Thumb Base Joint Replacement (Touch) Info Evidence
Reviewed by Dr Kieran Hirpara, Specialist Orthopaedic Surgeon Last reviewed
This protocol guides your recovery after a thumb base joint replacement (a dual-mobility total joint replacement, the Touch implant) for arthritis of the thumb base, with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It begins with your home exercise program, followed by the structured clinical protocol written for your hand therapist; bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your hand therapist may adjust the plan depending on how your recovery progresses. All of your recovery is guided through formal hand therapy.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect
The joint at the base of your thumb (the trapeziometacarpal, or CMC, joint) is where the thumb meets the wrist, and it is a very common site of arthritis. In this operation, the worn joint surfaces are removed and replaced with a small artificial joint: a dual-mobility implant, a tiny ball-and-socket with an extra moving surface that makes it stable and smooth. The trapezium bone is kept and the length of your thumb is preserved, so recovery is generally faster than a trapeziectomy (the older operation, which removes a bone and relies on scar tissue forming over many months).
A well-seated implant is stable and able to share load straight away, which is why the thumb only needs to be protected for a short time rather than immobilised for weeks. The plan is to settle the soft tissues, then quickly get your thumb opposing (touching the fingers) and moving again, and then build strength.
The recovery runs in three stages:
- First, protect (about the first 2–3 weeks). A soft bulky dressing for the first week or so, then a thumb splint to rest the new joint while the wound and soft tissues settle. You keep your fingers, wrist and the rest of the hand moving.
- Then, move (from about 2–3 to 6 weeks). Out of the day splint, you begin gentle active movement (opposition, lifting the thumb, opening the web space and circling) and use the hand for light everyday tasks.
- Then, strengthen (from 6 weeks onwards). Once the implant has bonded to the bone, pinch and grip strengthening begins and is built up gradually. Strength keeps improving over the following 6 to 12 months.
The one thing to respect early on is that the new joint can dislocate if it is forced into an extreme position before the tissues around it have healed. This is uncommon, and the early plan is simply built around not forcing the thumb while it settles.
Precautions and limitations
- Wear your thumb splint as directed (a day splint for the first 2–3 weeks, then a night splint through to 6 weeks) and keep the splint on for protection until your hand therapist advances you.
- Do NOT force the thumb into extreme positions, and avoid sudden or awkward grabs in the early weeks; the new joint can dislocate if pushed too far before it settles. Move within comfort only.
- Do NOT do any strong pinching, gripping, twisting (jar lids, keys, taps) or lifting until about 6 weeks; strengthening starts only when your hand therapist begins it.
- Keep your fingers, wrist and the rest of the hand moving from the start, and keep your hand elevated early on to settle swelling.
- Do NOT drive until about four to six weeks, once you are out of your splint and can grip the wheel comfortably and painlessly.
For wound, swelling and scar management, see the practice's wound care guidance.
Your exercises
Kieran Hirpara 4.0
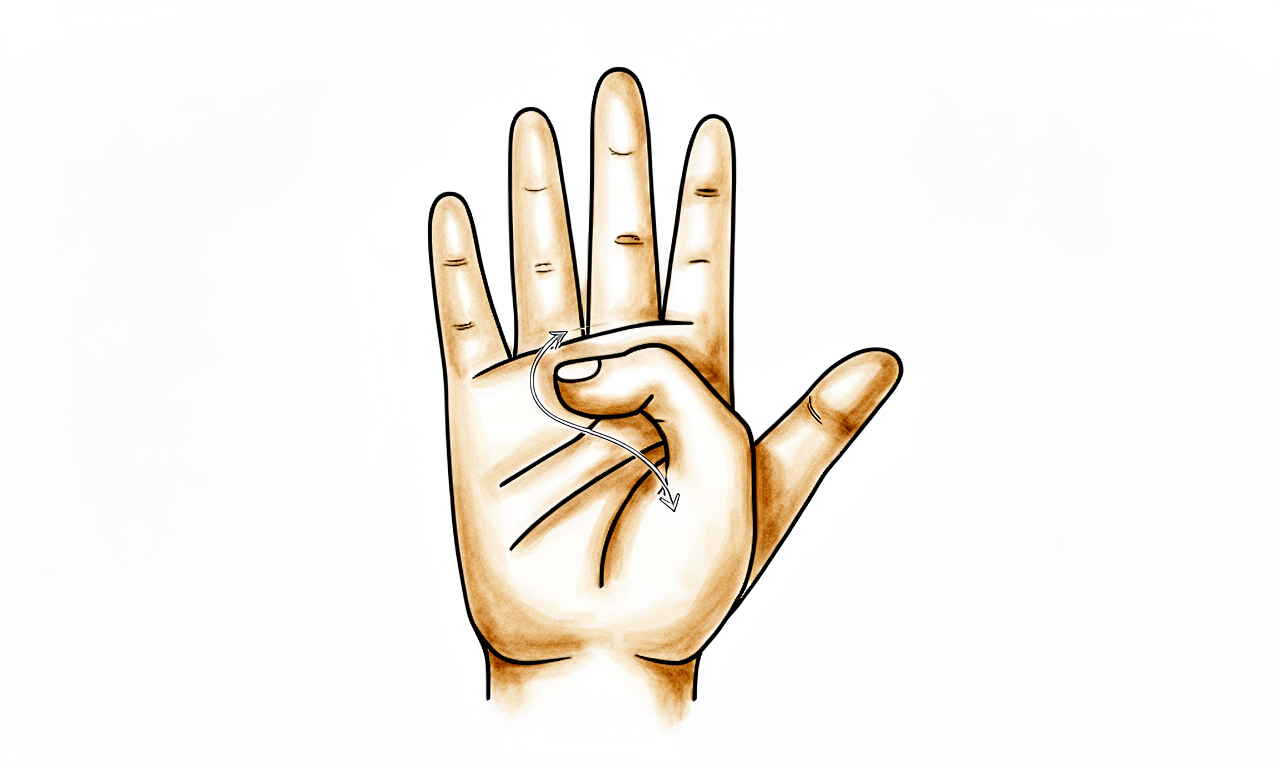
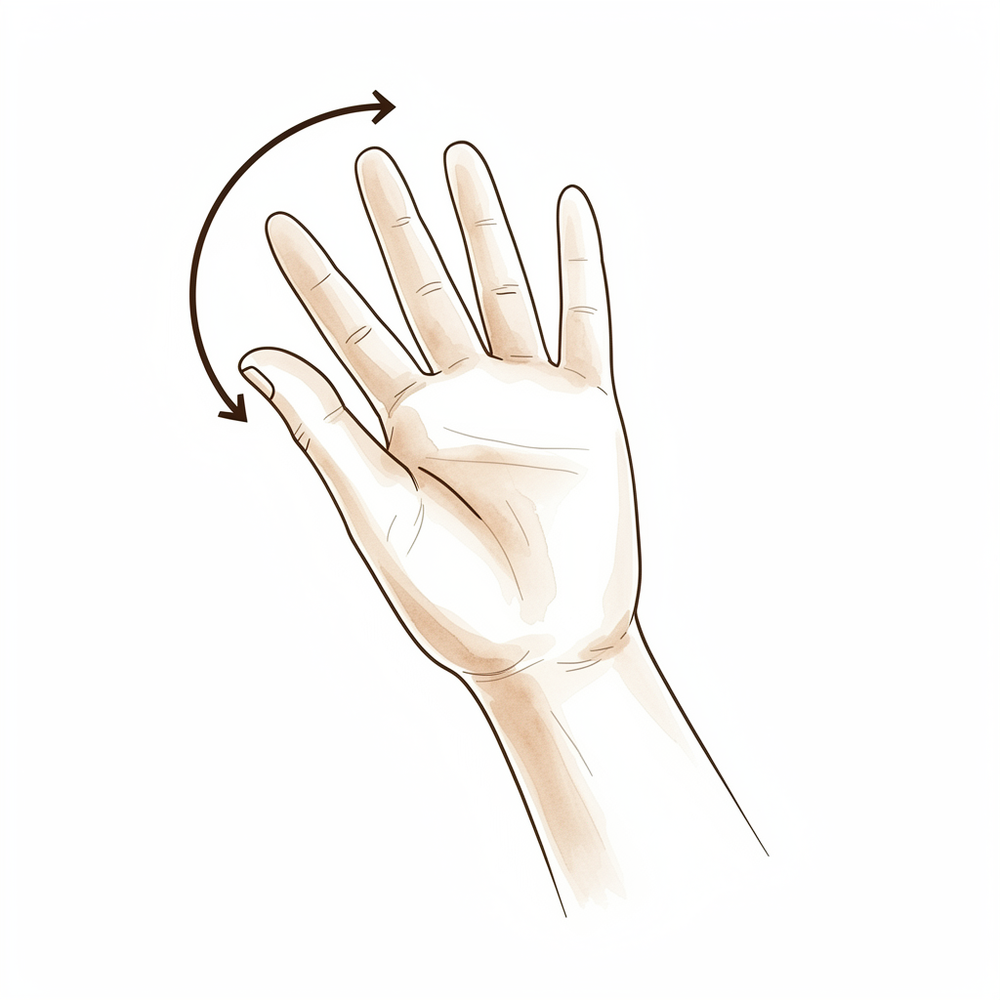
Thumb opposition (Kapandji ladder)
Slowly touch the tip of your thumb to the side of your index finger, then to the tip of each finger in turn, and then walk it down the little finger towards its base — climbing the 'ladder' a little further as you loosen up. Move only as far as is comfortable. This is the key movement to recover after a thumb base replacement, and it is started gently once you are out of your day splint (around two to three weeks).
Work through the ladder 5–10 times, 2–3 times a day, within comfort
Kieran Hirpara 4.0
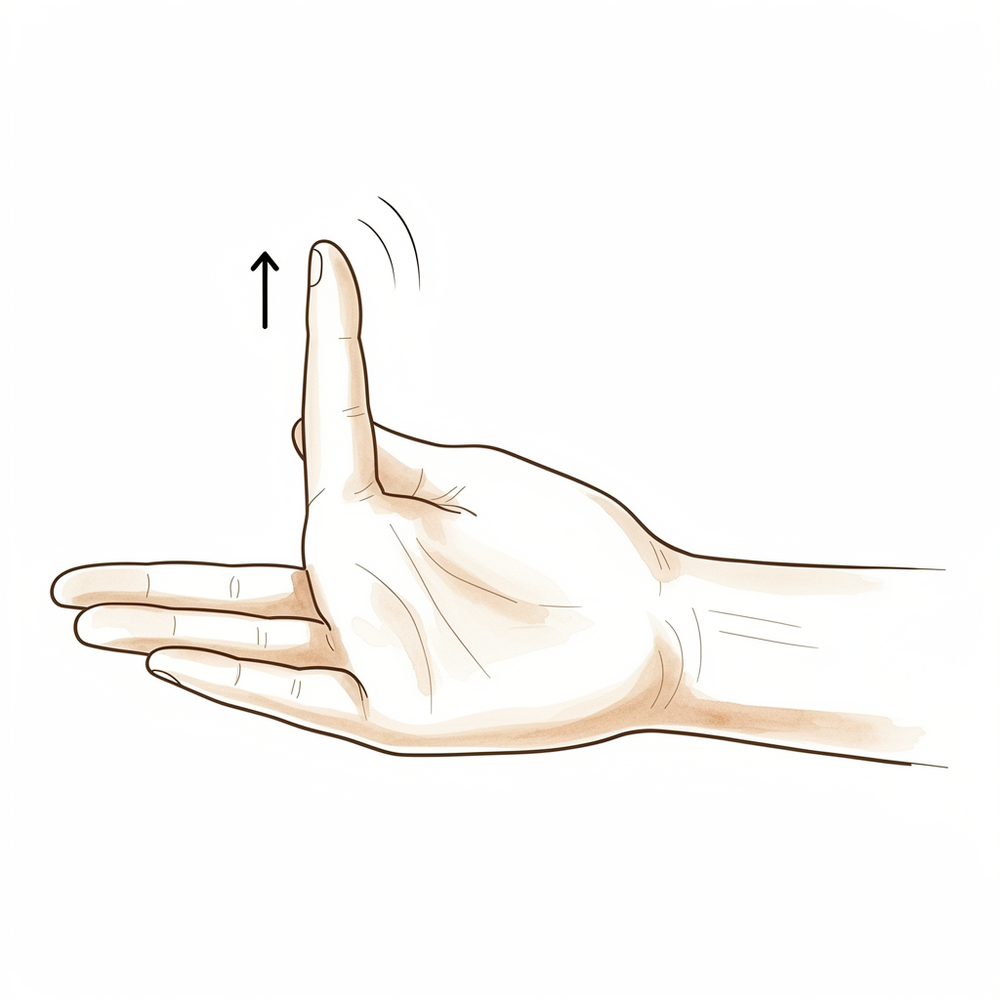
Palmar abduction (lift thumb off palm)
Rest your hand flat, palm up. Keeping your thumb straight, lift it up away from your palm towards the ceiling, as if opening your hand to hold a can — then lower it back down. This opens the web space and restores the thumb's reach. Keep it gentle and unforced; do not push into the end of the movement in the early weeks.
10 times, 2–3 times a day, within comfort
Kieran Hirpara 4.0
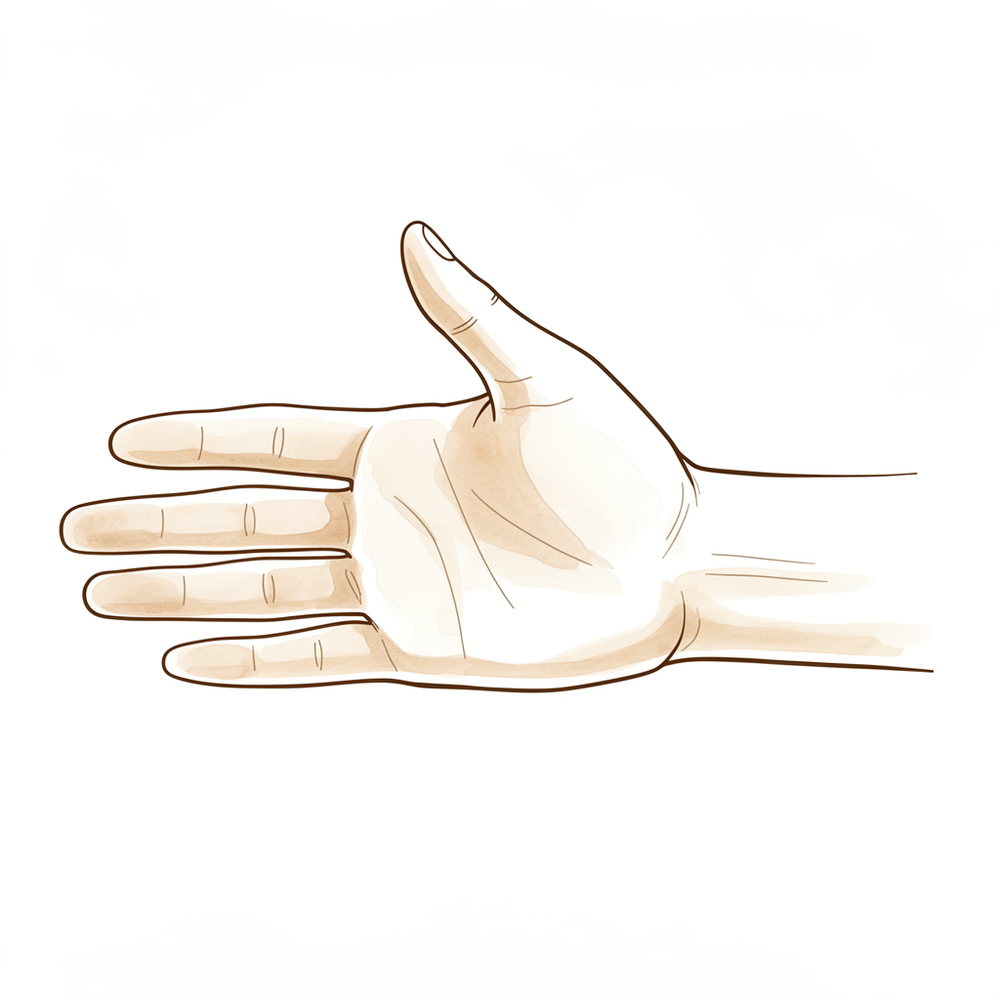
Radial abduction (thumb out to the side)
Rest your hand flat with the palm down. Slide your thumb out sideways, away from your index finger, keeping it in the same flat plane as your palm — like making an 'L' shape — then bring it back. This restores the sideways reach of the thumb. Move slowly and stop short of any strain.
10 times, 2–3 times a day, within comfort
Kieran Hirpara 4.0
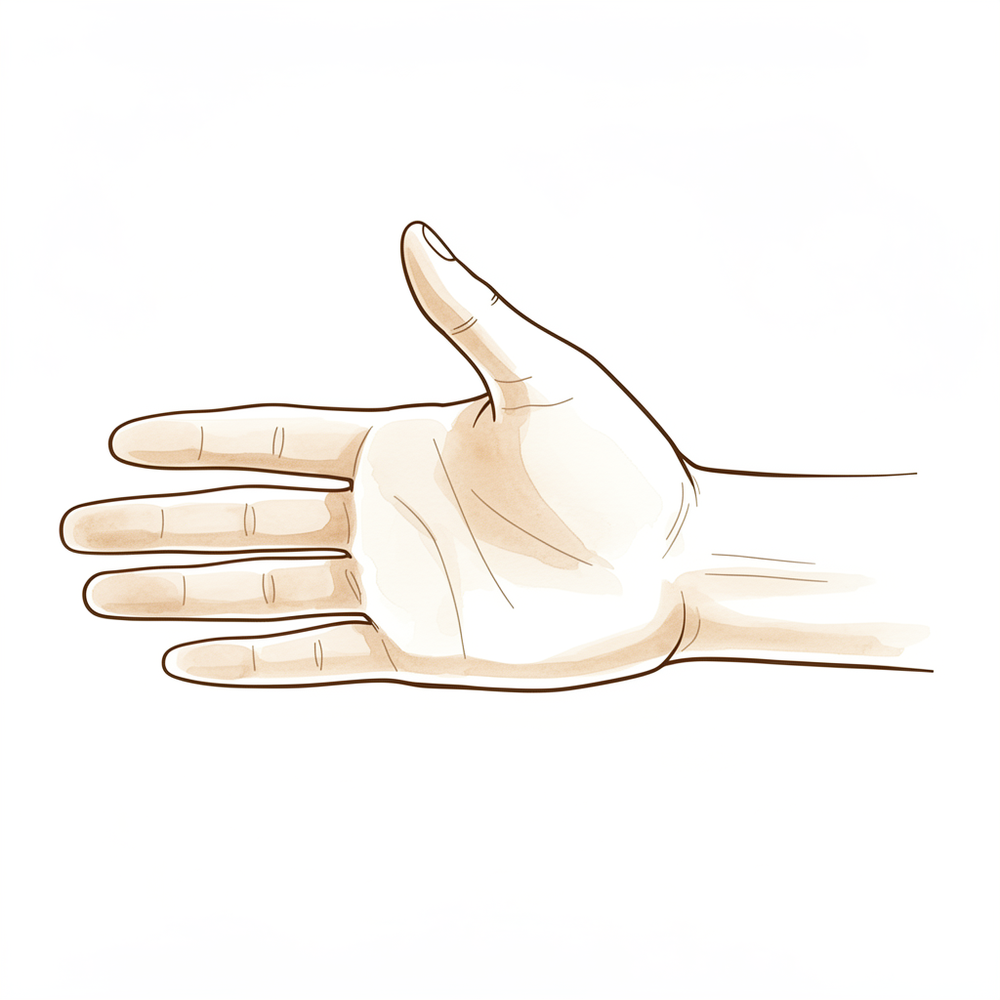
Web-space stretch
Open the space between your thumb and index finger as wide as is comfortable, feeling a gentle stretch across the web. You can rest your hand on a table and let the thumb ease open, or cup it around a rounded object. Hold the open position briefly, then relax. This keeps the web space from tightening as you heal — keep it gentle, never forced.
Hold ~5 seconds, 5–10 times, 2–3 times a day
Kieran Hirpara 4.0
Thumb circumduction
With your hand relaxed, draw slow, smooth circles with your thumb, taking it gently around its full range in both directions — as if stirring a small pot. Keep the circles easy and within comfort. This restores the combined, rolling movement of the new joint and is started gently once you are out of the day splint.
5–10 circles each direction, 2–3 times a day
Kieran Hirpara 4.0
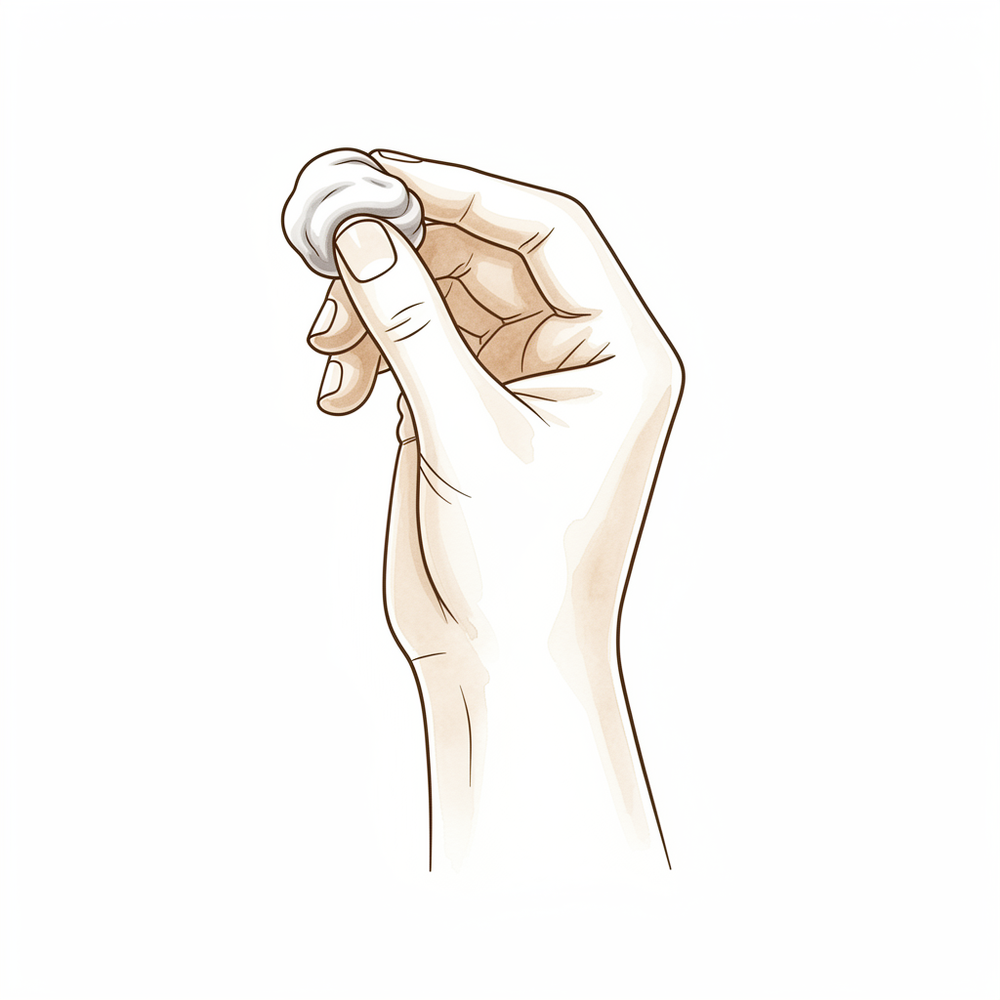
Putty / key pinch (from week 6)
A LATER exercise — only from around six weeks, once your hand therapist starts strengthening. Pinch a piece of therapy putty between your thumb and the side of your index finger (a 'key' pinch), and press your thumb tip to your fingertips (a 'tip' pinch), building the effort up gradually over the following weeks and months. Do NOT do strong pinching or gripping before six weeks — the new joint needs that time to settle and bond to the bone.
As guided by your hand therapist (from ~6 weeks), building gradually
These are the exercises from your handout. Start them only as guided by Dr Hirpara and your hand therapist, staying within whatever range and limits you have been given. The early exercises (opposition, lifting the thumb, the sideways movement, the web-space stretch and gentle circles) restore the thumb's movement without loading the new joint, and begin once you are out of your day splint. The putty and key pinch is a later strengthening exercise and should not be started until about six weeks, when your hand therapist begins it. Keep every movement gentle and unforced in the early weeks, and stop anything that causes sharp pain at the base of the thumb.
Your clinical protocol
The rest of this page is the staged clinical protocol for rehabilitation after a dual-mobility trapeziometacarpal (Touch) total joint replacement. This section is to be provided to your hand therapist, and each phase opens with a plain-English explanation of what is happening. Unlike a trapeziectomy, the implant is immediately stable and load-sharing, so immobilisation is minimal and active opposition is restored early; the implant-specific early risk is dislocation if forced into extreme range, so the first weeks protect against forced/end-range positions while restoring motion, then progress to loaded strengthening once osseointegrated.
Prior to treatment, check the patient's operation report and past medical history, and liaise with the treating surgeon regarding implant seating/stability and any intra-operative concerns. Dr Hirpara's regimen is a soft bulky dressing for 7–10 days, then a thumb spica DAY splint for 2–3 weeks, followed by a NIGHT splint continuing to 6 weeks (wrist neutral, thumb in mid palmar abduction, IP free). The trapezium is retained and thumb length preserved.
Phase I — protect (week 0 to ~2–3)
The first few weeks settle the soft tissues and protect the new joint. The thumb rests in a soft bulky dressing, then a thumb spica day splint, while the fingers, wrist and rest of the hand keep moving. No resisted thumb work, and no forced or extreme thumb positions (early dislocation is the implant-specific risk).
For your hand therapist:
Education and precautions - Immobilise the thumb base: soft bulky dressing 7–10 days → thumb spica DAY splint for weeks ~2–3 (wrist neutral, thumb in mid palmar abduction, IP joint free) - Avoid forced/extreme thumb positions and sudden grasps: dislocation is the early implant-specific risk - No resisted thumb work (no pinch, grip, twisting or lifting) - Keep the implant unloaded; light unloaded hand use only
Management - Wound: surgical dressings as directed; monitor for infection - Oedema: elevation, gentle hand pump, ice as needed - Exercises: active ROM of the IP joint of the thumb, the fingers, and the wrist; maintain full-hand mobility; no active CMC/opposition work yet, no loading
Criteria to progress - Wound settling; comfortable; out of the day splint at around 2–3 weeks for active motion
Phase II — active motion in a night splint (week ~2–3 to 6)
From about two to three weeks the day splint comes off and gentle active thumb movement begins: opposition (a Kapandji progression), palmar and radial abduction, gentle circumduction and web-space mobilisation. A night splint continues to six weeks. Light everyday use is encouraged; heavy grip and pinch are still withheld.
For your hand therapist:
Assessments - Active thumb opposition (Kapandji score), palmar/radial abduction, web-space width; pain and swelling; wound/scar review
Education and precautions - Out of the day splint; continue the NIGHT splint to 6 weeks - Active unresisted thumb motion only: no heavy grip or pinch before 6 weeks - Keep movement within comfort; avoid forcing end-range
Management - Exercises: active unresisted opposition (Kapandji progression), palmar and radial abduction, gentle circumduction, web-space mobilisation; light everyday functional use of the hand; commence scar massage once the wound is healed
Criteria to progress - Good active opposition restored; wound healed; pain-free unresisted motion at around 6 weeks
Phase III — load and strengthen (week 6 onwards)
From about six weeks the implant is osseointegrated and can be loaded. Pinch and grip strengthening begins (putty pinch, key and tip pinch, opposition strengthening) and is progressed gradually. Strength continues to mature over the following 6 to 12 months.
For your hand therapist:
Assessments - Key/tip pinch and grip strength versus the other side; opposition; pain/swelling response to loading; functional and work-specific testing as appropriate
Education and precautions - Begin progressive pinch and grip strengthening from 6 weeks; build load gradually - Expect strength to mature over 6–12 months; counsel patience with heavier loading
Management - Exercises: putty pinch, key/tip pinch, opposition strengthening, progressive resistance; grip strengthening; continue any residual mobility and scar work - Consider discharge once strength is functional and a suitable return of function is achieved - Consider referral back to the treating doctor if recovery plateaus or there is a poor outcome
Criteria for discharge - Functional, near-symmetrical pinch and grip; pain-free everyday and work-specific use
Getting back to work and activity
Light everyday hand use (eating, writing, light self-care) is encouraged within comfort from early on, as long as it does not involve forcing the thumb or strong pinching and gripping. Because you must not drive until you are out of your splint and can grip the wheel comfortably, plan for help with transport in the early weeks. Driving usually resumes at around four to six weeks, once you can grip the wheel painlessly, as confirmed by Dr Hirpara.
Office and light work is usually possible within two to four weeks; manual and heavier work waits until about six weeks and then builds up gradually, because strong pinch and grip loading only begins at six weeks. Strength keeps improving for 6 to 12 months, so heavier and more demanding tasks are returned to progressively rather than all at once, judged by how your thumb is responding, with Dr Hirpara and your hand therapist rather than the calendar alone.
After your protocol
This protocol works alongside the practice's general recovery advice; see managing post-operative pain, wound care and scar management. The phased plan above reflects published rehabilitation guidance after dual-mobility thumb base joint replacement, and your ongoing recovery is guided individually by Dr Hirpara and your hand therapist according to how your thumb progresses.
Evidence & references
Topic scope: post-operative rehabilitation after a dual-mobility total joint replacement of the trapeziometacarpal (thumb base / CMC) joint for advanced thumb base osteoarthritis — the Touch implant. Unlike trapeziectomy, the trapezium is retained and thumb length preserved, and a correctly seated dual-mobility implant is immediately stable and load-sharing. The rehab is therefore a minimal-immobilisation, early-motion pathway: protect briefly against the implant-specific early dislocation risk, restore opposition within the first month, then load.
Defining principle of the rehab here: a trapeziectomy relies on a scar/haematoma "spacer" forming where the bone was removed, which takes roughly 12 months to mature — so rehab is slow by necessity. A dual-mobility thumb base replacement instead provides an immediately stable, load-sharing artificial joint, so immobilisation can be minimal, opposition is restored within the first month, and recovery is faster than trapeziectomy. The dual-mobility cup specifically reduces the early dislocation risk that drove longer immobilisation with older single-mobility implants. The one deliberate early restraint is therefore avoidance of forced/extreme thumb positions (the implant-specific dislocation risk) for the first few weeks, after which loaded pinch/grip strengthening begins. This is a newer implant: the evidence base is short-to-mid-term and low-to-moderate level, and rehab regimens are under-reported and not standardised.
A. PROCEDURE OUTCOMES (dual-mobility Touch TMC arthroplasty)
Dual-mobility total joint replacement of the thumb base is a comparatively new alternative to trapeziectomy for advanced trapeziometacarpal osteoarthritis. Early- to mid-term series report high implant survival and good restoration of pinch and function, with the principal trade-off being a higher complication/revision profile than the well-established trapeziectomy — though the dual-mobility design improves on the dislocation rate of earlier single-mobility implants.
- High short-to-mid-term implant survival and good function. A Touch-specific series reported 96% implant survival at 2 years with high key-pinch strength; the main adverse events were soft-tissue complications (de Quervain-type tenosynovitis, trigger digit) rather than implant failure [Herren 2023]. A 150-patient dual-mobility cohort similarly reports early normalisation of function. Moderate (case series / retrospective cohort).
- Faster recovery than trapeziectomy because the joint is immediately stable. Because the implant is load-sharing from the outset, the thumb is only briefly immobilised, patients return to near-normal activity early, and formal therapy may not always be required — contrasting with the ~12-month maturation of a trapeziectomy spacer [Duerinckx & Verstreken 2022]. Moderate (narrative review / cohort).
- Opposition and pinch/grip recover well. Using the MOOVIS dual-mobility implant, the Kapandji opposition score improved from 7 to 10 with improved pinch and grip [Dreant 2018]. Moderate (cohort).
- The dual-mobility design reduces dislocation. The extra articulation lowers the early dislocation risk that limited older single-mobility prostheses, supporting earlier mobilisation [Tchurukdichian 2019; Martins 2020]. Moderate (cohort / mechanistic).
- Lower reoperation than ball-and-socket designs; persistent revision risk overall. A network meta-analysis found dual-mobility implants had lower reoperation than ball-and-socket designs, with TOUCH reoperation around 1.0% [Burnett 2026 NMA]. Reported outcomes continue to evolve in ongoing reviews [Tosti & Duerinckx 2026]. Moderate (NMA of mostly observational data).
- Registry-level work-absence benchmark. Swedish registry data give a sense of real-world recovery: sick leave of roughly 94 days for men and 109 days for women — a benchmark to set realistic return-to-work expectations rather than a target. Moderate (registry).
B. REHABILITATION / THERAPY EVIDENCE
The central rehab questions are (1) how long to immobilise, and (2) when to start motion and loading. Because the implant is immediately stable, the modern answer is minimal immobilisation with early active opposition — but the literature is explicit that there is no consensus and wide variation between centres, and that rehab protocols are under-reported.
- Minimal immobilisation is justified by immediate stability. A correctly seated dual-mobility implant is stable and load-sharing, so prolonged casting is unnecessary; the thumb is briefly protected, then mobilised early, with opposition typically back within the first month [Duerinckx & Verstreken 2022]. Moderate (review).
- No standardised regimen — wide variation in immobilisation and motion timing. A dedicated review of immobilisation and rehabilitation after thumb-base arthroplasty found reported immobilisation ranging from 2 to 12 weeks and active range-of-motion commencing anywhere from 1 to 6 weeks, with no consensus across studies [Barrett 2022]. This is the key caveat for any protocol: the timings are a defensible, surgeon-confirmed plan, not a trial-derived standard. Moderate (systematic review of heterogeneous protocols).
- Early opposition recovery is achievable and is the functional priority. Improvement of the Kapandji opposition score (7→10) demonstrates that active opposition is the early rehab target and is realistically attainable in the first weeks-to-months [Dreant 2018]. Moderate (cohort).
- The early restraint is dislocation avoidance, not protected healing. The dual-mobility design reduces but does not abolish early dislocation; the practical implication is to avoid forced/extreme thumb positions in the first weeks rather than to immobilise for prolonged periods [Tchurukdichian 2019; Martins 2020]. Moderate / mechanistic.
Recovery trajectory (expected, evidence-anchored)
| Phase | Window | Restraint | Hand use / therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Protect | Week 0 to ~2–3 | Soft bulky dressing 7–10 d → thumb spica DAY splint | Keep IP/MCP/digits/wrist moving; oedema control; avoid forced/extreme thumb positions | No resisted thumb work | Early dislocation is the implant-specific risk; minimal immobilisation because the implant is immediately stable |
| II — Active motion | Week ~2–3 to 6 | NIGHT splint to 6 wk | Out of day splint; active unresisted opposition (Kapandji), palmar + radial abduction, gentle circumduction, web-space work; light everyday use; scar massage once healed | Still no heavy grip/pinch | Opposition typically restored within the first month; faster than trapeziectomy |
| III — Load / strengthen | Week 6+ | Restrictions lifted | Progress pinch/grip-specific loading and task use | Pinch + grip strengthening from 6 wk (putty, key/tip pinch); full weight-bearing ~6 wk | Strength matures over 6–12 months; return to heavy/manual work staged across this window |
(Phase windows reflect KH-confirmed parameters and are consistent with the wide ranges reported in the literature; they are typical guides, not trial-derived deadlines — see Barrett 2022.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY
- Replacement vs trapeziectomy. Dual-mobility replacement restores the joint and gives a faster functional return (immediate stability, opposition back within a month) versus the ~12-month maturation of a trapeziectomy spacer, but at the cost of a higher complication and revision rate and a shorter evidence track record. Trapeziectomy remains the well-established, lower-risk benchmark. Moderate; trade-off, not a clear winner.
- How long to immobilise / when to start motion. No consensus — reported immobilisation spans 2–12 weeks and AROM start 1–6 weeks [Barrett 2022]. This page's day-splint-2–3-weeks → night-splint-to-6-weeks → strengthen-from-6-weeks plan is a defensible, surgeon-confirmed regimen within that reported range, not a proven standard. Weak–moderate.
- Dislocation risk. The dual-mobility cup reduces the early dislocation that limited older single-mobility implants, but the risk is not zero in the first weeks — hence the early forced/extreme-position restraint [Tchurukdichian 2019; Martins 2020]. Moderate / mechanistic.
- Complication profile. Soft-tissue complications (de Quervain-type tenosynovitis, trigger digit) are the commonest early issues rather than implant failure [Herren 2023]; reoperation is low for dual-mobility (TOUCH ~1.0%) and lower than ball-and-socket designs [Burnett 2026 NMA]. Moderate.
- Maturity of the evidence. This is a newer implant: outcomes are short-to-mid-term, evidence is low-to-moderate level (case series, retrospective cohorts, registry and NMA of mostly observational data), and rehabilitation is under-reported and not standardised. Tone should be appropriately cautious. Evidence base still maturing.
D. EVIDENCE STRENGTH FLAGS (summary)
- MODERATE (cohort / registry / NMA of observational data): high short-to-mid-term implant survival (96% at 2 yr, Touch) with good key-pinch; Kapandji opposition 7→10; dual-mobility lower reoperation than ball-and-socket (TOUCH ~1.0%); registry sick-leave benchmark (~94 d men / 109 d women); faster functional return than trapeziectomy.
- MODERATE (systematic review of heterogeneous protocols): no consensus on rehab — immobilisation 2–12 weeks, AROM start 1–6 weeks (Barrett 2022).
- WEAK / CONSENSUS: the specific immobilisation-then-early-opposition-then-strengthen phase timings (surgeon-confirmed, within the reported range; not trial-derived); the dislocation-avoidance rationale (mechanistic).
- CAVEAT: newer implant — short-to-mid-term, low-to-moderate-level evidence; higher complication/revision rates than trapeziectomy persist; rehab under-reported.
CITATIONS
RAG corpus (180,000+ Orthopaedic articles)
- Duerinckx J, Verstreken F. Dual mobility prosthesis for trapeziometacarpal joint arthritis. EFORT Open Rev. 2022. DOI: 10.1530/eor-22-0027
- Herren DB, et al. Trapeziometacarpal joint replacement with the Touch prosthesis: two-year results. J Hand Surg (Eur Vol). 2023. DOI: 10.1177/17531934231179581
- Dreant N, et al. Trapeziometacarpal arthroplasty with the dual-mobility MOOVIS prosthesis. Hand (NY). 2018. DOI: 10.1177/1558944718797341
- Tchurukdichian A, et al. Dual-mobility implant reduces the dislocation risk in trapeziometacarpal arthroplasty. Hand (NY). 2019. DOI: 10.1177/1558944719855690
- Martins A, et al. Dual-mobility trapeziometacarpal prosthesis. J Hand Surg (Eur Vol). 2020. DOI: 10.1177/1753193420901435
- Barrett H, et al. Immobilization and rehabilitation after trapeziometacarpal joint arthroplasty: a review. J Hand Surg Glob Online. 2022. DOI: 10.1016/j.jhsg.2022.05.011
- Tosti R, Duerinckx J. Trapeziometacarpal total joint arthroplasty: current concepts. J Hand Surg Am. 2026. DOI: 10.1016/j.jhsa.2026.01.003
- Burnett K, et al. Implant designs for trapeziometacarpal arthroplasty: a network meta-analysis of reoperation. J Hand Surg Am. 2026. DOI: 10.1016/j.jhsa.2025.12.011
Thumb base arthroplasty literature (URLs)
- Herren DB, et al. TOUCH trapeziometacarpal prosthesis — two-year results. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC12098211/
- Dual-mobility trapeziometacarpal arthroplasty — 150-patient cohort. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC12662895/
- TOUCH prosthesis case series. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC8470025/
- KeriMedical — TOUCH thumb base prosthesis patient information. https://www.kerimedical.com/en/patients/





