Biến dạng Boutonnière
Patients › Hand
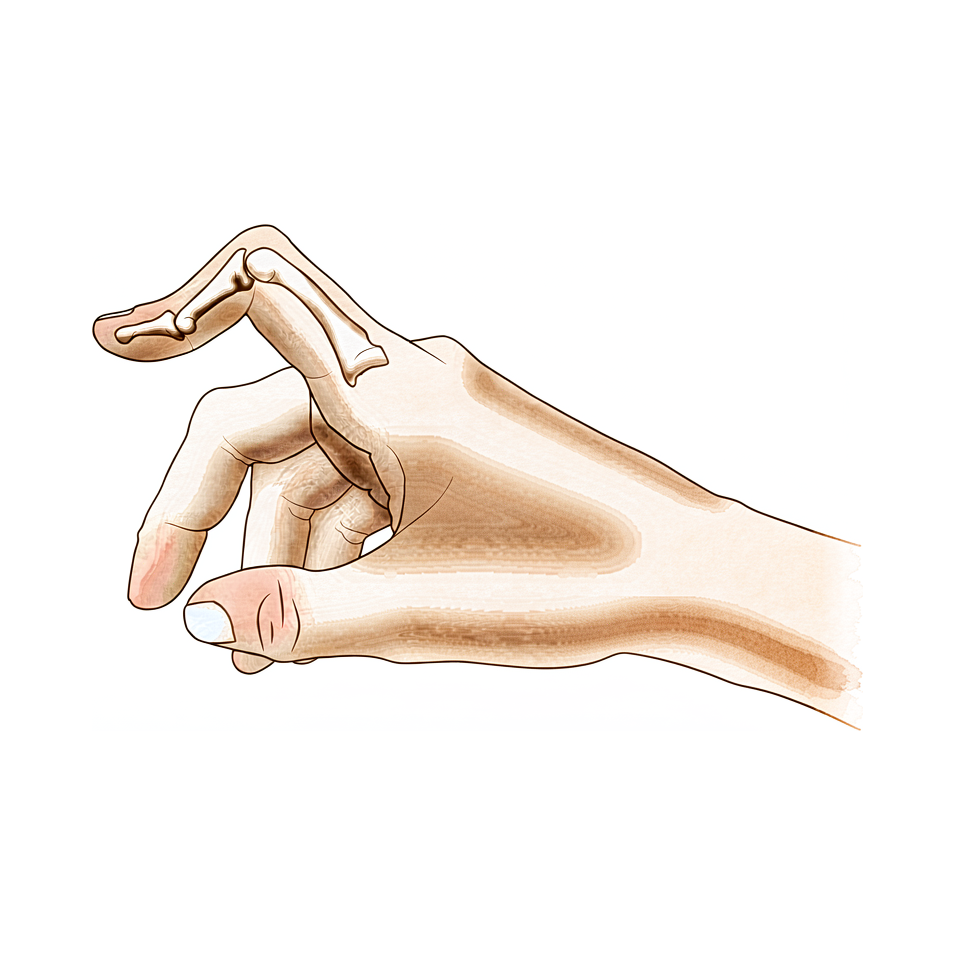
Extensor central-slip injury at the middle finger joint; early splinting prevents the zigzag deformity, established cases need surgery.
Những gì bạn đang cảm nhận
Bạn có thể nhận thấy khớp giữa của ngón tay cong vào trong trong khi khớp đầu ngón tay lại nhô ra. Hình dạng đặc biệt này được gọi là biến dạng boutonniere. Nó xảy ra khi các gân ở mặt trên của ngón tay bị lệch khỏi vị trí bình thường. Bạn có thể thấy sự thay đổi này phát triển chậm theo thời gian, hoặc xuất hiện đột ngột sau một chấn thương.
Cơn đau thường tập trung xung quanh khớp giữa của ngón tay. Sự khó chịu có thể cảm thấy như một cơn đau âm ỉ sâu hoặc một cơn đau nhói sắc khi bạn cử động ngón tay. Bạn có thể thấy rằng việc uốn cong ngón tay hoàn toàn gây ra nhiều đau hơn là giữ nó thẳng. Các hoạt động đòi hỏi phải nắm chặt hoặc bóp có thể trở nên khó khăn. Những nhiệm vụ đơn giản như cài cúc áo, xoay tay nắm cửa hoặc đánh máy có thể cảm thấy bất tiện hoặc gây đau.
Ngón tay của bạn có thể cảm thấy cứng, đặc biệt là vào buổi sáng. Bạn có thể nhận thấy sưng xung quanh khớp giữa. Sự cứng này có thể khiến bạn khó nắm tay thành nắm đấm. Nếu bạn bị viêm khớp dạng thấp, biến dạng có thể tiến triển khác với trường hợp do chấn thương. Không có viêm khớp hoặc chấn thương, khoảng 13% người dân trải qua tình trạng này.
Đầu ngón tay của bạn cũng có thể cảm thấy không ổn định. Trong một số trường hợp, khớp đầu ngón tay cong xuống nhiều hơn bình thường. Điều này có thể khiến bạn khó đặt ngón tay phẳng trên bàn. Bạn có thể gặp khó khăn khi đẩy mở cửa nặng hoặc nâng các vật nhẹ bằng tay đó. Ngủ nghiêng có thể đè lên ngón tay bị biến dạng, gây khó chịu.
Điều quan trọng là phải phân biệt biến dạng thực sự này với một chấn thương trông tương tự được gọi là pseudoboutonniere. Hai tình trạng này đòi hỏi cách chăm sóc khác nhau. Bác sĩ phẫu thuật của bạn sẽ xem xét kỹ cách ngón tay của bạn cử động để phân biệt chúng. Hiểu chính xác những gì bạn đang cảm nhận giúp định hướng kế hoạch điều trị tốt nhất cho bạn.
Những gì thực sự đang xảy ra
Khớp ngón tay của bạn là một bản lề phức tạp được tạo thành từ các xương, gân và một lớp vỏ bảo vệ gọi là bao khớp. Ở một ngón tay khỏe mạnh, một gân trung tâm chạy thẳng xuống giữa ngón tay để giúp duỗi ngón tay. Gân này hoạt động như sợi dây chính kéo ngón tay của bạn mở ra.
Trong biến dạng Boutonnière, gân trung tâm này bị tổn thương hoặc suy yếu. Nó có thể bị rách do chấn thương hoặc bị kéo giãn bởi các tình trạng như viêm khớp dạng thấp. Khi sự hỗ trợ trung tâm này thất bại, sự cân bằng lực trong ngón tay của bạn thay đổi. Các gân bên, vốn thường giúp uốn cong ngón tay, bắt đầu kéo quá mạnh.
Hãy tưởng tượng nó giống như một chiếc khóa kéo bị lệch khỏi đường ray. Các bộ phận vẫn còn đó, nhưng chúng không còn trượt mượt mà với nhau nữa. Vì gân trung tâm không còn giữ các bộ phận ở vị trí đúng, các gân bên bị trượt sang hai bên. Điều này khiến khớp giữa của ngón tay bị uốn cong vào trong, trong khi khớp đầu ngón tay có thể bị nhô ra.
Sự thay đổi về lực căng này là lý do khiến ngón tay của bạn trông cong queo và cảm thấy cứng. Bao khớp, vốn thường giữ cho khớp ổn định, trở nên căng và mất cân bằng. Theo thời gian, các mô thích nghi với vị trí sai lệch mới này. Đây là lý do tại sao biến dạng có thể tồn tại ngay cả khi bạn thử các phương pháp điều trị bảo tồn như nẹp hoặc vật lý trị liệu.
Yếu tố quan trọng nhất trong vấn đề này là sự thay đổi ở các gân và các cấu trúc liên quan. Những thay đổi này xảy ra sớm, đó là lý do tại sao chẩn đoán chính xác là rất quan trọng. Bác sĩ phẫu thuật của bạn cần phân biệt giữa biến dạng Boutonnière thực sự và một vấn đề tương tự được gọi là chấn thương giả Boutonnière. Lộ trình điều trị phụ thuộc hoàn toàn vào việc phân biệt chính xác điều này.
Nếu tổn thương được phát hiện sớm, bác sĩ phẫu thuật của bạn có thể tập trung vào việc khôi phục vị trí của gân trung tâm. Trong một số trường hợp, họ có thể sử dụng một mảnh nhỏ từ một gân khác để tái tạo khe trung tâm. Mảnh ghép mới này mô phỏng chức năng của gân ban đầu trong khi vẫn giữ nguyên các cử động khác của ngón tay. Mục tiêu là giữ cho khớp ở vị trí trung tâm và ổn định để bạn có thể di chuyển nó trở lại.
Tuy nhiên, nếu biến dạng đã tồn tại trong một thời gian dài, các mô có thể đã thay đổi vĩnh viễn. Trong những trường hợp mạn tính này, các sửa chữa đơn giản có thể không hiệu quả. Diễn biến tự nhiên của tình trạng này thường dẫn đến các vấn đề dai dẳng, đặc biệt nếu có viêm khớp dạng thấp liên quan. Kết quả lâu dài của việc tái tạo mô mềm trong những trường hợp này có thể không đáng tin cậy. Đôi khi, một thủ thuật cứu vãn triệt để hơn là cần thiết để sửa chữa hình dạng và chức năng của ngón tay bạn.
Những gì chúng tôi có thể làm về vấn đề này
Chúng tôi bắt đầu bằng việc điều trị không phẫu thuật để khôi phục khả năng vận động. Bạn sẽ thử nắn chỉnh theo chuỗi (serial casting) để đạt được sự duỗi đủ mức. Sau đó là việc sử dụng khớp chỉnh hình duỗi tương đối trong ba tháng. Bác sĩ phẫu thuật của bạn cũng có thể khuyên dùng vật lý trị liệu. Một đến hai mức độ cải thiện tầm vận động có thể đạt được với điều trị không phẫu thuật. Tuy nhiên, biến dạng có thể vẫn tồn tại ngay cả sau khi quản lý bảo tồn chuyên sâu. Chúng tôi sử dụng khớp chỉnh hình duỗi tương đối để tăng cường sự uốn cong chủ động của khớp liên đốt xa. Điều này giúp cải thiện sự duỗi của khớp ngón tay giữa. Bạn phải dành thời gian cho phương pháp này phát huy tác dụng trước khi xem xét phẫu thuật.
Quản lý y khoa tập trung vào sự thoải mái và giảm viêm. Nếu biến dạng của bạn liên quan đến viêm khớp dạng thấp, chúng tôi giải quyết hoạt động bệnh lý nền. Thuốc giảm đau và thuốc chống viêm giúp kiểm soát sự khó chịu. Tiêm có thể được khuyến nghị để giảm sưng trong khớp. Những điều trị này nhằm duy trì khả năng vận động của khớp và không đau trong khi bạn thực hiện liệu pháp. Mục tiêu là ổn định tình trạng và cải thiện chức năng hàng ngày của bạn mà không cần phẫu thuật.
Phẫu thuật được xem xét khi điều trị bảo tồn đã đạt đến giới hạn. Chúng tôi phân biệt biến dạng Boutonniere thực sự với chấn thương giả Boutonniere trước khi quyết định. Sự khác biệt này rất quan trọng trong việc xác định quản lý lâm sàng. Kết quả phẫu thuật thành công phụ thuộc vào việc khám tiền phẫu đầy đủ, phân giai đoạn chính xác biến dạng và thời điểm điều trị thích hợp. Nếu cần tái tạo mô mềm, chúng tôi hiểu rằng kết quả dài hạn có thể không đáng tin cậy. Biến dạng tái phát hoặc dai dẳng tốt nhất được điều trị bằng thủ thuật cứu vãn. Trong một số trường hợp, ghép gân hình chữ Y mang lại kết quả tốt hoặc xuất sắc. Bác sĩ phẫu thuật của bạn sẽ xác định nguyên nhân thực sự trước khi can thiệp phẫu thuật. Điều này đảm bảo thủ thuật được chọn phù hợp với giải phẫu và nhu cầu cụ thể của bạn.
Những điều cần mong đợi
Tiên lượng của bạn phụ thuộc rất nhiều vào việc đây là một dị dạng thực sự hay một tổn thương tương tự được gọi là pseudoboutonniere. Bác sĩ phẫu thuật của bạn phải xác nhận chẩn đoán trước tiên vì lộ trình điều trị thay đổi hoàn toàn dựa trên sự phân biệt này. Nếu bạn bị viêm khớp dạng thấp, kết quả dài hạn từ việc sửa chữa mô mềm thường không đáng tin cậy. Trong những trường hợp này, dị dạng dai dẳng hoặc tái phát có thể cần một thủ thuật cứu chữa sau đó.
Đối với hầu hết mọi người không bị viêm khớp dạng thấp, tình trạng này không phải lúc nào cũng tự khỏi. Điều trị không phẫu thuật có thể cải thiện tầm vận động của bạn từ một đến hai độ. Tuy nhiên, dị dạng rõ ràng có thể vẫn tồn tại ngay cả sau khi bạn hoàn thành việc quản lý bảo tồn chuyên biệt. Nếu chăm sóc bảo tồn không đủ, phẫu thuật cung cấp một lựa chọn mạnh mẽ. Ghép gân hình chữ Y mang lại kết quả tốt hoặc xuất sắc ở 16 trong số 18 bệnh nhân trong các loạt báo cáo. Thành công cũng phụ thuộc vào việc bác sĩ phẫu thuật của bạn thực hiện một cuộc khám toàn diện, phân loại dị dạng chính xác và chọn thời điểm can thiệp phù hợp.
Quá trình hồi phục là một quá trình dần dần. Nếu bạn bắt đầu với điều trị không phẫu thuật, bạn có thể sử dụng nẹp cố định tuần tự để thẳng ngón tay, tiếp theo là ba tháng sử dụng nẹp vận động tương đối ở tư thế gập. Phương pháp này mang lại kết quả tương tự như các phương pháp khác cho các trường hợp mạn tính và thường được thử nghiệm trước khi xem xét phẫu thuật. Bạn nên mong đợi việc đeo nẹp trong vài tháng để duy trì tư thế duỗi và cải thiện tư thế gập.
Nếu cần phẫu thuật, mục tiêu là khôi phục chức năng và sự thẳng hàng. Bạn sẽ cần tuân thủ chặt chẽ các hướng dẫn cụ thể của bác sĩ phẫu thuật. Diễn biến tự nhiên của dị dạng này có thể khác nhau, nhưng việc quản lý sớm và chính xác dẫn đến kết quả tốt nhất. Hãy kiên nhẫn với quá trình chữa lành. Cần có thời gian để các gân và khớp thích nghi với các vị trí mới của chúng. Bác sĩ phẫu thuật của bạn sẽ hướng dẫn bạn qua từng giai đoạn để đảm bảo khả năng quay trở lại các hoạt động hàng ngày của bạn là tốt nhất có thể.
Khi nào cần gặp bác sĩ
Hãy gặp bác sĩ đa khoa nếu bạn nhận thấy một sự cong ở khớp giữa của ngón tay không thể duỗi thẳng. Hãy yêu cầu đánh giá bởi bác sĩ chuyên khoa nếu bạn có cơn đau dai dẳng không cải thiện khi nghỉ ngơi. Hãy tìm kiếm sự chăm sóc y tế nếu bạn cảm thấy yếu hoặc mất ổn định ở ngón tay. Hãy đến gặp bác sĩ nếu ngón tay bị khóa hoặc đột ngột mất lực khi sử dụng. Hãy liên hệ với bác sĩ phẫu thuật của bạn nếu các triệu chứng ảnh hưởng đến giấc ngủ hoặc công việc của bạn. Sự xấu đi đột ngột của biến dạng cũng cần được chú ý ngay lập tức. Chẩn đoán chính xác là rất quan trọng để điều trị đúng cách. Việc phân biệt giữa một biến dạng thực sự và một chấn thương tương tự giúp xác định phương pháp chăm sóc phù hợp. Đánh giá sớm đảm bảo kết quả tốt nhất cho chức năng bàn tay của bạn.
Evidence & references
Overview
- Differentiating a true boutonniere deformity from a pseudoboutonniere injury is critical in determining clinical management [2].
- An understanding of the anatomy, clinical presentation, treatment options, and expected outcomes is crucial for optimal treatment of posttraumatic boutonniere and swan neck deformities [4].
- The natural history of the boutonnière deformity in rheumatoid arthritis is outlined, and a simple method of repair is described [3].
- The prevalence of boutonnière deformity without rheumatoid arthritis or trauma is approximately 13% [5].
- One to two grades of ROM improvement can be achieved with nonoperative treatment, although deformity can persist even after dedicated conservative management [8].
- Similar results occurred for chronic boutonniere deformity using serial casting for adequate extension followed by 3 months of RMF orthotic use, which should be attempted prior to surgical intervention [1].
- Long-term results following soft tissue reconstruction for boutonniere deformity in rheumatoid arthritis are unreliable, and recurrent or persistent deformity is best treated with a salvage procedure [9].
- A successful operative result for swan-neck and boutonniere deformities in the rheumatoid hand depends on complete preoperative examination, correct staging of the deformity, and proper timing of treatment [10].
- The Y-shaped tendon graft can be a useful procedure for the correction of chronic boutonniere deformity, providing good or excellent results in 16 of 18 patients in one series [6].
- Detachment of up to two-thirds of the phalangeal length was effective in reducing extensor lag of the DIP joint and did not cause any boutonniere deformity in a cadaveric model of fractional Fowler tenotomy for chronic mallet finger [7].
Anatomy & Pathophysiology
- Boutonnière deformity can persist even after dedicated conservative management [8].
- One to two grades of range of motion improvement can be achieved with nonoperative treatment of Boutonnière deformity [8].
- Accurate diagnosis and treatment of finger metacarpophalangeal joint injuries begins with an understanding of all potential diagnoses [15].
- Hand surgery and hand therapy practice interventions, including use of relative motion flexion orthoses for management of non-surgical and surgical extensor mechanism injuries, may benefit from an in-depth look at extensor mechanism zone III and IV anatomy and biomechanics [19].
- The most important factor in the development of finger deformities is the changes occurring in the tendons and related structures, especially in early stages [21].
- Reconstruction of the extensor central slip using a distally based flexor digitorum superficialis slip provides a robust repair that anatomically mimics the extensor central slip while maintaining the function of the donor FDS tendon [24].
- The main goals of any treatment of a proximal interphalangeal joint complication are maintaining concentric reduction of the joint, restoring joint stability, and facilitating early range-of-motion exercises [33].
Classification
- Differentiating a true boutonniere deformity from a pseudoboutonniere injury is critical in determining clinical management [2].
- The natural history of the boutonnière deformity in rheumatoid arthritis is outlined [3].
- The prevalence of boutonnière deformity without rheumatoid arthritis or trauma is approximately 13% [5].
- A modified Terrono classification for Type 1 thumb deformity in rheumatoid arthritis could detect advanced deformity earlier and was more strongly correlated with hand function [17].
Clinical Presentation
- Differentiating a true boutonniere deformity from a pseudoboutonniere injury is critical in determining clinical management [2].
- An understanding of the clinical presentation is crucial for optimal treatment of posttraumatic boutonnière and swan neck deformities [4].
- Accurate diagnosis of finger metacarpophalangeal joint injuries begins with an understanding of all potential diagnoses [15].
- The natural history of the boutonnière deformity in rheumatoid arthritis is outlined in historical literature [3].
- The prevalence of boutonnière deformity without rheumatoid arthritis or trauma is approximately 13% [5].
- The swan neck deformity can progress significantly with time due to increasing distal interphalangeal joint flexion contracture [14].
Investigations
- Differentiating a true boutonniere deformity from a pseudoboutonniere injury is critical in determining clinical management [2].
- An understanding of the anatomy, clinical presentation, treatment options, and expected outcomes is crucial for optimal treatment of posttraumatic boutonnière and swan neck deformities [4].
- Accurate diagnosis and treatment of finger metacarpophalangeal joint injuries begins with an understanding of all potential diagnoses [15].
- It is necessary to determine the true etiology before surgical intervention [12].
- A successful operative result depends on complete preoperative examination, correct staging of the deformity, and proper timing of treatment [10].
- Cortical breaks were commonly visualized in MCP and PIP joints with HR-pQCT and microCT [37].
Treatment
- Serial casting for adequate extension followed by 3 months of relative motion flexion (RMF) orthotic use should be attempted prior to surgical intervention for chronic boutonniere deformity [1].
- Differentiating a true boutonniere deformity from a pseudoboutonniere injury is critical in determining clinical management [2].
- A simple method of repair is described for the boutonnière deformity in rheumatoid arthritis [3].
- Understanding the anatomy, clinical presentation, treatment options, and expected outcomes is crucial for optimal treatment of posttraumatic boutonnière and swan neck deformities [4].
- The prevalence of boutonnière deformity without rheumatoid arthritis or trauma is approximately 13% [5].
- The Y-shaped tendon graft is a useful procedure for the correction of chronic boutonniere deformity, providing good or excellent results in 16 of 18 patients in a reported series [6].
- Detachment of up to two-thirds of the phalangeal length is effective in reducing extensor lag of the DIP joint and does not cause any boutonniere deformity in a cadaveric model [7].
- One to two grades of ROM improvement can be achieved with nonoperative treatment, although deformity can persist even after dedicated conservative management [8].
- Long-term results following soft tissue reconstruction for boutonniere deformity in rheumatoid arthritis are unreliable, and recurrent or persistent deformity is best treated with a salvage procedure [9].
- A successful operative result for swan-neck and boutonniere deformities in the rheumatoid hand depends on complete preoperative examination, correct staging of the deformity, and proper timing of treatment [10].
- Metacarpophalangeal joint arthroplasty improves function and deformity and achieves nearly uniform patient satisfaction in rheumatoid arthritis [11].
- One technique does not treat all finger deformities uniformly, highlighting the need to determine the true etiology before surgical intervention [12].
- The use of relative motion flexion orthoses (RMFO) is effective in increasing active distal interphalangeal joint flexion and improving PIP extension in patients with Burton stage 1 chronic boutonniere deformity [13].
Complications
- Differentiating a true boutonniere deformity from a pseudoboutonniere injury is critical in determining clinical management [2].
- The prevalence of boutonniere deformity without rheumatoid arthritis or trauma is approximately 13% [5].
- Detachment of up to two-thirds of the phalangeal length was effective in reducing extensor lag of the DIP joint and did not cause any boutonniere deformity in a cadaveric model [7].
- Long-term results following soft tissue reconstruction for boutonniere finger deformity in rheumatoid arthritis are unreliable [9].
- Recurrent or persistent deformity is best treated with a salvage procedure [9].
- A successful operative result depends on complete preoperative examination, correct staging of the deformity, and proper timing of treatment [10].
- One technique does not treat all deformities uniformly, highlighting the need to determine the true etiology before surgical intervention [12].
- Swan neck deformity can progress significantly with time due to increasing DIPJ flexion contracture [14].
Recovery
- Serial casting for adequate extension followed by 3 months of relative motion flexion (RMF) orthotic use yields similar results for chronic boutonniere deformity and should be attempted prior to surgical intervention [1].
- One to two grades of range of motion (ROM) improvement can be achieved with nonoperative treatment, although deformity can persist even after dedicated conservative management [8].
- The Y-shaped tendon graft is a useful procedure for the correction of chronic boutonniere deformity, providing good or excellent results in 16 of 18 patients in a reported series [6].
- The use of relative motion flexion orthoses (RMFO) is effective in increasing active distal interphalangeal joint flexion and improving proximal interphalangeal (PIP) extension in patients with Burton stage 1 chronic boutonniere deformity [13].
- Long-term results following soft tissue reconstruction for boutonniere deformity in rheumatoid arthritis are unreliable, and recurrent or persistent deformity is best treated with a salvage procedure [9].
- A successful operative result for boutonniere deformity depends on complete preoperative examination, correct staging of the deformity, and proper timing of treatment [10].
Key Evidence
- [L4] Similar results occurred for chronic boutonniere deformity using serial casting for adequate extension followed by 3 months of RMF orthotic use, which should be attempted prior to surgical intervention. [1] (10.1016/j.jht.2023.02.005)
- [L5] Differentiating a true boutonniere deformity from a pseudoboutonniere injury is critical in determining clinical management. [2] (10.1016/j.jhsa.2022.10.019)
- [L4] The natural history of the boutonnière deformity in rheumatoid arthritis is outlined, and a simple method of repair is described. [3] (10.2106/00004623-196951070-00009)
- [L5] An understanding of the anatomy, clinical presentation, treatment options, and expected outcomes is crucial for optimal treatment of posttraumatic boutonnière and swan neck deformities. [4] (10.5435/jaaos-d-14-00272)
- [L3] The prevalence of boutonnière deformity without rheumatoid arthritis or trauma is approximately 13%. [5] (10.1177/1753193417704610)
- [L4] The Y-shaped tendon graft can be a useful procedure for the correction of chronic boutonniere deformity; in our patient series, this provided good or excellent results in 16 of 18 patients. [6] (10.1016/j.jhsa.2021.01.003)
- [L5] Detachment of up to two-thirds of the phalangeal length was effective in reducing extensor lag of the DIP joint and did not cause any boutonniere deformity in this cadaveric model. [7] (10.1016/j.jhsa.2012.07.039)
- [L3] One to two grades of ROM improvement can be achieved, although deformity can persist even after dedicated conservative management. [8] (10.1016/j.jht.2025.02.013)
- [L5] Long-term results following soft tissue reconstruction are unreliable, and recurrent or persistent deformity is best treated with a salvage procedure. [9] (10.1016/j.jhsa.2011.05.029)
- [L5] A successful operative result depends on complete preoperative examination, correct staging of the deformity, and proper timing of treatment. [10] (10.5435/00124635-199903000-00002)
- [L5] Follow-up studies show that this surgery improves function and deformity and achieves nearly uniform patient satisfaction. [11] (10.5435/00124635-200305000-00005)
- [L5] It emphasizes that one technique does not treat all deformities uniformly and highlights the need to determine the true etiology before surgical intervention. [12] (10.1016/j.jhsa.2022.07.008)
- [L4] The use of RMFO is effective in increasing active distal interphalangeal joint flexion and improving PIP extension in patients with Burton stage 1 chronic boutonniere deformity. [13] (10.1016/j.jhsa.2022.08.007)
- [L5] The swan neck deformity in this individual progressed significantly with time because of increasing DIPJ flexion contracture. [14] (10.1016/j.jht.2009.11.005)
- [L5] Accurate diagnosis and treatment of finger metacarpophalangeal joint injuries in athletes begins with an understanding of all potential diagnoses, allowing for safe and early return to play. [15] (10.5435/jaaos-d-21-01031)
- [L3] The modified classification could detect advanced deformity earlier and was more strongly correlated with hand function. [17] (10.1177/1753193419886719)
- [L5] Hand surgery and hand therapy practice interventions, including use of RMF orthoses for management of non-surgical and surgical EM injuries may benefit from an in-depth look at the EM zone III and IV anatomy and biomechanics. [19] (10.1016/j.jht.2023.01.002)
- [L4] The most important factor in the development of finger deformities is the changes occurring in the tendons and related structures, especially in early stages. [21] (10.2106/00004623-195739030-00006)
- [L4] The modified technique provides a robust repair that anatomically mimics the extensor central slip yet maintains the function of the donor FDS tendon. [24] (10.1016/j.jhsa.2009.01.025)
- [L5] The main goals of any treatment of a PIP joint complication are maintaining concentric reduction of the joint, restoring joint stability, and facilitating early range-of-motion exercises. [33] (10.1016/j.hcl.2017.12.014)
- [L4] Cortical breaks were commonly visualized in MCP and PIP joints with HR-pQCT and microCT. [37] (10.1186/s12891-016-1148-y)
References
[1] The relative motion concept in acute and chronic boutonniere deformity: Invited commentary. Journal of Hand Therapy. 2023. DOI: 10.1016/j.jht.2023.02.005 [2] Boutonniere Versus Pseudoboutonniere Deformities: Pathoanatomy, Diagnosis, and Treatment. The Journal of Hand Surgery. 2023. DOI: 10.1016/j.jhsa.2022.10.019 [3] Correction of the Rheumatoid Boutonnière Deformity. The Journal of Bone & Joint Surgery. 1969. DOI: 10.2106/00004623-196951070-00009 [4] Posttraumatic Boutonnière and Swan Neck Deformities. Journal of the American Academy of Orthopaedic Surgeons. 2015. DOI: 10.5435/jaaos-d-14-00272 [5] Thumb boutonnière deformity without rheumatoid arthritis or trauma. Journal of Hand Surgery (European Volume). 2017. DOI: 10.1177/1753193417704610 [6] Y-Shaped Tendon Graft—A Technique in the Reconstruction of Posttraumatic Chronic Boutonniere Deformity. The Journal of Hand Surgery. 2021. DOI: 10.1016/j.jhsa.2021.01.003 [7] Fractional Fowler Tenotomy for Chronic Mallet Finger: A Cadaveric Biomechanical Study. The Journal of Hand Surgery. 2012. DOI: 10.1016/j.jhsa.2012.07.039 [8] Nonoperative treatment of the Boutonniere deformity: Is there a difference in outcomes?. Journal of Hand Therapy. 2025. DOI: 10.1016/j.jht.2025.02.013 [9] Treatment of Boutonniere Finger Deformity in Rheumatoid Arthritis. The Journal of Hand Surgery. 2011. DOI: 10.1016/j.jhsa.2011.05.029 [10] Operative Correction of Swan-Neck and Boutonniere Deformities in the Rheumatoid Hand. Journal of the American Academy of Orthopaedic Surgeons. 1999. DOI: 10.5435/00124635-199903000-00002 [11] Metacarpophalangeal Joint Arthroplasty in Rheumatoid Arthritis. Journal of the American Academy of Orthopaedic Surgeons. 2003. DOI: 10.5435/00124635-200305000-00005 [12] Clarification of Extensor Tenotomy for Finger Deformities. The Journal of Hand Surgery. 2022. DOI: 10.1016/j.jhsa.2022.07.008 [13] The Use of Relative Motion Flexion Orthoses for Chronic Boutonniere Deformity. The Journal of Hand Surgery. 2024. DOI: 10.1016/j.jhsa.2022.08.007 [14] Swan Neck Deformity after Distal Interphalangeal Joint Flexion Contractures: A Biomechanical Analysis. Journal of Hand Therapy. 2010. DOI: 10.1016/j.jht.2009.11.005 [15] Finger Metacarpophalangeal Joint Injuries in Athletes: Evaluation, Diagnosis, Treatment, and Return to Play. Journal of the American Academy of Orthopaedic Surgeons. 2023. DOI: 10.5435/jaaos-d-21-01031 [17] A modified Terrono classification for Type 1 thumb deformity in rheumatoid arthritis: a cross-sectional analysis. Journal of Hand Surgery (European Volume). 2019. DOI: 10.1177/1753193419886719 [19] An in-depth look at zone III and IV anatomy of the finger extensor mechanism and some clinical implications for use of the relative motion flexion orthosis. Journal of Hand Therapy. 2023. DOI: 10.1016/j.jht.2023.01.002 [21] Finger Deformities Caused by Rheumatoid Arthritis. The Journal of Bone & Joint Surgery. 1957. DOI: 10.2106/00004623-195739030-00006 [24] Reconstruction of the Extensor Central Slip Using a Distally Based Flexor Digitorum Superficialis Slip. The Journal of Hand Surgery. 2009. DOI: 10.1016/j.jhsa.2009.01.025 [33] Complications of Proximal Interphalangeal Joint Injuries. Hand Clinics. 2018. DOI: 10.1016/j.hcl.2017.12.014 [37] Visual detection of cortical breaks in hand joints: reliability and validity of high-resolution peripheral quantitative CT compared to microCT. BMC Musculoskeletal Disorders. 2016. DOI: 10.1186/s12891-016-1148-y





