Inpatient exercises — shoulder replacement Info Evidence
Reviewed by Dr Kieran Hirpara, Specialist Orthopaedic Surgeon Last reviewed
These are the gentle exercises to begin in hospital after your shoulder replacement (total, reverse, or replacement for a fracture). They keep the hand, elbow and shoulder moving while the repair settles.
Your exercises
Kieran Hirpara 4.0
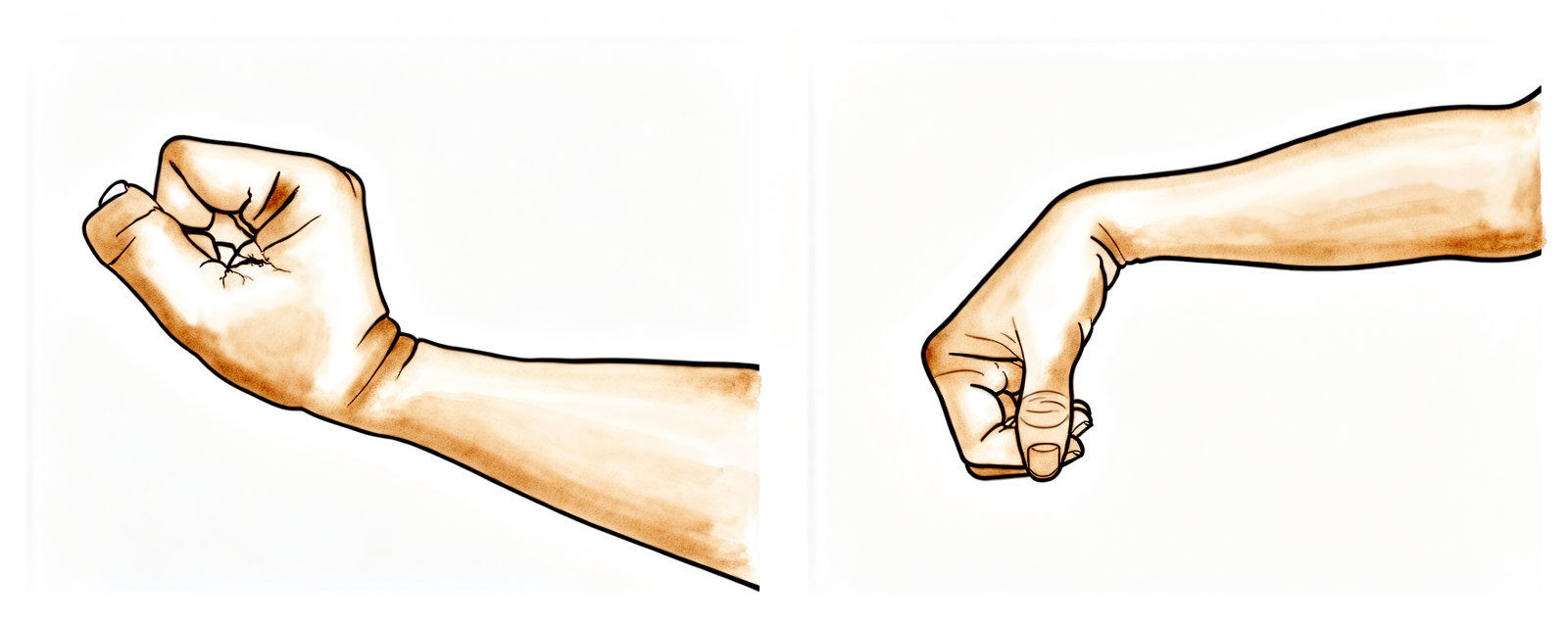
Wrist movement
Keep your hand moving by bending your wrist forwards, backwards and side to side.
10 times, 3 times per day
Kieran Hirpara 4.0
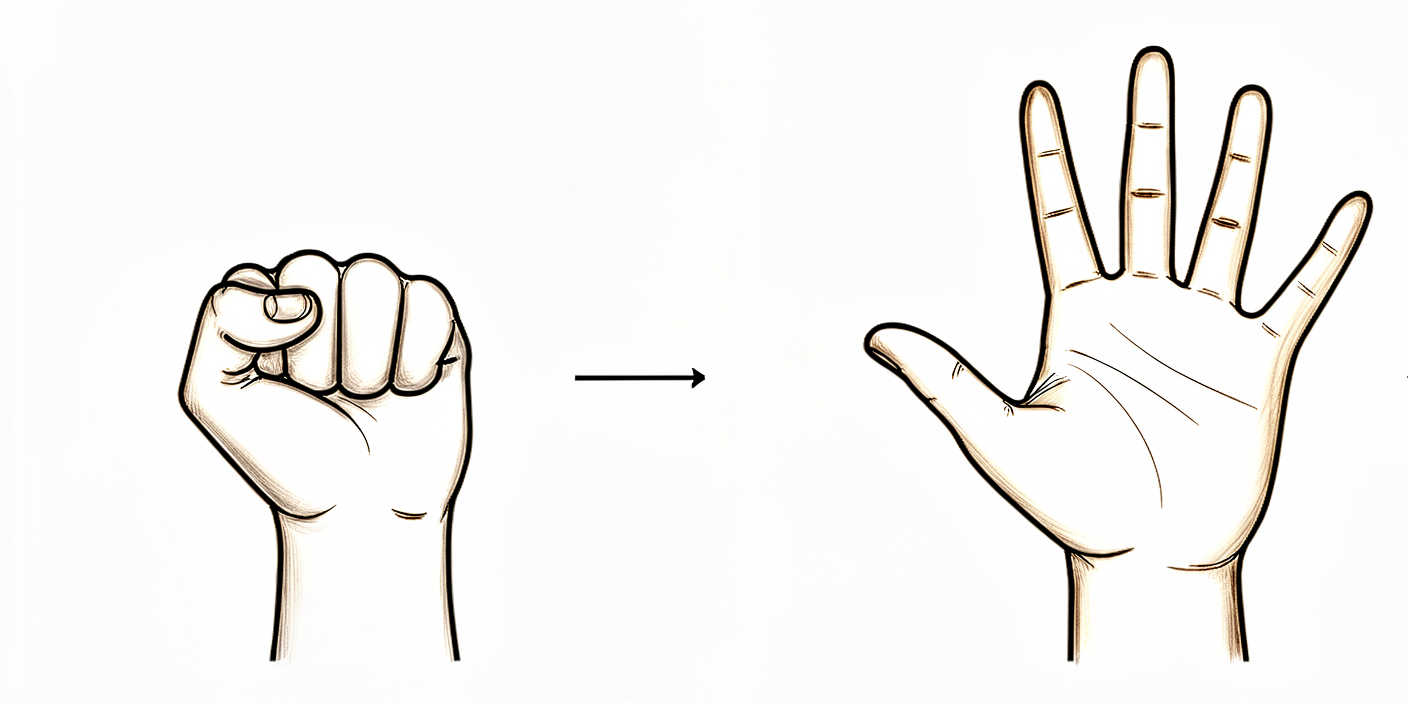
Open and close hand
Keep your hand and fingers moving by opening and closing them, or by squeezing a stress ball.
10 times, 3 times per day

Kieran Hirpara 4.0
Elbow bends
Bend and straighten your elbow.
10 times, 3 times per day
Kieran Hirpara 4.0
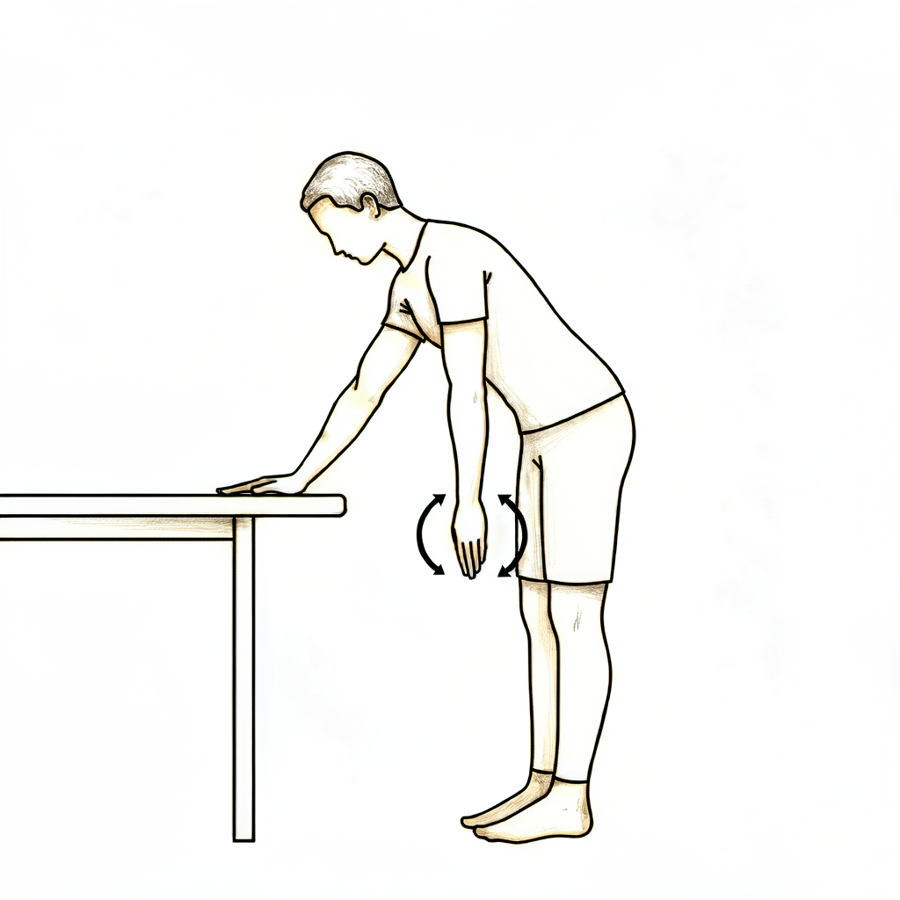
Pendulums
This is a passive exercise. Lean forward and let your arm relax down. Use your body to move the arm gently either clockwise or anti-clockwise, along with forwards, backwards and side to side.
About 30 seconds each way, 3 times per day
Kieran Hirpara 4.0
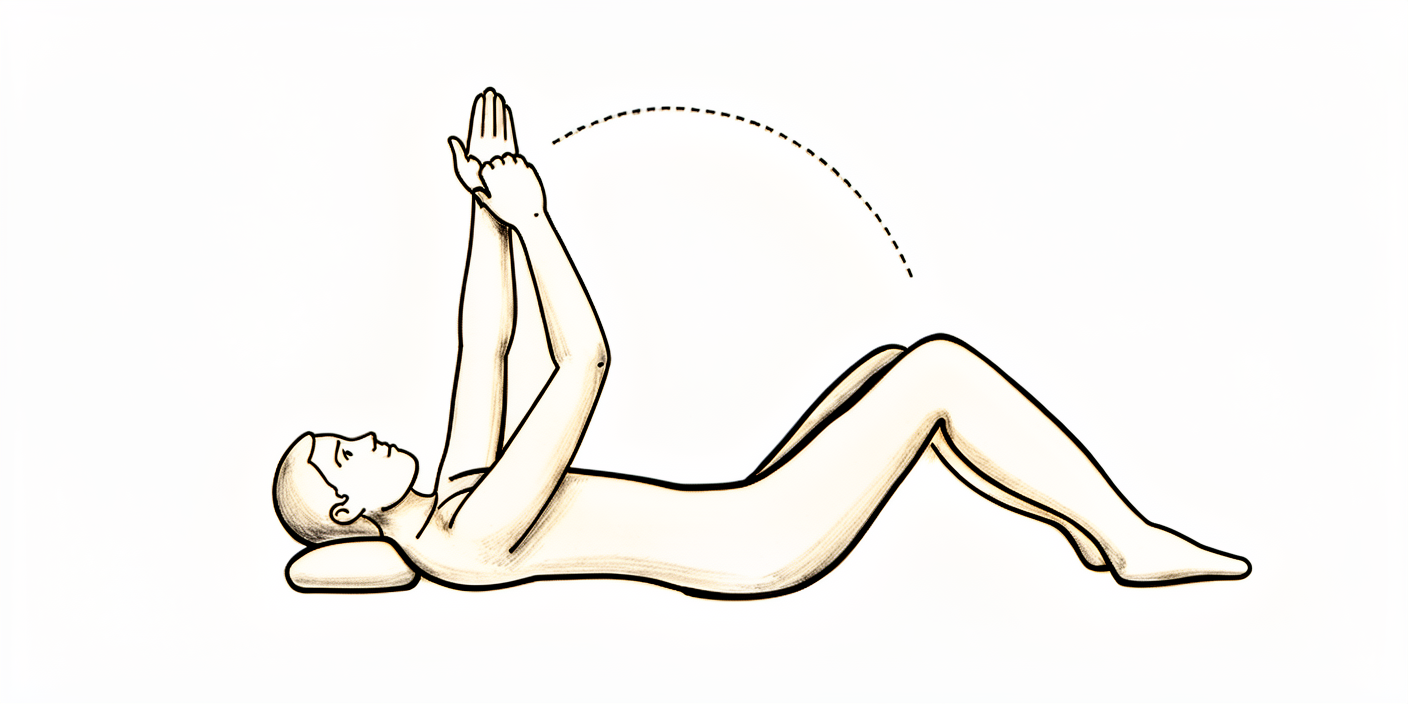
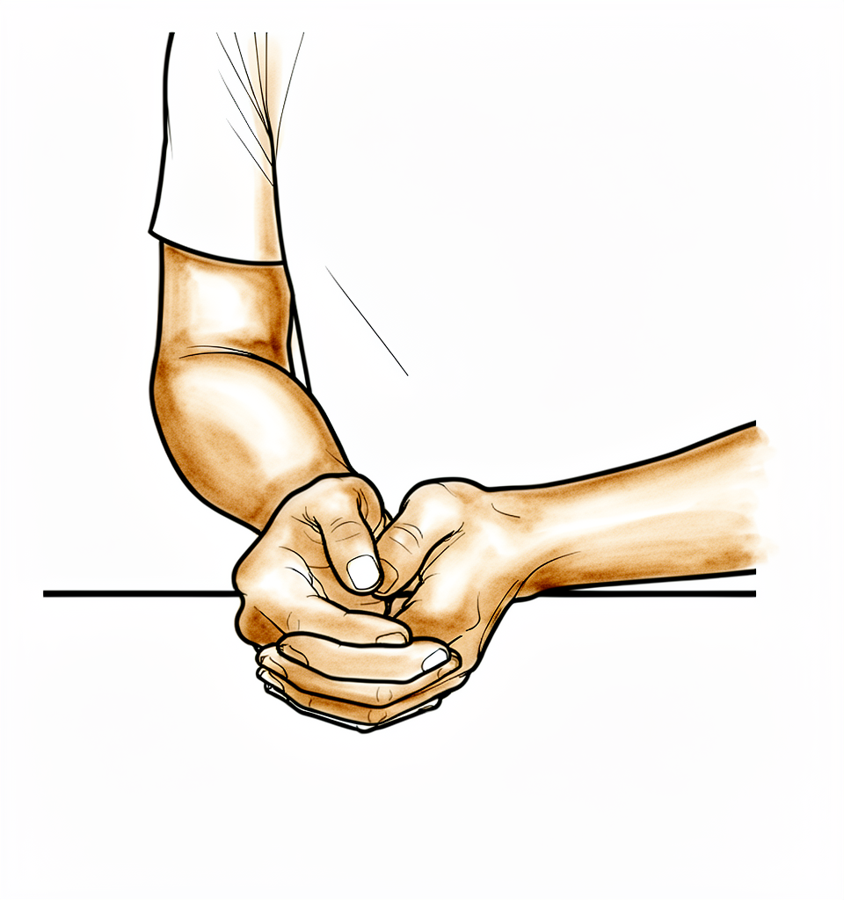
Assisted forward flexion
Sitting on a chair and leaning forward, cradle your operated arm with the other arm and gently move it upwards in front of you. Lower it back down with the help of your non-operated arm. You could also lie on your back in bed and help the arm upwards if you prefer.
10 times, 3 times per day

Kieran Hirpara 4.0
Assisted abduction
Sitting on a chair and leaning forward, cradle the arm again and help it out to the side (like rocking a baby).
10 times, 3 times per day
Kieran Hirpara 4.0
External rotation
Sitting on a chair, only move your arm from where it sits in the sling to pointing straight in front of you. Don't go further outwards.
10 times, 3 times per day
Kieran Hirpara 4.0
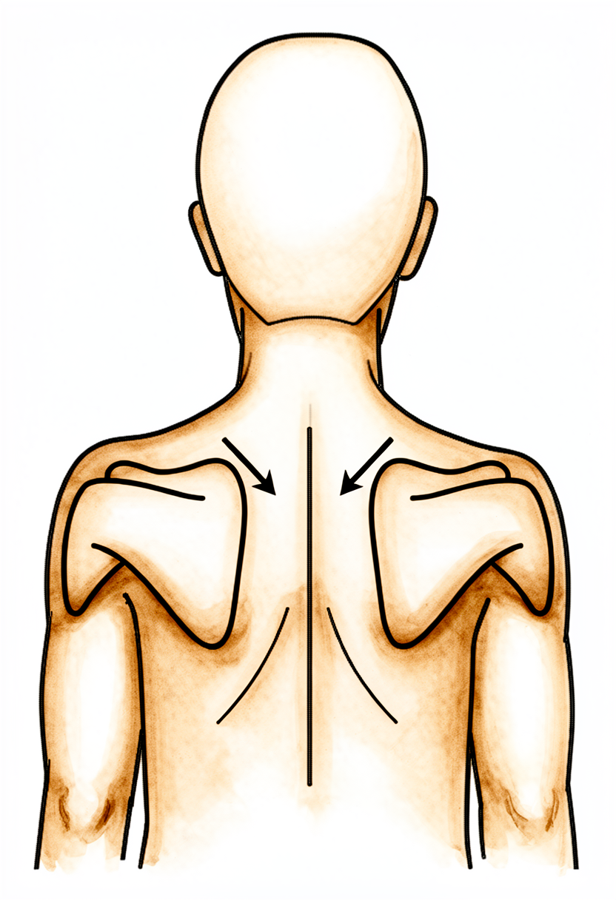
Lower trapezius setting
Squeeze your shoulder blades downwards and together.
Hold 5 seconds, 5 times, 3 times per day
Kieran Hirpara 4.0
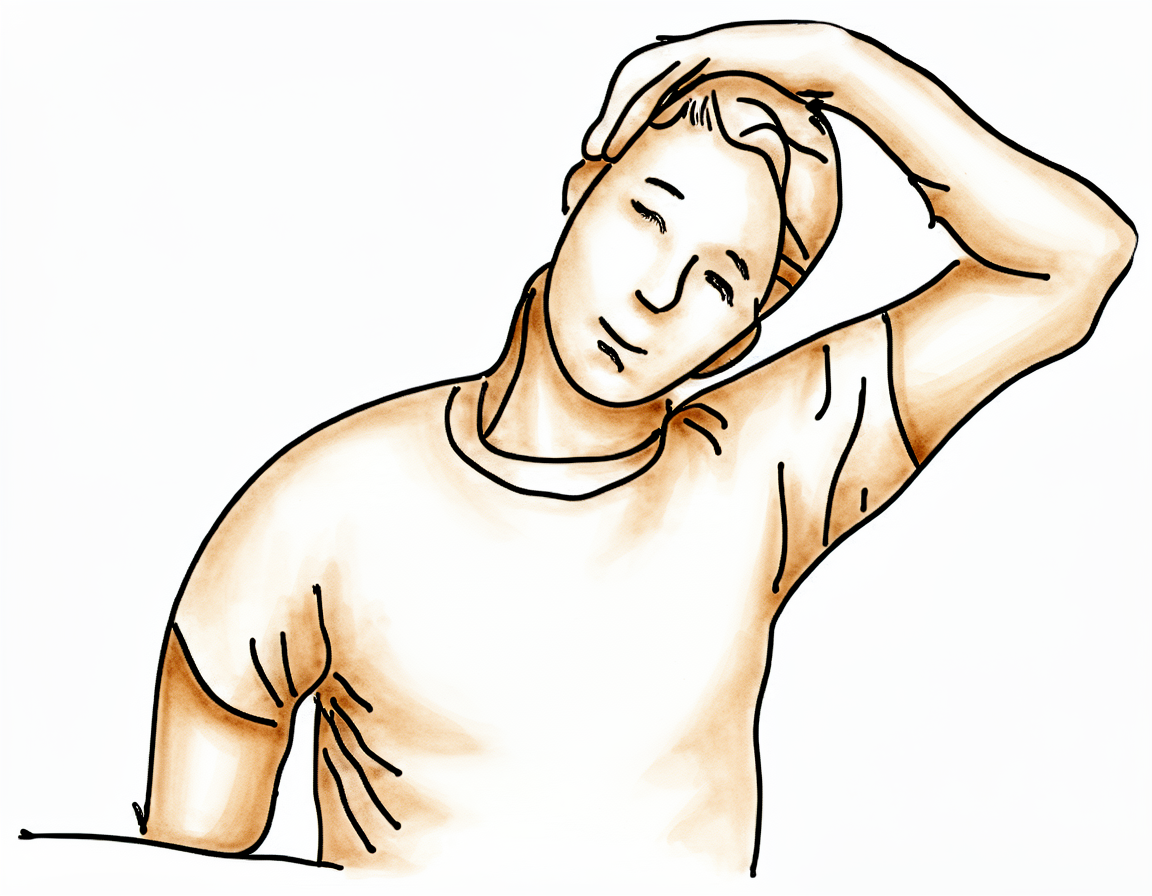
Upper trapezius stretch
Use your non-operated arm to bring your ear towards your shoulder, away from the operated side.
Hold 10 seconds, 3 times, 3 times per day
Kieran Hirpara 4.0
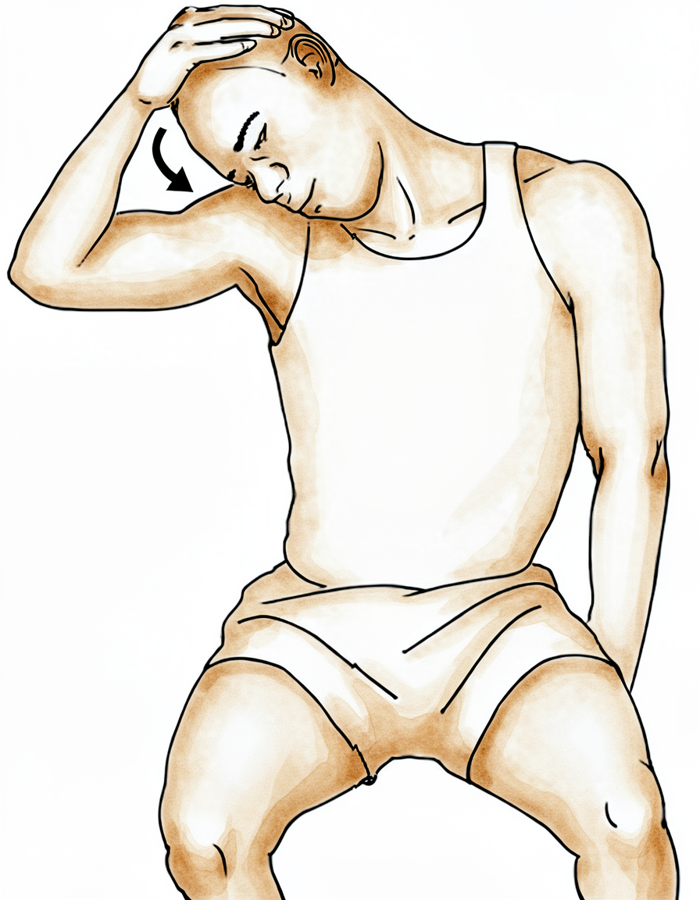
Levator scapulae stretch
Use your non-operated arm to bring your nose towards your armpit area, away from the operated side.
Hold 10 seconds, 3 times, 3 times per day
Kieran Hirpara 4.0
Rhythmic stabilisation
With your arm supported in front of you at about shoulder height, have your physiotherapist (or your good hand) apply small, gentle pushes from different directions while you hold the arm still and steady — do not let it move. This trains the shoulder's stabilising muscles to react. Keep all the efforts gentle.
As guided by your physiotherapist
Begin these gentle exercises in hospital and continue them at home. They should be comfortable; ease back if pain increases.
If you had a reverse replacement, you can start moving the shoulder early; begin with assisted and gravity-assisted movements (easiest lying on your back, letting gravity help), then add gentle active movement as your comfort allows, staying within what feels comfortable. Just keep clear of the positions to avoid listed under "Wearing your sling."
If you had a total (anatomic) replacement or a replacement for a fracture, keep your early movements assisted and gentle as shown; let your other arm do the work, and don't push the operated arm outwards past where the exercises ask, so the healing repair at the front of the shoulder is protected.
Wearing your sling
How long you wear the sling depends on which replacement you had; please follow the rule for your operation.
If you had a reverse replacement:
- The sling is mainly for comfort and support, and you'll wear it for about 2 weeks rather than full-time for 6 weeks.
- You can take your arm out of the sling for your exercises and for showering.
- You can start gentle shoulder movements straight away (see your exercises); there's no need to keep the arm completely still.
- There are a few positions to avoid in the early weeks while everything settles: don't reach your arm behind your body or behind your back, don't combine reaching backwards with turning the arm inwards, don't lift anything, and don't push up through your hands (for example, pushing yourself up out of a chair). Your physiotherapist will go through these with you.
If you had a total (anatomic) replacement, or a replacement for a fracture:
- You need to sleep in the sling.
- You are allowed to take your arm out of the sling for your exercises and for showering.
- You need to wear your sling for 6 weeks, especially when out of the house.
- A repair at the front of your shoulder needs time to heal, so your early movements are gentler and more guarded; keep to the assisted exercises shown and don't force the arm outwards past where the exercises ask.
For everyone:
- Use ice for pain relief if needed.
- When wearing your sling, relax your shoulder and let the sling take the weight of your arm.
- Take your painkillers before you do your exercises, and before your physiotherapy appointments.
- Unless you have arranged your own physiotherapy, an appointment has been made for you and is detailed in your discharge pack.
- If you have any problems, contact the rooms or let your physiotherapist know.
When you go home
Once you are home, your recovery continues with the full rehabilitation protocol for your operation: reverse shoulder replacement; total shoulder replacement; shoulder replacement for fracture.
The evidence behind this early in-hospital phase (why the sling and gentle movements matter, why a reverse replacement can move early and freely with the main caution being to keep the arm from reaching behind the body, and why a total replacement is more guarded with external rotation limited to protect the repair at the front of the shoulder) is summarised in the evidence section, available as a PDF from the top of this page.
Evidence & references
Topic scope: This page covers only the early in-hospital phase of recovery after a shoulder replacement — the first days on the ward and the principles of the first protected weeks — for anatomic total shoulder arthroplasty (TSA), reverse total shoulder arthroplasty (RSA), and shoulder replacement performed for a proximal-humerus fracture. The companion patient page (the synthesis) lists the actual in-hospital exercises and sling rules; this page sets out the evidence behind them. The full course of rehabilitation for each operation lives in its own protocol — follow that one once you are home: total shoulder replacement, reverse shoulder replacement, and shoulder replacement for fracture, each of which carries its own detailed evidence page.
Defining principle of the early phase: the two pathways now differ. A reverse replacement is run on an accelerated, permissive footing, while an anatomic total replacement (and a replacement for a fracture) remains protective. In every case the hand/wrist/elbow are kept active from the start, but what the shoulder itself is allowed to do — and what is being protected — differs by operation:
- Anatomic TSA protects the subscapularis repair. To put the ball-and-socket implant in, the surgeon detaches and re-attaches the subscapularis tendon (or its bone block) at the front of the shoulder. Early external rotation is limited, active and resisted internal rotation is delayed, and shoulder elevation is kept passive/assisted — because these are the positions that strain the healing repair. This is why the in-hospital ER exercise only moves the arm from the sling position to pointing straight ahead — and no further. The sling is worn full-time for about 6 weeks.
- Reverse TSA is accelerated. Often there is no subscapularis repair to protect, and the deltoid (not the cuff) powers the arm, so the shoulder can move early. The sling is for comfort and support only (~2 weeks), and active-assisted and active-as-tolerated shoulder motion begins from the start (supine/gravity-assisted first), within comfort. The main early constraint is dislocation precautions, whose at-risk position is hand-behind-the-back (combined extension + adduction + internal rotation): avoid reaching the arm behind the body or behind the back, no lifting, and no pushing up through the hands. This aligns with the accelerated reverse literature (see the reverse protocol's evidence page).
- Replacement for fracture adds a third constraint: the tuberosities (the bony muscle attachments) must heal, so this pathway follows the protective line (like anatomic TSA) and is usually the most protective of the three.
Common to all three: the hand/wrist/elbow are kept active immediately, and adequate analgesia makes early gentle motion possible. The sling duration and how freely the shoulder moves then differ — permissive for reverse, guarded for anatomic and fracture.
The early in-hospital phase, in brief
Most patients stay in hospital a short time after a shoulder replacement — commonly about one to two nights, and selected patients are now safely discharged the same day. Before discharge the ward physiotherapist fits the sling, teaches independent sling management, and starts the gentle exercises shown in the synthesis: keeping the hand, wrist and elbow active; pendulums; and shoulder elevation — assisted (passive) and limited in external rotation after an anatomic repair, but active-assisted and active-as-tolerated from the start after a reverse replacement. The arm is commonly numb from a nerve block when you wake, with sensation returning over roughly 24 hours. The job of this phase is pain control, swelling reduction, keeping the non-shoulder joints moving, and protecting the new joint while it settles — not building strength, which comes later in the home protocol.
Evidence by theme
1. Length of stay is short, and same-day discharge appears safe in selected patients
Shoulder replacement has traditionally been an inpatient operation, but length of stay is short and falling. At an orthopaedic specialty hospital the average stay was about 1.3 days versus ~1.85 days at a general centre [RAG corpus — 10.1016/j.jse.2016.01.010]. A large series found same-day discharge was not inferior to a longer in-hospital stay for 90-day readmissions [RAG corpus — 10.1016/j.jse.2019.09.037], and outpatient TSA in an ambulatory centre was reported as a safe alternative to inpatient care in a matched cohort (2016 Neer Award) [RAG corpus — 10.1016/j.jse.2016.07.011]. Same-day discharge appears safe even in patients aged ≥65 with appropriate selection [RAG corpus — 10.1016/j.jse.2021.02.022]. Whether you stay one night or go home the same day is an individual decision; the early-exercise and sling principles are the same either way.
Evidence: MODERATE (cohort / matched-cohort data).
2. Pain control is the patient's and the system's primary early concern
When patients consider shorter stays, perioperative pain control is their primary concern [RAG corpus — 10.1016/j.jse.2022.07.009] — which is why the synthesis emphasises taking analgesia before exercises and physiotherapy. Adequate pain relief is also what makes early gentle motion possible. A regional nerve block is commonly used, explaining the early numbness that recovers over about a day.
Evidence: MODERATE (survey / practice data).
3. Early motion depends on the operation — accelerated for reverse, guarded for anatomic
The ward starts active hand/wrist/elbow motion immediately after every replacement. What the shoulder is allowed to do then splits by operation. For reverse replacement the conservative-versus-early question has been tested directly: randomised trials show that earlier motion and shorter (or even no) immobilisation do not increase dislocation or complications, including a 3-week-versus-no-immobilisation RCT in primary RSA [RAG corpus — 10.1016/j.jse.2025.02.015], and home-based physiotherapy matched formal outpatient therapy after RSA [RAG corpus — 10.1016/j.jse.2023.03.023]. Dr Hirpara's reverse pathway now follows this accelerated line: a short (~2-week) comfort sling, and active-assisted and active-as-tolerated shoulder motion (supine/gravity-assisted first) from the start, within comfort — with dislocation precautions (no arm behind the body, no lifting, no pushing through the hands) the main early constraint. By contrast, anatomic TSA and replacement for fracture keep the protective early line — passive/assisted elevation only, no active shoulder lifting, and the front-of-shoulder repair (or the tuberosities) guarded — because there is a repair that the reverse construct does not have.
Evidence: MODERATE–STRONG for RSA early motion (RCTs), which the reverse pathway now reflects; the specific in-hospital timings are consensus/surgeon preference.
4. Why external rotation is limited after anatomic TSA but freer after reverse
In anatomic TSA the subscapularis must be detached to seat the implant and then repaired, and external rotation (especially with the arm out to the side) puts the greatest strain on that repair — so early ER is restricted while forward elevation and scaption, which do not load the repair, are allowed sooner [literature — Brigham & Women's Faulkner TSA guideline; subscapularis management review]. Typical published protocols cap early external rotation at around 20–30° and release it at about 6 weeks; the synthesis applies this by moving the arm only from the sling position to "pointing straight ahead." After reverse replacement there is usually no subscapularis repair to protect, so ER is more permissive and the dominant precaution is instead the hand-behind-the-back dislocation position [parent reverse protocol — RAG corpus 10.1016/j.jse.2016.12.073; 10.1016/j.jse.2020.05.019].
Evidence: MODERATE (biomechanical + protocol consensus); no single defining rehab RCT for the early in-hospital window.
Phased timeline — the early phase only
This focuses on the in-hospital and immediately-post-discharge window. The complete multi-phase course (intermediate, transitional, advanced strengthening, return to sport) lives in each parent protocol; the rows below are intentionally consistent with the Phase I content of those pages.
| Phase | Window | Sling | Shoulder motion | Operation-specific note |
|---|---|---|---|---|
| In hospital | Days 0–2 | Reverse: comfort/support. Anatomic + fracture: worn incl. overnight | Active hand/wrist/elbow (all); pendulums. Reverse: active-assisted + active-as-tolerated from the start (supine/gravity-assisted first). Anatomic + fracture: passive/assisted elevation, limited assisted ER | Ward physio fits sling, teaches management, starts the synthesis exercises before discharge |
| Early protection | Weeks 0–3 | Reverse: ~2 weeks for comfort. Anatomic + fracture: full-time (worn overnight) | Reverse: continue active-assisted/active motion within comfort; dislocation precautions (no arm behind body, no lifting, no pushing through hands). Anatomic TSA: passive/assisted only, no active lifting, ER limited (sling-to-straight-ahead), IR delayed. Fracture: most protective | Pain + swelling control; keep adjacent joints moving |
After this early window, follow the full protocol for your specific operation (linked above), where the sling is weaned, active motion is progressed, and strengthening begins.
Key controversies / evidence quality
- Inpatient vs same-day discharge. Cohort evidence supports same-day discharge in selected patients, but selection matters and pain control is the limiting factor; whether you stay overnight is a clinical judgement, not a fixed rule. Moderate.
- How protective to be early. Randomised data (strongest for reverse) show early motion and shorter immobilisation are safe. The reverse pathway now applies this accelerated approach (short comfort sling, early active-assisted/active motion, dislocation precautions). The anatomic pathway stays protective because it has a subscapularis repair to guard — there the protective early phase is a deliberate surgeon clinical decision, not an oversight relative to the accelerated literature. Moderate–strong evidence; applied per operation.
- The in-hospital protocol itself is consensus/expert. The specific early exercises and ROM limits are drawn from published institutional protocols and surgeon guidance, not from a rehab RCT of the in-hospital window. Weak/consensus.
Evidence-strength flags (summary)
- MODERATE (cohort): short length of stay; same-day discharge non-inferior for readmissions and safe in selected and older patients; pain control as the primary patient concern.
- MODERATE–STRONG (RCT, mainly reverse): early motion / shorter immobilisation safe after RSA; home-based PT equivalent to formal outpatient PT after RSA.
- MODERATE (biomechanical + protocol consensus): ER restriction protects the subscapularis repair in anatomic TSA; reverse rehab more permissive in ER but constrained by the dislocation position.
- WEAK / CONSENSUS: the specific in-hospital exercise set and early-phase timings (institutional protocols + surgeon preference; no defining rehab RCT of the inpatient window).
Citations
RAG corpus (180,000+ Orthopaedic articles) — real DOIs returned by search
- Length of stay after shoulder arthroplasty — the effect of an orthopedic specialty hospital. J Shoulder Elbow Surg. 2016. DOI: 10.1016/j.jse.2016.01.010
- Same-day discharge is not inferior to longer length of in-hospital stay for 90-day readmissions following shoulder arthroplasty. J Shoulder Elbow Surg. 2020. DOI: 10.1016/j.jse.2019.09.037
- Outpatient total shoulder arthroplasty in an ambulatory surgery center is a safe alternative to inpatient total shoulder arthroplasty in a hospital: a matched cohort study (2016 Neer Award). J Shoulder Elbow Surg. 2016. DOI: 10.1016/j.jse.2016.07.011
- Is outpatient shoulder arthroplasty safe in patients aged ≥65 years? A comparison of readmissions and complications in inpatient and outpatient settings. J Shoulder Elbow Surg. 2021. DOI: 10.1016/j.jse.2021.02.022
- Perioperative pain control represents the primary concern for patients considering outpatient shoulder arthroplasty: a survey-based study. J Shoulder Elbow Surg. 2022. DOI: 10.1016/j.jse.2022.07.009
- Three-week immobilization vs. no immobilization in primary reverse total shoulder arthroplasty: a randomized controlled trial. J Shoulder Elbow Surg. 2025. DOI: 10.1016/j.jse.2025.02.015
- Home-based physical therapy results in similar outcomes to formal outpatient physical therapy after reverse total shoulder arthroplasty: a randomized controlled trial. J Shoulder Elbow Surg. 2023. DOI: 10.1016/j.jse.2023.03.023
- The American Society of Shoulder and Elbow Therapists' consensus statement on rehabilitation for anatomic total shoulder arthroplasty. J Shoulder Elbow Surg. 2020. DOI: 10.1016/j.jse.2020.05.019
- Dislocation following reverse total shoulder arthroplasty. J Shoulder Elbow Surg. 2017. DOI: 10.1016/j.jse.2016.12.073
Literature (URLs)
- The effect of subscapularis-specific rehabilitation following total shoulder arthroplasty: a prospective, double-blinded, randomized controlled trial. J Hand Ther / ScienceDirect. 2023. https://pubmed.ncbi.nlm.nih.gov/37263480/
- Management of the subscapularis tendon during total shoulder arthroplasty (early ER strains the repair most). J Hand Ther / ScienceDirect. 2016. https://www.sciencedirect.com/science/article/abs/pii/S1058274616305791
Published rehabilitation protocols (basis for the early-phase structure)
- Brigham & Women's Faulkner Hospital — Department of Rehabilitation Services: Total Shoulder Arthroplasty Guideline (early ER restriction to protect the subscapularis repair). https://www.brighamandwomensfaulkner.org/assets/BWH/patients-and-families/rehabilitation-services/pdfs/total-shoulder-arthroplasty-guideline.pdf
- Massachusetts General Brigham Sports Medicine — Rehabilitation Protocol for Total Shoulder Arthroplasty and Hemiarthroplasty (Revised December 2018). https://www.massgeneral.org/assets/MGH/pdf/orthopaedics/sports-medicine/physical-therapy/rehabilitation-protocol-for-total-shoulder-arthroplasty-and-hemi.pdf
- Massachusetts General Brigham Sports Medicine — Rehabilitation Protocol for Reverse Shoulder Arthroplasty (Revised December 2018). https://www.massgeneral.org/assets/mgh/pdf/orthopaedics/sports-medicine/physical-therapy/rehabilitation-protocol-for-reverse-shoulder-arthroplasty.pdf





