de Quervain's Release Info Evidence
Reviewed by Dr Kieran Hirpara, Specialist Orthopaedic Surgeon Last reviewed
This protocol guides your recovery after a de Quervain's release, a small operation that opens the tight tunnel over the thumb-side tendons of your wrist, with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It begins with your home exercise program, followed by the structured clinical protocol written for your hand therapist; bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your hand therapist may adjust the plan depending on how your recovery progresses.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect
De Quervain's tenosynovitis is irritation of the two tendons that run to your thumb (the abductor pollicis longus and extensor pollicis brevis) where they pass through a snug tunnel (the first dorsal compartment) on the thumb side of the wrist. The release is a small operation that opens that tunnel so the tendons have room to glide freely, settling the pain and catching.
Because nothing is stitched back together or tightened (the tunnel is simply opened and is meant to stay open), this is an early-motion recovery, not a long protected one. There is no construct that needs months of healing. The whole aim of the rehabilitation is to keep the tendons moving through the healing surgical bed so they do not stick down, while the small wound and the skin nerves over it settle.
So the plan is simple: a soft dressing (sometimes a light thumb splint just for comfort) for the first few days to about a week or two, gentle thumb and wrist movement started early, scar care once the wound is healed, and a gradual build-up of grip and pinch strength. Most people are back to comfortable normal activity by around four to six weeks.
Two things are watched after this particular operation. The first is a small skin nerve, the radial sensory nerve, whose branches run right across the front of the surgical site; it can be left tingly or tender for a while, and the early nerve-settling work is aimed at it. The second is the position of the tendons: opening the tunnel too far towards the palm side can occasionally let a tendon slip forwards (subluxate) when you move the thumb. Both are uncommon, and your hand therapist will keep an eye out for them.
Precautions and limitations
- Keep the thumb and wrist moving from the start: gentle movement is the treatment here, not rest. Stiffness from doing too little is the main thing we are trying to avoid.
- Use any comfort splint only as directed and only for the first days to a week or two: it is for comfort, not protection, and should come off for your exercises.
- Keep the wound clean and dry until it is healed; do not start scar massage until the dressings are off and the skin is closed.
- Avoid heavy gripping, forceful pinching, lifting and twisting (wringing a cloth, opening tight jars, heavy tools) until around three to four weeks, then build back up gradually.
- Tell your therapist or the rooms if you notice tingling, numbness or a sharp shooting feeling over the back of the thumb and wrist, or a tendon that snaps or slips when you move the thumb.
For wound, swelling and scar management, see the practice's wound care guidance.
Your exercises
Kieran Hirpara 4.0
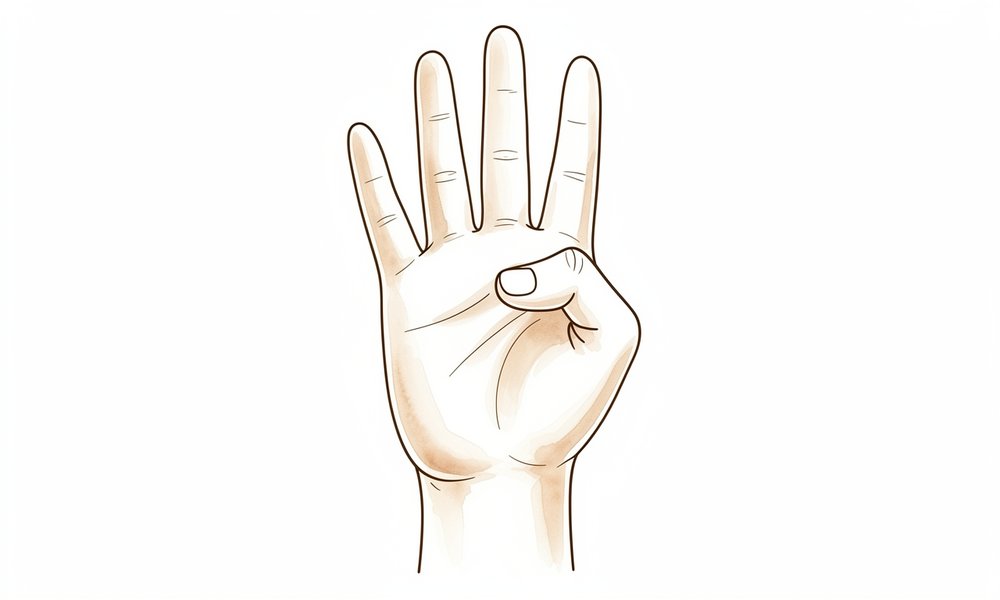
Thumb movement (bend, straighten and reach)
Gently move your thumb through its full range: bend the tip down towards your palm, straighten it out, then move the whole thumb across to touch the base of your little finger and back out wide. Keep it slow and comfortable. Early thumb movement keeps the released tendons gliding so they do not stick down in the healing scar.
10 of each, 3–4 times a day, within comfort
Kieran Hirpara 4.0
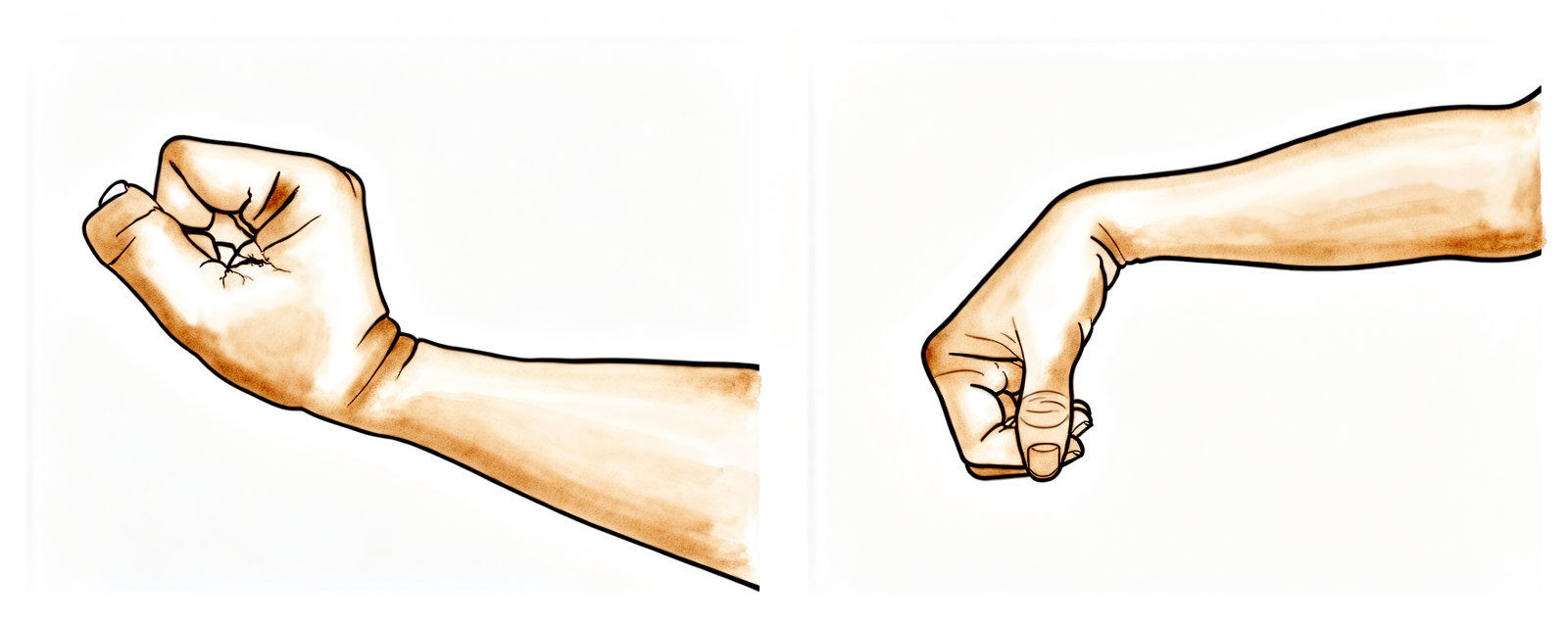
Wrist movement (up, down and side to side)
With your forearm resting on a table, gently bend the wrist up and down, then tilt it side to side (towards the thumb, then towards the little finger). Move only as far as is comfortable. This keeps the wrist supple while the wound settles.
10 each direction, 3–4 times a day

Kieran Hirpara 4.0
Tendon glides (thumb and finger gliding)
Open your hand wide, then slide the thumb across to touch each fingertip in turn, then make a loose fist and open again. The aim is smooth gliding, not force. Keeping the tendons moving through the released tunnel is the single most important thing in the early weeks to avoid stiffness and adhesions.
5–10 slow cycles, 3–4 times a day
Kieran Hirpara 4.0
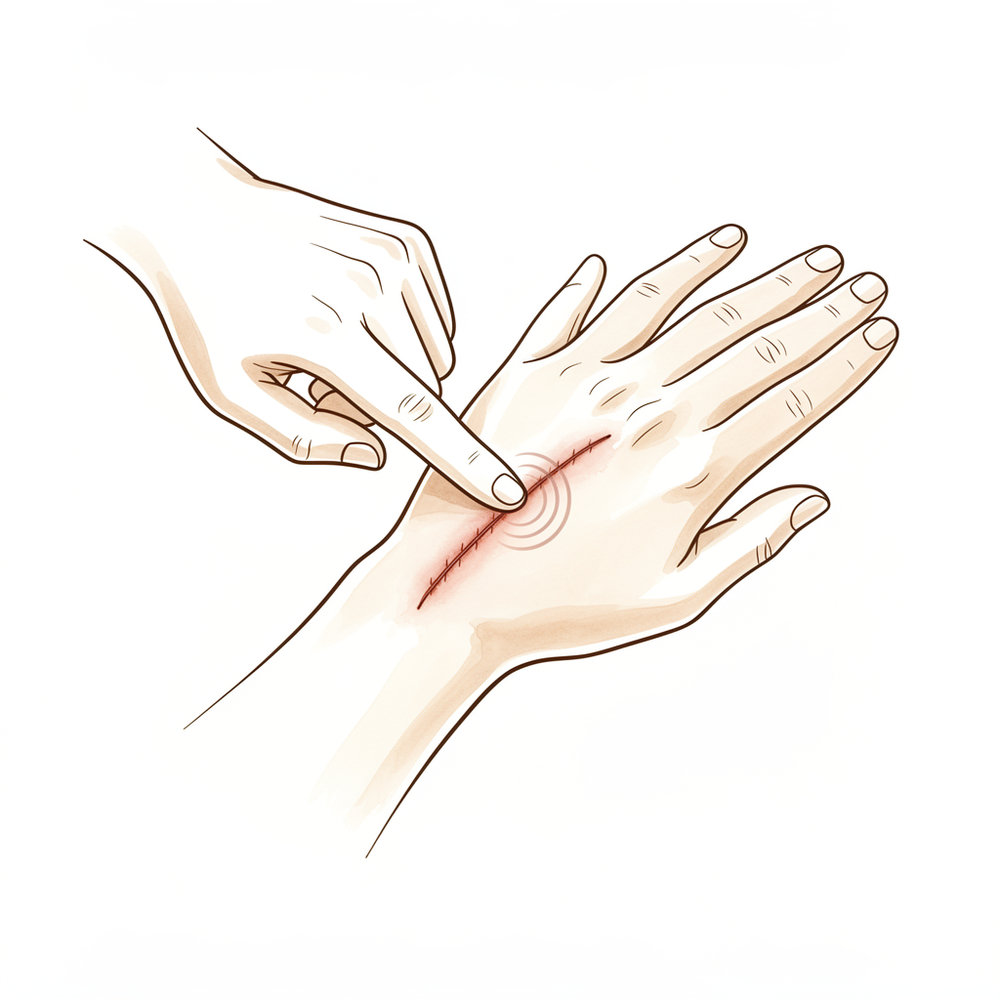
Scar massage
Once the wound is fully healed and the dressings are off (commonly from around two weeks), rub a little plain moisturiser into the scar with small firm circles for a minute or two. This softens the scar and helps the skin and the tender nerve branches underneath settle. Stop if the area is still open or weepy.
1–2 minutes, 2–3 times a day, once healed

Kieran Hirpara 4.0
Grip and pinch strengthening
A LATER exercise — usually from around three to four weeks, once the wound has healed and movement is comfortable. Squeeze a soft ball or therapy putty for grip, and pinch a small piece of putty between your thumb and fingertips for pinch. Build the effort up gradually. This rebuilds the strength that always dips after surgery.
10–15 squeezes/pinches, 2–3 times a day (from ~3–4 weeks)
Kieran Hirpara 4.0
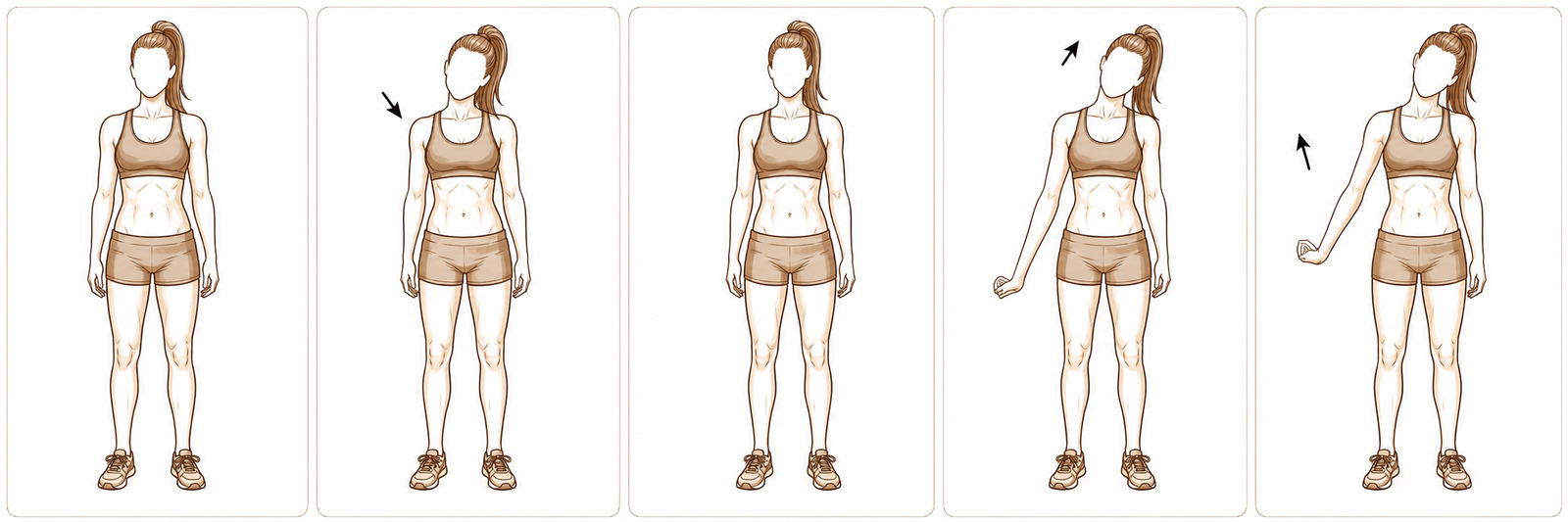
Radial nerve glide (if the wrist-back feels tingly or tender)
Only if your hand therapist starts it — for tingling, tenderness or sensitivity over the back of the thumb and wrist. With the arm out in front, gently ease the wrist and thumb down into a light stretch until you feel a mild pull, hold a moment, then release. It should never be painful or make the tingling worse. This calms the small skin nerve that runs right over the operation site.
5–10 slow glides, 1–2 times a day, only as guided
These are the exercises from your handout. Start them as guided by Dr Hirpara and your hand therapist. The early exercises (thumb movement, wrist movement and tendon glides) keep everything moving and gliding so the released tendons do not stick down; these begin within the first days, within comfort. Scar massage starts once the wound is healed. Grip and pinch strengthening is a later addition, usually from around three to four weeks. The nerve glide is only added if the skin over the wrist feels tingly or tender. Stop anything that causes sharp or shooting pain over the thumb side of the wrist.
Your clinical protocol
The rest of this page is the staged clinical protocol for rehabilitation after de Quervain's (first dorsal compartment) release. This section is to be provided to your hand therapist, and each phase opens with a plain-English explanation of what is happening. This is a decompression, not a repair: the first dorsal compartment is divided and is meant to stay divided, so there is no construct to protect. The programme is therefore an early-motion, glide-based pathway: keep the APL/EPB tendons gliding through the surgical bed to prevent adhesion, control oedema, manage the scar and the radial sensory nerve, and restore grip and pinch.
Prior to treatment, check the patient's operation report and liaise with the treating surgeon regarding the release (longitudinal/dorsal incision, whether a separate EPB sub-sheath/septum was found and released), the dorsal positioning of the release to protect against volar tendon subluxation, and any radial sensory nerve handling. Dr Hirpara performs an open release through a dorsal/longitudinal approach, protecting the radial sensory nerve branches and keeping the release dorsal to avoid volar subluxation; immobilisation is for comfort only (soft dressing ± short thumb spica for a few days to ~1–2 weeks), and early thumb and wrist motion is the default.
Phase I — early motion, oedema and wound care (week 0 to ~2)
The first week or two protect the wound and settle swelling while motion starts immediately. There is no protected arc to respect: the goal is to get the released tendons gliding straight away. Any splint is for comfort only and comes off for exercises.
For your hand therapist:
Education and precautions - This is a decompression: no construct to protect; early active motion is the intended default - Comfort support only: soft dressing ± short thumb spica for the first few days to ~1–2 weeks; off for exercises and washing - Keep the wound clean and dry until healed; defer scar work until skin is closed - Avoid forceful grip, pinch, lifting and wrist twisting in this window - Screen the radial sensory nerve distribution (dorsoradial thumb/wrist) for paraesthesiae, hypersensitivity or Tinel's; screen for APL/EPB subluxation on resisted/active thumb extension–abduction
Management - Wound: surgical dressings as directed; monitor for infection - Oedema: elevation, gentle retrograde massage, ice as needed - Exercises: active thumb ROM (flexion/extension, palmar + radial abduction, opposition), active wrist ROM, APL/EPB tendon glides, full active finger ROM; light functional hand use within comfort
Criteria to progress - Wound healed/settling; swelling controlled; comfortable active thumb and wrist motion
Phase II — restoring motion and scar management (weeks ~2 to 4)
Once the wound is healed, the comfort splint is discarded and the focus shifts to full, comfortable motion plus active scar and nerve desensitisation. Light strengthening begins towards the end of this window.
For your hand therapist:
Assessments - Thumb and wrist active/passive ROM; scar quality; radial sensory nerve symptoms; subluxation screen
Education and precautions - Discontinue any comfort splint; encourage normal light hand use - Continue to avoid heavy/forceful grip and pinch until ~3–4 weeks
Management - Scar: massage and silicone/moisturiser once healed; desensitisation if hypersensitive - Nerve: radial sensory nerve glides/desensitisation if irritable; settle before loading - Exercises: progress to full thumb and wrist ROM; continue tendon glides; begin light grip/pinch (putty, soft ball) from ~3–4 weeks
Criteria to progress - Full, pain-free thumb and wrist ROM; healed, mobile scar; settling nerve symptoms
Phase III — strengthening and return to activity (weeks ~4 to 6 and beyond)
With motion restored and the wound mature, grip and pinch are built up and the patient is returned to full activity. Most reach comfortable normal use by around four to six weeks; heavier manual demands take a little longer and are criterion-based.
For your hand therapist:
Assessments - Grip and pinch strength versus the other side; pain with loading; functional/work-specific testing as appropriate
Education and precautions - Graded return to gripping, pinching, lifting and twisting; full activity as comfort and strength allow - Persisting dorsoradial pain/tingling or a snapping tendon → refer back to the treating surgeon (consider neuroma, incomplete release, or volar subluxation)
Management - Exercises: progressive grip and pinch strengthening; task- and work-specific loading; continue any residual scar/nerve work - Consider discharge once strength is near-symmetrical and function is restored - Consider referral back to the treating doctor if recovery plateaus or there is a poor outcome
Criteria for discharge / return to full activity - Near-symmetrical grip and pinch; pain-free functional and work-specific use
Getting back to work and activity
Light everyday hand use (eating, writing, dressing, light tasks) is encouraged from the start, within comfort. Because the operation is on the wrist and the hand needs to move freely and grip safely, driving resumes once the wound is comfortable, any comfort splint is off, and you can grip and turn the wheel confidently, for most people within the first week or two, as confirmed at your review.
Forceful gripping, pinching, lifting and twisting wait until around three to four weeks and are then built up gradually. Desk and light work often resume within days to a week or two; heavier manual work that depends on strong, repeated thumb and wrist loading is usually back by around four to six weeks, judged by your regained strength and comfort rather than the calendar alone, by Dr Hirpara and your hand therapist.
After your protocol
This protocol works alongside the practice's general recovery advice: see managing post-operative pain, wound care and scar management. The phased plan above reflects published rehabilitation guidance after de Quervain's release, and your ongoing recovery is guided individually by Dr Hirpara and your hand therapist according to how your hand progresses.
Evidence & references
Topic scope: post-operative rehabilitation after surgical release of the first dorsal compartment of the wrist (abductor pollicis longus, APL, and extensor pollicis brevis, EPB) for refractory de Quervain's tenosynovitis. This is a decompression, not a reconstruction: the fibro-osseous tunnel is opened and is meant to stay open, so the rehabilitation is an early-motion pathway built around tendon gliding, oedema and scar control, and protection of the overlying radial sensory nerve — rather than months of protected healing.
Defining principle of the rehab here: de Quervain's release relieves a tendon entrapment and does not create a construct that needs protection. The divided extensor retinaculum is meant to stay divided. So (unlike a tendon or ligament repair) immediate, gentle active thumb and wrist motion is the default, and the only deliberate restraints are brief comfort support and a short window of heavy-grip/pinch/twist avoidance while the wound heals. The therapy programme exists to keep the APL/EPB tendons gliding through the healing surgical bed so they do not adhere, to settle the radial sensory nerve branches that cross the incision, and to rebuild grip and pinch — not to immobilise. The single branch points are (1) whether a separate EPB sub-sheath/septum was present and released (its retention is a classic cause of failed release) and (2) keeping the release dorsal so the tendons do not subluxate volarly.
A. PROCEDURE OUTCOMES (open release; endoscopic and retinaculum-sparing variants)
Surgical release of the first dorsal compartment is a reliable operation for de Quervain's that has failed non-operative care: the great majority of patients obtain durable symptom relief, and the principal debates are over technique details (incision orientation, completeness of EPB sub-sheath release, whether to preserve/lengthen the retinaculum) rather than whether to decompress.
- Open release gives durable, high-quality long-term outcomes. A series of 80 cases with a mean 9.5-year follow-up reported sustained relief with a low complication profile, establishing the long-term reliability of open release [Garçon et al., Orthop Traumatol Surg Res 2018]. Moderate (long-term cohort).
- Functional recovery is good and objectively measurable. A series using DASH scores to evaluate first-extensor-compartment release for refractory disease documented good functional outcomes, and emphasised identifying and releasing a separate EPB sub-compartment (septum) when present [Lee et al., Clin Orthop Surg 2014]. DASH is a validated, widely used outcome instrument across hand and wrist conditions [Baltzer, Novak & McCabe, J Hand Surg Am 2014 — scoping review]. Moderate (cohort) + instrument SR.
- Endoscopic and open release are broadly comparable. A comparative study of endoscopic versus open release found favourable results for the endoscopic approach with attention to the radial sensory nerve, while open release remains the standard reference technique [Kang et al., Bone Joint J 2013]. Moderate (comparative).
- The retinaculum can be partly resected, simply divided, or reconstructed. Partial resection of the extensor retinaculum gives good short-term results [Altay et al., Orthop Traumatol Surg Res 2011]; simple release and Z-plasty (retinaculum-lengthening) reconstruction give comparable outcomes, with Z-plasty proposed to reduce subluxation risk at the cost of complexity [Kim, Baek & Lee, J Hand Surg Eur 2019]. A longitudinal-incision technique series likewise reports good functional outcomes [Mangukiya et al., Musculoskelet Surg 2019]. Moderate (comparative/cohort).
- Dissatisfaction does occur and is worth counselling for. A focused study of dissatisfaction after first dorsal compartment release found that a minority of patients remain dissatisfied, often linked to residual pain, nerve symptoms or incomplete relief — a reminder that outcomes are good but not universal [Rogozinski & Lourie, J Hand Surg Am 2016]. Moderate (cohort).
B. REHABILITATION / THERAPY EVIDENCE
The central rehab questions are (1) whether to immobilise the thumb/wrist afterwards and for how long, and (2) whether formal hand therapy changes the outcome. The published base specific to post-de-Quervain-release rehabilitation is thin and consensus-driven: there are no high-quality trials comparing immobilisation regimens or therapy protocols. Practice converges on brief comfort support and early motion, with hand therapy used selectively.
- Early motion is the rationalised default; prolonged immobilisation is not supported. Because the release is a decompression with no construct to protect, early active thumb and wrist motion is used to keep the APL/EPB tendons gliding and prevent adhesion. Immobilisation, where used, is a soft dressing or short thumb spica for comfort only for days to ~1–2 weeks. The supporting evidence is mechanistic/consensus, mirroring the well-established early-motion rationale after other upper-limb decompressions. Weak–moderate (mechanism strong, outcome data sparse).
- De Quervain's is not always an isolated problem — therapy assessment matters. A hand-therapy review highlights that de Quervain's syndrome may coexist with other dorsoradial/wrist pathology, so post-operative therapy should reassess rather than assume a single diagnosis — relevant when symptoms persist after release [Redvers-Chubb, Hand Therapy 2015]. Consensus (narrative/therapy review).
- Hand therapy focus is glide, scar and nerve, then strength. The programme priorities are tendon gliding (adhesion prevention), oedema control, scar management and radial sensory nerve desensitisation, and graded grip/pinch strengthening. The benefit of formal supervised therapy over a home programme is not established by trial data; selective therapy is defensible. Weak / consensus.
Recovery trajectory (expected, evidence-anchored)
| Phase | Window | Restraint | Hand use / therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Early motion, oedema & wound care | Week 0–~2 | Comfort support only (soft dressing ± short thumb spica) | Immediate active thumb + wrist motion; APL/EPB tendon glides; elevation/oedema control; screen radial sensory nerve + subluxation | Light functional use only | No construct to protect; motion is the treatment. Keep wound clean/dry |
| II — Restore motion & scar/nerve care | Week ~2–4 | Splint discarded once healed | Full thumb + wrist ROM; scar massage once wound healed; radial sensory nerve glides/desensitisation if irritable | Begin light grip/pinch (putty, ball) from ~3–4 wk | Avoid forceful grip/pinch/twist until ~3–4 wk |
| III — Strengthening & return | Week ~4–6+ | Restrictions lifted, graded | Progressive grip/pinch and task-specific loading | Return to near-symmetrical grip/pinch; full activity as strength allows | Light/desk work days–1–2 wk; manual work ~4–6 wk, criterion-based |
(Phase windows are typical clinical guides, not trial-derived deadlines. Driving resumes once the wound is comfortable, any comfort splint is off, and the patient can grip and steer confidently — commonly within 1–2 weeks.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY
- The EPB sub-sheath (septum) must be sought and released. A separate EPB sub-compartment is common and, if missed, is a classic cause of persistent symptoms / failed release. Series that emphasise identifying and releasing it report good outcomes [Lee 2014]. Moderate — strong mechanistic consensus.
- Volar tendon subluxation if released too volar. Dividing the retinaculum too far towards the palmar side can let the APL/EPB tendons subluxate volarly with thumb motion. Keeping the release dorsal, and retinaculum-lengthening (Z-plasty) reconstructions, are described specifically to mitigate this [Kim 2019; Altay 2011]. Moderate (technique-comparative).
- Radial sensory nerve injury is the signature complication. The superficial radial nerve branches cross the operative field; injury or scar entrapment produces dorsoradial numbness, hypersensitivity or painful neuroma and is a leading driver of dissatisfaction [Ilyas et al., J Am Acad Orthop Surg 2007; Rogozinski 2016]. Careful exposure with nerve protection is emphasised across open and endoscopic techniques [Kang 2013]. Moderate.
- Immobilise or move early? No trial settles the optimal post-operative regimen; consensus favours brief comfort support and early motion (decompression logic) over prolonged splinting. Weak — consensus, not trial-derived.
- Outcomes are good but not universal. A measurable minority remain dissatisfied, usually from residual pain, nerve symptoms or incomplete release — worth explicit pre-operative counselling [Rogozinski 2016]. Moderate.
D. EVIDENCE STRENGTH FLAGS (summary)
- MODERATE (cohort / comparative): durable long-term relief from open release (9.5-yr cohort); good DASH-measured functional outcomes; comparability of endoscopic vs open and of simple release vs Z-plasty / partial retinaculum resection; radial sensory nerve injury as the signature complication; a real, defined dissatisfaction rate.
- WEAK / CONSENSUS: the early-motion, glide-based rehabilitation programme itself (mechanistically rationalised; no trial comparing immobilisation regimens or therapy protocols after de Quervain's release); the role of formal supervised therapy vs a home programme; exact phase timings and return-to-activity windows (typical guides, not trial-derived). Outcomes and the two signature complications (radial sensory nerve injury; volar subluxation) are better studied than the rehabilitation protocol.
CITATIONS
RAG corpus (180,000+ Orthopaedic articles)
- Garçon JJ, Charruau B, Marteau E, et al. Results of surgical treatment of De Quervain's tenosynovitis: 80 cases with a mean follow-up of 9.5 years. Orthop Traumatol Surg Res. 2018. DOI: 10.1016/j.otsr.2018.04.022 (PMID 29909297)
- Lee HJ, Kim PT, Aminata IW, et al. Surgical Release of the First Extensor Compartment for Refractory de Quervain's Tenosynovitis: Surgical Findings and Functional Evaluation Using DASH Scores. Clin Orthop Surg. 2014. DOI: 10.4055/cios.2014.6.4.405
- Ilyas AM, Ast M, Schaffer AA, et al. de Quervain Tenosynovitis of the Wrist. J Am Acad Orthop Surg. 2007. DOI: 10.5435/00124635-200712000-00009 (PMID 18063716)
- Kang HJ, Koh IH, Jang JW, et al. Endoscopic versus open release in patients with de Quervain's tenosynovitis. Bone Joint J. 2013. DOI: 10.1302/0301-620X.95B7.31486 (PMID 23814248)
- Altay M, Ertürk C, Işıkan UE. De Quervain's disease treatment using partial resection of the extensor retinaculum: A short-term results survey. Orthop Traumatol Surg Res. 2011. DOI: 10.1016/j.otsr.2011.03.015
- Kim J, Baek J, Lee J. Comparison between simple release and Z-plasty of retinaculum for de Quervain's disease: a retrospective study. J Hand Surg Eur Vol. 2019. DOI: 10.1177/1753193418818341 (PMID 30669923)
- Mangukiya HJ, Kale A, Mahajan NP, et al. Functional outcome of De Quervain's tenosynovitis with longitudinal incision in surgically treated patients. Musculoskelet Surg. 2019. DOI: 10.1007/s12306-018-0585-1
- Rogozinski B, Lourie GM. Dissatisfaction After First Dorsal Compartment Release for de Quervain Tendinopathy. J Hand Surg Am. 2016;41(1). DOI: 10.1016/j.jhsa.2015.09.020 (PMID 26481556)
- Baltzer H, Novak CB, McCabe SJ. A Scoping Review of Disabilities of the Arm, Shoulder, and Hand Scores for Hand and Wrist Conditions. J Hand Surg Am. 2014. DOI: 10.1016/j.jhsa.2014.07.050 (PMID 25227601)
- Redvers-Chubb K. De Quervain's syndrome: It may not be an isolated pathology. Hand Therapy. 2015. DOI: 10.1177/1758998315599796
de Quervain's release literature (URLs)
- Lee HJ, et al. Surgical Release of the First Extensor Compartment for Refractory de Quervain's Tenosynovitis (DASH outcomes; EPB septum). Clin Orthop Surg 2014 (open access). https://doi.org/10.4055/cios.2014.6.4.405
- Garçon JJ, et al. Results of surgical treatment of De Quervain's tenosynovitis: 80 cases, mean 9.5-year follow-up. Orthop Traumatol Surg Res 2018. https://doi.org/10.1016/j.otsr.2018.04.022
- Ilyas AM, et al. de Quervain Tenosynovitis of the Wrist (review — radial sensory nerve, surgical technique, complications). J Am Acad Orthop Surg 2007. https://doi.org/10.5435/00124635-200712000-00009
- Rogozinski B, Lourie GM. Dissatisfaction After First Dorsal Compartment Release for de Quervain Tendinopathy. J Hand Surg Am 2016. https://doi.org/10.1016/j.jhsa.2015.09.020





