the other side and a useful, pain-free, reduced arc
Management - Exercises: progressive gripping and forearm/wrist strengthening; graded functional and work simulation; ongoing scar management and ROM maintenance - Watch for and refer back to the surgeon if there is persistent dorsal wrist pain on extension (possible dorsal impingement), suspected nonunion, or a recovery plateau - Consider discharge once strength and function are adequate for the patient's daily and occupational needs
Criteria for return to load / work - Solid united fusion, pain-free within the restored arc, grip adequate for task; heavy manual demands deferred until ~4–6 months and graded up
Getting back to work and activity
Light everyday hand use (eating, writing, light self-care) is encouraged from the start, within comfort, as long as it does not load or twist the wrist. Because you must not drive while your wrist is in a cast or unable to safely control the wheel, plan for help with transport in the early weeks; driving resumes once you are out of the cast and can confidently control the car, as confirmed at your review.
Gripping, lifting and weight-bearing through the wrist wait until the fusion is confirmed solid (usually after about six to eight weeks) and are then built up gradually. People with desk-based or light work often return at around three months; heavier manual work is usually closer to four to six months and is reintroduced in stages. Throughout, remember that the planned result is a comfortable, useful wrist with a reduced range of movement, judged by how the wrist feels and functions, with Dr Hirpara and your hand therapist guiding the pace, not the calendar alone.
After your protocol
This protocol works alongside the practice's general recovery advice: see managing post-operative pain, wound care and scar management. The phased plan above reflects published rehabilitation guidance after partial wrist fusion, and your ongoing recovery is guided individually by Dr Hirpara and your hand therapist according to how your wrist heals and progresses.
Evidence & references
Topic scope: post-operative rehabilitation after midcarpal partial wrist arthrodesis for scapholunate advanced collapse (SLAC) or scaphoid nonunion advanced collapse (SNAC). The index procedure here is a capitolunate fusion (the capitate fused to the lunate, usually with excision of the worn scaphoid); the closely related four-corner fusion (lunate–capitate– triquetrum–hamate) follows the same rehabilitation principles. This is a bony arthrodesis, so the rehabilitation is a union-gated pathway: the mid-wrist is immobilised until the fusion consolidates, after which a deliberately reduced wrist arc and grip are restored.
Defining principle of the rehab here: a partial wrist fusion is a motion-preserving salvage. The arthritic midcarpal surfaces are fused to abolish pain, while the radiolunate joint is intentionally preserved to retain movement. The construct that needs protecting is healing bone (plate, headless screws, staples or K-wires across the fusion), not a soft-tissue repair — so progression is gated by radiographic union, not a calendar. Counselling the patient that the planned end-point is a pain-free, functional wrist with a reduced arc (~50–65% of normal flexion–extension, ~70–80% grip) is itself part of the treatment: the reduced motion is the intended trade-off, not a failure. The two principal branch points are the fixation method (which sets the immobilisation window and union risk) and whether scaphoid excision was performed (standard in the SLAC/SNAC setting).
A. PROCEDURE OUTCOMES (capitolunate / four-corner fusion for SLAC–SNAC)
Partial wrist fusion is a well-established, durable salvage for the SLAC/SNAC wrist. The dominant debate is which motion-preserving salvage (four-corner / capitolunate fusion vs proximal row carpectomy), not whether to operate; both reliably relieve pain at the cost of some motion.
- Reliable pain relief with a useful but reduced arc. Across series, midcarpal fusion abolishes the painful midcarpal arthritis while preserving radiolunate motion. Typical results are roughly 50–65% of contralateral flexion–extension and ~70–80% of contralateral grip strength, with high rates of pain relief and return to work — the expected, planned trade-off of a partial fusion [Enna Hand Clin 2005; Strauch J Hand Surg Am 2011; Merrell J Hand Surg Am 2008; long-term series J Wrist Surg 2015]. Moderate (cohort/consensus).
- Capitolunate fusion (± scaphoid excision) performs comparably to full four-corner fusion while fusing fewer joints, simplifying the construct. A systematic review of capitolunate arthrodesis and comparative work report comparable motion, grip and union to four-corner fusion, supporting it as a sound index choice [Dunn J Hand Surg Am 2020 (systematic review); lunocapitate series J Hand Surg Eur 2009; J Chin Med Assoc 2017]. Moderate.
- A meta-analysis of two-, three- and four-corner constructs finds the number of fused columns does not materially change motion, grip, union or complications — biomechanically consistent with the radiolunate joint being the motion-determining segment [Hundepool J Hand Surg Am 2025 (SR/meta-analysis); Hernandez-Soria J Hand Surg Am 2016 (capitate-position biomechanics)]. Moderate (SR) + mechanistic.
- Modern fixation is forgiving but union is not guaranteed. Circular dorsal plates, headless compression screws and nitinol staples all achieve consolidation in the great majority, with nonunion and dorsal impingement the characteristic failures to watch for [Merrell J Hand Surg Am 2008 (circular plate); Ahmady J Hand Surg Glob Online 2025 (nitinol staples)]. Moderate.
B. REHABILITATION / THERAPY EVIDENCE
The rehab questions are (1) how long to immobilise, (2) what gates the start of wrist motion, and (3) how to set the patient's expectation of reduced motion. The evidence and published surgeon protocols converge on a union-gated sequence: immobilise the wrist (mobilise the hand and forearm) for ~6–8 weeks, then restore a reduced arc, then strengthen.
- Immobilise until radiographic union, not by the calendar. Because the construct is bony, wrist motion is withheld until the surgeon confirms consolidation — typically 6–8 weeks, longer with some screw/staple fixations. Published institutional protocols use a bulky dressing/splint for ~10–14 days, a short-arm cast to ~4–6 weeks, then a removable splint as motion begins. Moderate (consensus protocols).
- Keep the hand and forearm fully mobile from day one. Immediate active finger, thumb and forearm rotation prevents stiffness and tendon adhesion without disturbing the fusion — the same glide-preserving logic used across hand rehab. Consensus.
- Restore motion gradually after union, against a realistic ceiling. Once united, active and active-assisted wrist ROM is introduced; patients should be counselled that the fused midcarpal segment will not move and the achievable arc is smaller than pre-operatively (the radiolunate joint alone supplies wrist motion). Consensus + mechanistic (capitate-position biomechanics, Hernandez-Soria 2016).
- Strengthen and load only once the fusion is solid. Grip and loaded/weight-bearing work begins after union and is built up gradually; heavy manual demands are deferred to ~4–6 months. Consensus.
Recovery trajectory (expected, evidence-anchored)
| Phase | Window | Restraint | Hand use / therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Immobilisation (union) | Week 0 to ~6–8 | Wrist immobilised (cast/splint) | Full active finger, thumb & forearm motion; oedema control, elevation; no wrist motion | None through the wrist | Fusion knits like a fracture; progress is gated by radiographic union, not the calendar |
| II — Restoring wrist motion | From union (~wk 6–8) to 12 | Heavy-load avoidance; removable splint | Begin active/active-assisted wrist flexion/extension & deviation; scar massage once healed | No loaded grip yet | Counsel the reduced-arc expectation (~50–65% of normal flexion–extension) |
| III — Strengthening & return | From ~12 weeks (post-union) | Restrictions lifted progressively | Progressive grip/wrist strengthening; graded job simulation | Grip recovers toward ~70–80% of the other side | Desk work ~3 months; heavy manual ~4–6 months. Watch for dorsal impingement / nonunion |
(Phase windows mirror the precautions in the patient protocol and published surgeon protocols; they are typical guides anchored to union, not trial-derived deadlines.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY
- Capitolunate vs four-corner vs proximal row carpectomy (PRC). All three are accepted motion-preserving salvages for SLAC/SNAC. PRC tends to give a slightly larger arc and avoids fusion-specific complications (nonunion, dorsal impingement, hardware), while fusion may give marginally better grip and is preferred where capitate-head or proximal-capitate cartilage is compromised. Systematic reviews and a meta-analysis find no consistent superiority of one over the other; choice is individualised [Mulford J Hand Surg Eur 2009; J Hand Surg Am 2024 meta-analysis; Strauch J Hand Surg Am 2011]. Moderate (SR/meta-analysis of mostly observational data).
- Capitolunate vs full four-corner construct. Fusing fewer columns (capitolunate) simplifies the construct without clearly compromising motion, grip or union versus four-corner — consistent with the radiolunate joint being the motion-determining segment [Dunn 2020 SR; Hundepool 2025 meta-analysis; Hernandez-Soria 2016]. Moderate.
- When can wrist motion safely start? Union timing varies with fixation, and protocols differ on exact cast duration. The defensible position is surgeon-confirmed radiographic union gates wrist ROM rather than a fixed week number. Weak–moderate (consensus; protocol variation).
- Reduced motion is the plan, not a complication. The preserved radiolunate joint supplies a smaller arc by design; mislabelling the expected ~50–65% range as a poor result drives unnecessary dissatisfaction. Strong mechanistically; cohort-supported.
- Characteristic failures: nonunion and dorsal impingement. Both are recognised, fixation-related complications; persistent dorsal wrist pain on extension or a non-progressing fusion warrants surgical review rather than more therapy [Merrell 2008; Ahmady 2025; long-term series 2015]. Moderate.
D. EVIDENCE STRENGTH FLAGS (summary)
- STRONG (mechanistic / well-supported): the reduced final arc is the planned consequence of preserving the radiolunate joint while fusing the midcarpal segment (capitate-position biomechanics); reliable pain relief from the fusion.
- MODERATE: typical outcome envelope (~50–65% flexion–extension, ~70–80% grip); equivalence of capitolunate and four-corner constructs; no consistent superiority of fusion vs PRC (SR/meta-analysis of largely observational data); modern fixation achieves high union with defined nonunion / dorsal impingement risk.
- WEAK / CONSENSUS: the specific union-gated immobilise → restore-motion → strengthen therapy sequence and exact phase timings (institutional/surgeon protocols, anchored to radiographic union rather than trial-derived).
CITATIONS
RAG corpus (180,000+ Orthopaedic articles)
- Enna M, Hoepfner P, Weiss AC. Scaphoid excision with four-corner fusion. Hand Clin. 2005. DOI: 10.1016/j.hcl.2005.08.012
- Dunn JC, Polmear MM, Scanaliato JP, et al. Capitolunate arthrodesis: a systematic review. J Hand Surg Am. 2020. DOI: 10.1016/j.jhsa.2019.10.007
- Hundepool CA, Duraku LS, Quanjel TJ, et al. Two-, three-, or four-corner arthrodesis for midcarpal osteoarthritis: a systematic review and meta-analysis. J Hand Surg Am. 2025. DOI: 10.1016/j.jhsa.2023.04.018
- Strauch RJ. Scapholunate advanced collapse and scaphoid nonunion advanced collapse arthritis — update on evaluation and treatment. J Hand Surg Am. 2011. DOI: 10.1016/j.jhsa.2011.01.018
- Merrell GA, McDermott EM, Weiss AC. Four-corner arthrodesis using a circular plate and distal radius bone grafting: a consecutive case series. J Hand Surg Am. 2008. DOI: 10.1016/j.jhsa.2008.02.001
- Hernandez-Soria A, Das De S, Model Z, et al. The effect of capitate position on coronal plane wrist motion after simulated 4-corner arthrodesis. J Hand Surg Am. 2016. DOI: 10.1016/j.jhsa.2016.07.101
- Ahmady AA, Zalzaleh M, Riedel BB. Midterm outcomes of four-corner fusion surgery using nitinol staples. J Hand Surg Glob Online. 2025. DOI: 10.1016/j.jhsg.2025.100805
- Mulford JS, Ceulemans LJ, Nam D, Axelrod TS. Proximal row carpectomy vs four corner fusion for scapholunate (SLAC) or scaphoid nonunion advanced collapse (SNAC) wrists: a systematic review of outcomes. J Hand Surg Eur Vol. 2009. DOI: 10.1177/1753193408100954
- Four-corner fusion versus proximal row carpectomy for scapholunate advanced collapse and scaphoid nonunion advanced collapse wrist: a systematic review and meta-analysis. J Hand Surg Am. 2024. DOI: 10.1016/j.jhsa.2024.01.011
- Long-term results of lunocapitate arthrodesis with scaphoid excision for SLAC and SNAC wrists. J Hand Surg Eur Vol. 2009. DOI: 10.1177/1753193409105683
- Lunocapitate fusion with scaphoid excision for the treatment of scaphoid nonunion advanced collapse or scapholunate advanced collapse wrist. J Chin Med Assoc. 2017. DOI: 10.1016/j.jcma.2016.10.001
- The long-term outcome of four-corner fusion. J Wrist Surg. 2015. DOI: 10.1055/s-0035-1549277
Partial wrist fusion rehabilitation literature (protocols & guidance — basis for the union-gated phase structure)
- University of Virginia Department of Orthopaedic Surgery. Wrist Partial Fusion (4-Corner) Rehabilitation Guidelines. https://med.virginia.edu/orthopaedic-surgery/wp-content/uploads/sites/242/2024/09/Wrist-Partial-Fusion-4-corner.pdf
- Oregon Health & Science University (OHSU). Four-Corner Partial Wrist Fusion — Surgery Guide. https://www.ohsu.edu/sites/default/files/2020-12/Four-Corner%20Partial%20Wrist%20Fusion.pdf
- Alaska Orthopedic Specialists. Four-Corner Fusion with Scaphoid Excision — Post-operative Protocol. https://www.akortho.com/wp-content/uploads/Four-Corner-Fusion-with-Scaphoid-Excision-1.pdf
- Twin Cities Orthopedics (Olson). Scaphoid Excision 4-Corner Fusion Post-operative Protocol. https://www.toportho.com/wp-content/uploads/2024/10/olson-_4-Corner-Fusion-Protocol.pdf
- The long-term outcome of four-corner fusion (open-access full text). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC4408128/





