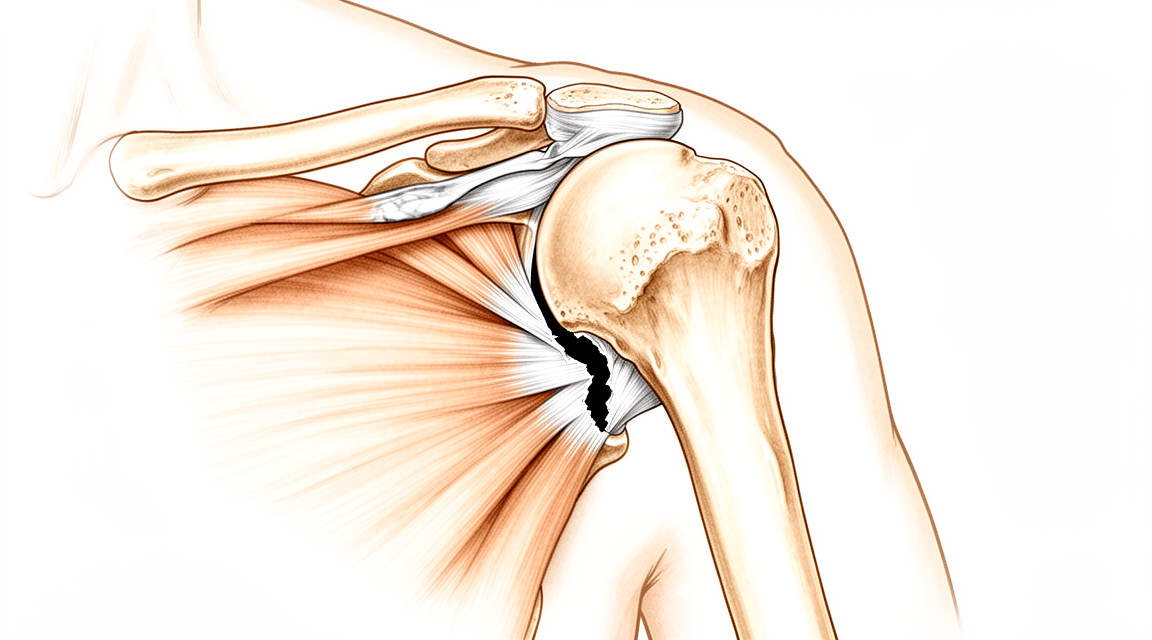
肩袖修复
Patients › Rehabilitation
Staged rehabilitation protocol after rotator cuff repair at Mater Private Hospital Rockhampton, with the early exercise program.
本方案旨在指导您在基兰·希尔帕拉(Kieran Hirpara)医生处接受肩袖修复术后的康复过程。方案将每个阶段的通俗解释与结构化康复计划相结合,您可以将此计划分享给您的物理治疗师;请在首次就诊时携带此页面或其PDF版本,以确保康复过程协调一致。您的物理治疗师可能会根据您的康复进展调整该计划。
如果您对术后伤口有任何疑虑,请联系诊室。拍摄伤口照片并通过电子邮件发送以供审查通常很有帮助。
预期情况
肩袖修复术将撕裂的肌腱重新附着于骨头上,而整个康复计划旨在保护这种生物学上的再附着。术后六周时修复处仍然较软,并在随后的数月内持续成熟:在愈合研究中,术后六周时其强度仅约为正常强度的四分之一,十二周时约为二分之一,且至少需要六个月才能达到接近完全的强度。这就是为什么活动和负荷是逐步恢复,而不是一次性全部恢复的原因。
早期急于活动是人之常情,但证据令人安心。对于常见的较小和中等大小撕裂,早期活动所获得的额外活动度是暂时的,到术后一年时,早期开始活动与稍晚开始活动之间没有差异。在最初几周保持耐心,长远来看不会有任何损失,并且能在修复处最脆弱的时候提供保护。也有充分证据表明,在术后第一周就开始激进治疗弊大于利,因此最初几周刻意保持温和。
您能为肩膀做的最有用的事情就是早期保护修复处。大多数再撕裂发生在术后三到六个月内,未遵守早期限制的患者再撕裂的可能性要大得多。遵守方案比任何锻炼都重要。
肩袖修复术通常与同一手术中的其他操作联合进行:最常见的是肩峰下减压术、远端锁骨切除术、肱二头肌腱固定术或肩胛上神经松解术。当出现这种情况时,本方案适用于整个恢复过程:修复的肌腱是愈合最慢的部分,其时间表决定了整体进度。
您的恢复时间表取决于所修复撕裂的大小。这是决定进度的最关键因素,因为较大的撕裂愈合更慢,且再撕裂的可能性更高。Hirpara 医生会告知您的修复属于哪一组,下文将计划分为两个明确标记的轨道:
- 小/中等撕裂: 一根或两根肌腱,组织质量良好。
- 大/巨大撕裂: 较大的撕裂,涉及两根或更多肌腱,或组织质量较差。步骤相同,但持续时间更长且进展更为谨慎:保护性活动维持时间更长,主动活动恢复较晚,力量训练推迟。
手术过程
您的肩袖修复手术通常采用关节镜(微创)方式进行,偶尔也会通过一个小切口进行开放手术。撕裂的肌腱会被重新固定到肱骨顶端的骨性附着点上,康复工作的重点是在肌腱愈合期间保护该修复部位,随后逐步恢复关节的完全活动度、力量和功能。
佩戴您的悬吊带
您将佩戴简易肩关节悬吊带,而非外展枕式悬吊带。两者在预后结果上并无证实的差异,且简易悬吊带更易于日常使用。Hirpara 医生在每一例肩袖修复术中均使用简易悬吊带,包括大型和巨大撕裂。
- 白天佩戴悬吊带 6 周以提供支撑,特别是在外出或身处他人面前时。
- 您睡觉时不佩戴悬吊带。 它仅用于日间支撑;睡眠时请取下,将手臂舒适地支撑在枕头上。
- 淋浴和进行锻炼时取下悬吊带(在您被指导如何操作后)。只要取下悬吊带,请保持手臂放松并置于身体侧面。
- 如果肩部肿胀或疼痛,请使用冰敷,尤其是在锻炼后。
佩戴悬吊带时请注意您的姿势:保持耳朵、肩膀和髋部在一条直线上,避免含胸驼背。良好的姿势可保护您的背部,并有助于防止肩部僵硬。
重要注意事项——禁止事项
- 在术后约 6 周内,严禁依靠自身力量主动活动肩关节(术后 4 周时,修复组织的强度仅约为正常强度的 20%)。
- 术后 6 周内,严禁通过手或手臂进行提、推、拉动作或承重。
- 早期严禁将手臂向外旋转超过中立位(即正前方位置)。
- 如果修复了肩袖前侧肌腱(肩胛下肌): 在前 12 周内,主动外旋角度应控制在约 30° 以内,且在此期间禁止主动向内旋转手臂(抗阻内旋);此举旨在保护前侧修复部位。您的主刀医生会告知您是否适用此规定。
- 严禁做“空罐试验”动作(拇指向下)的抬臂练习。永远不要做。
- 早期严禁将手伸至背后,并避免任何突然的猛拉或推挤动作。
- 如可能,在前约 12 周内避免服用非甾体抗炎药(NSAIDs);此类药物可能会干扰肌腱愈合。请咨询诊所关于止痛药的使用建议。
- 在需要佩戴悬吊带期间(6 周),严禁驾驶车辆。
小/中型撕裂
这是针对一个或两个肌腱撕裂且组织状况良好的情况。如果某个阶段标注了周数,这表示您的时间安排。
中小型撕裂伤 — 第一阶段:保护期(第0–6周)
前六周的核心目标只有一个:在肌腱开始愈合于骨头的过程中保护修复部位。白天佩戴简易吊带提供支撑,睡觉时取下吊带,通过冰敷控制肿胀,并进行轻柔的练习,以保持手、腕、肘和颈部的活动度,同时避免对修复的肌腱施加负荷。您的物理治疗师(或在健侧手臂的帮助下由您自己)为您轻柔地活动肩部;您需保持完全放松。
- 吊带: 白天佩戴简易吊带提供支撑;睡觉时取下吊带;进行锻炼和卫生清洁时取下。
- 允许的活动: 仅限辅助性和被动活动;不得依靠自身肩部力量进行任何活动。由健侧手臂或拐杖完成动作。早期逐渐增加仰卧位辅助前屈至约 90°(半程),辅助外旋仅限至正位(中立位)。
- 练习: 钟摆运动;仰卧位辅助前举;手臂外展托抱式;辅助外旋至中立位;轻柔的手、腕和肘部活动;肩胛骨和颈部练习。
进入下一阶段的指征: 疼痛通过简单止痛药得到缓解和控制(约3/10或更低);辅助前屈舒适地达到约 90°;辅助外旋舒适地达到中立位;伤口已愈合且无异常迹象;且无修复部位过度受力的迹象。
中小型撕裂伤——第二阶段:恢复活动度(第6–12周)
修复处正在愈合,但仍较薄弱,在第6周时仅具有正常强度的约20–30%。因此,本阶段旨在恢复活动度,而非力量。此时已不再使用吊带。您将从辅助活动逐步过渡到自主活动,从省力体位开始(如仰卧位,或在桌面上滑动以消除重力影响),并逐渐过渡到直立位。本阶段后期加入轻度肌肉激活(等长)训练。
- 吊带: 已停用(在第4–6周时已基本停用)。
- 允许的活动: 全范围辅助活动,约从第6周开始过渡到自主活动。辅助/主动前屈活动度逐渐增加至约120°及以上。
- 锻炼: 仰卧位辅助前举;辅助外旋(使用棍棒);坐位桌面滑动;门框滑轮训练;轻柔的等长(按压并保持)外旋、内旋和外展训练(约从第8周开始);本阶段后期(第9周后)进行交叉臂拉伸。
进入下一阶段的标准: 您能够自主将手臂前屈至至少115–120°且控制良好(无耸肩或肩胛骨代偿性上提);辅助/被动活动度完全或接近完全且无痛;轻柔的等长训练后无疼痛加重;且在开始抗阻训练前,疼痛评分不超过约2/10。
中小型撕裂——第三阶段:强化训练(第12–16周)
这是修复组织成熟最快的时期,重点从恢复活动度转向重建力量、耐力和控制力。从大约第12周开始,使用轻阻力带和轻重量进行抗阻训练:高重复次数,低负荷。黄金法则是一次一个平面:只有在该方向上获得接近全范围且舒适的活动度后,才能在该方向上进行强化训练。始终拇指向上发力,严禁拇指向下。
- 吊带: 无需使用;预期可实现全范围活动。
- 练习: 肩高位置的外旋弹力带练习;使用棍棒的内部旋转练习;全范围上举(full-can lift);低拉(肩胛骨后缩);弹力带划船;睡眠者拉伸。您的物理治疗师可能还会加入节律性稳定训练(轻柔的保持稳定练习,治疗师轻轻推动您的手臂,您进行抵抗)以重新训练控制力;此为手法操作,无图示。
进入下一阶段的准备标准: 您能够自主完成全范围且无痛的活动,并具备肩胛骨控制能力;强化训练后无疼痛或肿胀;在肩胛骨平面内能够舒适地进行抗阻抬举;旋转力量正在向对侧水平发展(轻柔测试下约为80%;完全力量测试需推迟至更晚阶段)。
中小型撕裂——第四阶段:重返运动与工作(第16–24周)
本阶段是恢复肩部完全功能的过渡期,随后逐步重返运动及重体力工作。您需保持已获得的关节活动度,并增强力量、爆发力和耐力,以自信地进行过头伸手、搬运及工作等动作。重返活动是分阶段进行的,而非突然恢复;对于运动,采用逐步增加训练量和强度的间歇性训练计划是重返赛场最安全的方式。
- 支具: 无需佩戴。
- 练习: 使用轻重量并逐渐增加重量的全范围外旋抬举(full-can lift);针对运动和工作的特异性体能训练、渐进式负荷训练,以及在阶段后期酌情进行的受控高速(增强式)训练。
重返活动的标准: 您的旋转肌群力量至少达到对侧的 85–90%;在较大负荷下拥有完全且无痛的活动范围,且无反应性肿胀;并通过针对您运动项目或职业的任务特异性测试。重返运动或重体力工作通常在4–6个月左右,这取决于是否满足上述标准,以及是否获得Hirpara医生和您的物理治疗师的许可,而非仅依据日历时间。
大型/巨大撕裂
这是针对较大撕裂(涉及两条或更多肌腱,或组织质量较差)的康复路径。各阶段相同,但每个阶段需延长维持时间,并更谨慎地推进,以促进愈合。部分外科医生会刻意延迟该组患者的正式康复治疗;请遵循 Hirpara 医生给予您的具体指导。仍使用简单吊带,不使用外展枕,即使是大型或巨大撕裂。
巨大撕裂 — 第一阶段:保护期(第0–6周)
与小/中型撕裂路径相同,但活动受到严格保护,且进展更为缓慢。由您的物理治疗师或健侧手臂为您移动肩关节;您需保持放松。在此组别中,有时会延迟正式康复治疗以促进愈合。
- 吊带: 日间使用简单吊带提供支撑;睡眠时不佩戴吊带;进行锻炼和卫生清洁时取下。
- 允许的活动: 仅限受保护的被动活动,以Hirpara医生设定的范围为限;通常活动度小于小/中型撕裂路径。
- 锻炼: 钟摆运动;按指示进行轻柔的受保护辅助活动;手、腕和肘部活动;肩胛骨定位练习。
进入下一阶段的条件: 疼痛得到控制;修复部位无过度受压的迹象;且Hirpara医生允许您进展(此组别个体化差异大;切勿仅凭日历自行推进)。
巨大撕裂 — 第二阶段:恢复活动度(第6–12周)
支具通常在第6周去除,但主动活动度的引入比小/中型撕裂方案更晚且更个体化,以提供更长的修复保护。抗阻袖肌训练被刻意推迟。
- 支具: 约在第6周开始停用。
- 允许的活动: 辅助活动逐渐过渡至主动活动,时间晚于小/中型方案;具体时机由物理治疗师根据愈合情况确定。
- 练习: 与小/中型方案第二阶段相同的训练(辅助前举、辅助棍棒外旋、桌面滑动、门框滑轮),但进展更缓慢;抗阻袖肌训练被推迟。
进入下一阶段的条件: 主动活动度稳步改善;辅助/被动活动度完全恢复;肩胛骨控制良好;且医疗团队认为修复愈合良好,足以开始负荷训练。
巨大型撕裂——第三阶段:强化训练(约从第16周开始)
强化训练延迟至约第16周进行,而非第12周,因为较大的修补需要更长的时间才能成熟。此后,进展过程与小/中型撕裂的强化阶段相同:使用轻阻力带和哑铃,高重复次数,低负荷,每次针对一个平面,始终保持拇指朝上。
- 吊带: 无需使用;预期可完全活动。
- 锻炼: 同小/中型撕裂强化阶段的锻炼(弹力带外旋、使用棍棒的内旋、全范围上举、低拉、弹力带划船、睡眠者拉伸),开始时间较晚并逐步增加强度。随着控制能力的提高,可加入节律性稳定训练(手法固定-保持练习)。
进入下一阶段的标准: 您能自主完成完全且无痛的活动;强化训练后无疼痛或肿胀;且与对侧相比,力量正在均衡增长。
巨大撕裂——第四阶段:重返运动与工作(6个月及以上)
巨大撕裂患者重返运动和重体力劳动的时间较晚,通常为6个月或更久,且往往更长,回归过程更为缓慢且速度较慢。渐进过程与小/中型撕裂的轨迹相同,均采用分阶段、基于标准的方法。
- 吊带: 无需使用。
- 锻炼: 渐进式负荷训练及针对运动或工作的专项体能训练,逐步增加强度。
达到重返标准时: 经Hirpara医生和您的物理治疗师共同批准;您的旋转肌力至少达到对侧的85%;且具备完全、无痛的活动范围及耐力,在负荷下无反应性肿胀。预期需要6个月或更长时间(往往更长),决策应基于是否满足上述标准,而非仅依据日历时间。
重返运动与工作
对于所有修复手术,重返活动的标准是基于临床指标的(无痛,且具备足够的关节活动度、力量和耐力),并由 Hirpara 医生与您的物理治疗师共同签署确认,而非仅依据日历时间决定。
- 小型/中型撕裂: 久坐类工作可在数周内恢复;12–16 周后开始更重的力量训练;约 4–6 个月后重返运动或重体力劳动。
- 大型/巨大撕裂: 6 个月或更久,通常时间更长,恢复过程更为缓慢且谨慎。
对于过顶运动(overhead sports)和投掷类运动,在恢复 unrestricted play(无限制比赛/训练)前,需完成分级的间歇性训练计划。完全(最大)力量测试将推迟至术后 9–12 个月进行。
您的早期锻炼
这些是早期(保护)阶段的轻柔锻炼,从病房开始并延续至家中进行,操作时您的患侧手臂不在吊带内,且肩部肌肉放松。请按照物理治疗师的指导开始这些锻炼,若任何动作引起尖锐的肩部疼痛,请立即停止。这些锻炼内容位于上述各路径的“第一阶段”部分。
术后康复方案
本方案与诊所的一般术后恢复建议配合使用;详见术后疼痛管理和伤口护理。关于手术本身,请参阅肩袖修复术。
Evidence & references
Rotator Cuff Repair — Best-Evidence Rehabilitation Protocol
Scope: arthroscopic (and mini-open) rotator cuff repair (RCR). Two evidence sources combined: (1) local RAG corpus of 180,000+ Orthopaedic articles (citations below carry the journal/year), and (2) authoritative published institutional rehabilitation protocols (URLs below).
Each claim is flagged [STRONG] (RCT / meta-analysis / systematic review) or [CONSENSUS] (institutional protocol, narrative review, expert opinion) where relevant.
1. Consensus phased timeline (small/medium, "standard" 1–2 tendon repair)
Synthesised primarily from the Brigham & Women's Hospital (BWH) Arthroscopic RCR protocol and the BWH Standard of Care, cross-checked against the published institutional consensus. [CONSENSUS] for the exact week windows; [STRONG] that no specific week-by-week schedule is proven superior across all sizes (see controversies — Baumgarten 2009 Level I/II review; Chan 2014 meta-analysis).
| Phase | Weeks | Sling | ROM allowed | Active ROM | Strengthening | Precautions |
|---|---|---|---|---|---|---|
| I — Passive motion / protective ("healing") | 0–6 | Sling + small abduction cushion worn at all times, including sleep; remove only for exercise/icing/hygiene. Weaned wks 4–6. | PROM/AAROM only. Pendulums. Supine passive forward elevation to ~90–100°; passive ER (arm near side) to ~30°. Progress toward 120–140° FE / 30–60° ER by end of phase. | None. No active shoulder motion (tendon ~20% of normal strength at 4 wks). Active elbow/wrist/hand OK (curls only if biceps not involved). | Submaximal scapular + cuff setting; manual scapular work only. No resisted shoulder. | No active abduction/elevation; no pushing off with the arm for 6 wks; no NSAIDs >=12 wks (tendon healing). |
| II — Active-assisted -> active ROM | 6–12 | Discontinued (weaned wks 4–6). | Full PROM/AAROM to tolerance; supine->seated AAROM with cane/towel. | AAROM starts ~6 wks; AROM starts ~6–8 wks (gravity-eliminated -> upright). Goal >115° active FE before Phase III. | Begin light isotonic for deltoid, non-repaired cuff, scapula at ~10–12 wks (small tears); delayed to 16 wks for large/massive. | Avoid empty-can raises ever; no straight-arm lateral raises; light waist-level use only early. |
| III — Strengthening | 12–16 | None. | Should have full ROM with good stability. | Full active use for ADLs; return to full work + modified recreation. | Progressive cuff/scapular/deltoid strengthening; endurance/power. | <=5 lb lifting; no sudden jerk/push; thumb-up (full-can) raises only. |
| IV — Return to sport/work prep | 16–24 | None. | Maintain full ROM. | Sport/work-specific conditioning, plyometrics, progressive weight program. | Advanced/sport-specific strengthening. | <=10 lb until cleared; no painful progressions. |
| Return to sport / heavy work | >=4–6 months (often 6 mo; up to 12 mo for full recovery) | — | — | — | — | Surgeon + therapist clearance; pain-free, adequate ROM + endurance. |
Tendon-healing biology underpinning the schedule (BWH protocol): repair strength ~20% of normal at 4 wks, ~40% at 8 wks, ~60% at 12 wks, ~70% at 16 wks, ~80% at 32 wks — the rationale for no active motion before 6 wks and no strengthening before 12 wks. [CONSENSUS] (institutional, biologically grounded).
2. Small/medium vs large/massive tears (the key size distinction)
[STRONG] Tear size is the dominant modifier of healing/retear risk: weighted mean retear ~26.6% overall (Chamberlain/Namdari/Keener, What's New in Shoulder & Elbow Surgery, JBJS 2015), rising to ">90% in massive tears" (Hsu, Horneff, Gee, Immobilization After Rotator Cuff Repair, Orthop Clin North Am 2016). Retear correlates with larger tear size, advanced age, fatty infiltration.
| Variable | Small / medium (<3 cm, 1–2 tendons, good tissue) | Large / massive (>3–5 cm, >=2 tendons, poor tissue) |
|---|---|---|
| Sling/immobilizer duration | 4–6 wks | 6 wks (commonly), abduction pillow; some delay PT to 6 wks to protect healing |
| PT start | within first 6 wks | may be delayed up to 6 wks to promote healing (BWH hybrid protocol) |
| Active ROM start | ~6–8 wks | later, individualised; protect repair longer |
| Strengthening start | ~10–12 wks | delayed to ~16 wks |
| Return to sport/heavy work | 4–6 months | >=6 months, frequently longer; lower/slower return |
[STRONG] Review of online RCR protocols (Coda et al., Arthrosc Sports Med Rehabil 2020): for large/massive tears, sling/immobilizer use ranged 4–10 wks, with the plurality (~55%) at 6 wks. [STRONG] Substantial between-protocol variability exists (Galetta et al., J Shoulder Elbow Surg 2021, ACGME-program protocol survey; Coda 2020) — i.e., no single validated schedule; size-stratification is consensus-driven.
Return-to-work pooled data: [STRONG] Haunschild et al. (Am J Sports Med 2021) systematic review/meta-analysis quantifies return-to-work after primary RCR (timeline varies with job demand; heavy-labor return slower).
3. KEY CONTROVERSY — Early vs Delayed (immobilization) passive motion after arthroscopic RCR
This is the central evidence debate. Two competing concerns: early PROM reduces post-op stiffness; delayed/immobilization may protect tendon-to-bone healing (reduce retear), especially in larger tears.
Evidence FOR early passive motion (less stiffness, no proven healing penalty in small/medium)
- [STRONG] Keener et al. RCT — early vs delayed passive motion after arthroscopic repair of full-thickness tears, 114 patients, small-to-medium tears (cited in Braman/Neviaser/Parsons, What's New in Shoulder and Elbow Surgery, JBJS 2014): the landmark RCT in this debate; early motion improved early ROM without a clear healing penalty in this size class.
- [STRONG] Mazzocca et al. RCT (Arthroscopy 2017): no difference between delayed and early motion in WORC scores, clinical outcomes, or structural failure at 6 months; both protocols equivalent on patient-reported outcomes.
- [STRONG] Saltzman et al. (J Shoulder Elbow Surg 2017) — systematic review of overlapping meta-analyses: early-motion protocols may give superior early ROM; differences trend toward equivalence by ~1 year.
- [STRONG] Li et al. meta-analysis (Medicine 2018): early passive motion (EPM) gives superior ROM recovery, with the caveat below.
Evidence FOR delayed motion / immobilization (protect healing, lower retear in larger tears)
- [STRONG] Chan et al. meta-analysis (J Shoulder Elbow Surg 2014): documents the shift toward delaying motion over healing concerns; early motion improves ROM but raises healing-integrity questions.
- [STRONG] Li et al. meta-analysis (Medicine 2018): EPM "may adversely affect shoulder function" and "might result in lower rates of tendon healing in large-sized tears" — i.e., the early-motion benefit is size-dependent and may cost healing in big tears.
- [STRONG] Gallagher et al. systematic review (Phys Sportsmed 2015): early aggressive rehab may compromise repair integrity; conclusions size/quality dependent.
- [STRONG] Stillson et al. (J Am Acad Orthop Surg 2022, large Medicare cohort): strong association between starting PT within 1 week post-op and increased revision/revision-surgery rates — the largest study to date on rehab timing; cautions against very early aggressive therapy.
- Supporting basic-science: delayed early passive motion was harmless to cuff healing in animal models (rabbit model cited in Thigpen/Shaffer/Kissenberth, Clin Sports Med 2015, "Knowing the Speed Limit").
Current consensus
[STRONG/CONSENSUS] The meta-analytic bottom line (Mazzocca 2017 RCT; Saltzman 2017; Chan 2014): for small-to-medium tears, early and delayed PROM converge by ~6–12 months — timing is largely surgeon preference and does not change final outcome, so either is defensible. For large/massive tears (and poor tissue), the balance tips toward a delayed / protected approach to favor healing and lower retear (Li 2018; Hsu 2016), and very early (<1 wk) aggressive PT should be avoided (Stillson 2022). This is exactly the size-stratified pattern the BWH protocol encodes (delay PT/strengthening for large/massive). Note Cochrane-level certainty remains low — no protocol is proven superior on patient-important outcomes (Baumgarten 2009 Level I/II review found insufficient evidence for a single optimal protocol).
4. Practice shift to flag
- Historical default = early passive motion (minimize stiffness). Over the last decade the field moved toward delaying/protecting motion in larger tears on healing grounds (Chan 2014; Li 2018), then partially back toward equipoise for small/medium tears as RCTs/meta-analyses showed equivalent final outcomes (Mazzocca 2017; Saltzman 2017).
- Newest signal: avoid ultra-early (<1 week) PT regardless — associated with higher revision rates (Stillson 2022, Medicare cohort). Net current practice = size-stratified: standard 6-wk sling + passive-only phase, active ROM ~6–8 wks, strengthening ~12 wks for small/medium and ~16 wks for large/massive, RTS 4–6+ months.
CITATIONS
RAG corpus articles (title / journal / year)
- Keener et al. — early vs delayed passive motion after arthroscopic full-thickness RCR (small–medium, n=114). Cited in Braman J, Neviaser A, Parsons B. What's New in Shoulder and Elbow Surgery. J Bone Joint Surg. 2014;96(20). [STRONG — RCT]
- Mazzocca AD, Arciero RA, Shea KP, et al. The Effect of Early Range of Motion on Quality of Life, Clinical Outcome, and Repair Integrity After Arthroscopic Rotator Cuff Repair. Arthroscopy. 2017;33(6). [STRONG — RCT]
- Chan K, MacDermid JC, Hoppe DJ, et al. Delayed versus early motion after arthroscopic rotator cuff repair: a meta-analysis. J Shoulder Elbow Surg. 2014. [STRONG — meta-analysis]
- Saltzman BM, Zuke WA, Go B, et al. Does early motion lead to a higher failure rate or better outcomes after arthroscopic rotator cuff repair? A systematic review of overlapping meta-analyses. J Shoulder Elbow Surg. 2017;26(9):1681-1691. [STRONG]
- Li S, Sun H, Luo X, et al. The clinical effect of rehabilitation following arthroscopic rotator cuff repair (meta-analysis). Medicine. 2018. [STRONG — meta-analysis]
- Gallagher BP, Bishop ME, Tjoumakaris FP, et al. Early versus delayed rehabilitation following arthroscopic rotator cuff repair: A systematic review. Phys Sportsmed. 2015. [STRONG]
- Stillson QA, Sun JQ, Maninang M, et al. Effect of Physical Therapy and Rehabilitation Timing on Rotator Cuff Repair Revisions and Capsulitis. J Am Acad Orthop Surg. 2022 (large Medicare cohort). [STRONG]
- Baumgarten KM, Vidal AF, Wright RW. Rotator Cuff Repair Rehabilitation: A Level I and II Systematic Review. Sports Health. 2009 (insufficient evidence for a single optimal protocol). [STRONG]
- Parsons BO, Gruson KI, Chen DD, et al. Does slower rehabilitation after arthroscopic rotator cuff repair lead to long-term stiffness? J Shoulder Elbow Surg. 2010;19(7):1034-1039. [moderate]
- Thigpen CA, Shaffer MA, Kissenberth MJ. Knowing the Speed Limit. Clin Sports Med. 2015. [CONSENSUS/review]
- Chamberlain AM, Namdari S, Keener JD. What's New in Shoulder and Elbow Surgery? J Bone Joint Surg. 2015;97(20) (retear ~26.6%; predictors). [STRONG — pooled]
- Hsu JE, Horneff JG, Gee AO. Immobilization After Rotator Cuff Repair. Orthop Clin North Am. 2016 (retear up to >90% massive). [CONSENSUS/review]
- Coda RG, Cheema SG, Hermanns CA, et al. A Review of Online Rehabilitation Protocols Designated for Rotator Cuff Repairs. Arthrosc Sports Med Rehabil. 2020;2(3) (sling 4–10 wks; ~55% at 6 wks for large/massive). [STRONG — protocol systematic review]
- Galetta MD, Keller RE, Sabbag OD, et al. Rehabilitation variability after rotator cuff repair. J Shoulder Elbow Surg. 2021;30(6) (ACGME program protocol variability). [STRONG]
- Haunschild ED, Gilat R, Lavoie-Gagne O, et al. Return to Work After Primary Rotator Cuff Repair: A Systematic Review and Meta-analysis. Am J Sports Med. 2021. [STRONG]
Published institutional protocols (URLs)
- Brigham & Women's Hospital — Arthroscopic Rotator Cuff Repair Protocol (hybrid patient/therapist; full phased timeline, tear-size stratification): https://www.brighamandwomens.org/assets/BWH/patients-and-families/rehabilitation-services/pdfs/shoulder-arthroscopic-rct-repair-protocol-hybrid-patient-therapist.pdf
- Brigham & Women's Hospital — Standard of Care: Arthroscopic repair of a rotator cuff tear (small/medium/large-massive protocol families; literature review): https://www.brighamandwomens.org/assets/BWH/patients-and-families/rehabilitation-services/pdfs/shoulder-rotator-cuff-repair-arthroscopic.pdf
Overall evidence grade: the biology-based phase structure is [CONSENSUS] (well-aligned across institutions). The early-vs-delayed motion question is supported by multiple [STRONG] RCTs and meta-analyses, which converge on equivalence for small/medium tears and a protect-healing tilt for large/massive — but Cochrane-level certainty for any single optimal schedule remains LOW.





