Ulnar-Sided Wrist Pain and Ulnar Impaction Info
Last reviewed
Patients › Wrist
Pain on the little-finger side of the wrist from the ulna grinding against the wrist bones, and how shortening it relieves the pressure.
What you're feeling
Pain on the little-finger side of the wrist (the ulnar side) is very common, and it has several possible causes. This page is about the most important mechanical one: a condition called ulnar impaction (also known as ulnocarpal abutment).
The pain tends to sit deep on the outer edge of the wrist, towards the back of the hand. It is often worse when you grip firmly, twist your forearm, or bend the wrist towards the little finger, so everyday actions like opening a jar, turning a key, using a screwdriver, wringing out a cloth, or leaning on the hand to push up out of a chair can all set it off. Many people also notice a click or a clunk in the wrist with certain movements, and the wrist can ache after a day of heavy use. Putting weight through the wrist (in a plank, a push-up, or pushing a heavy door) is a classic aggravator.
It usually builds up gradually rather than starting with a single injury, though it can follow a wrist fracture.
What's actually happening
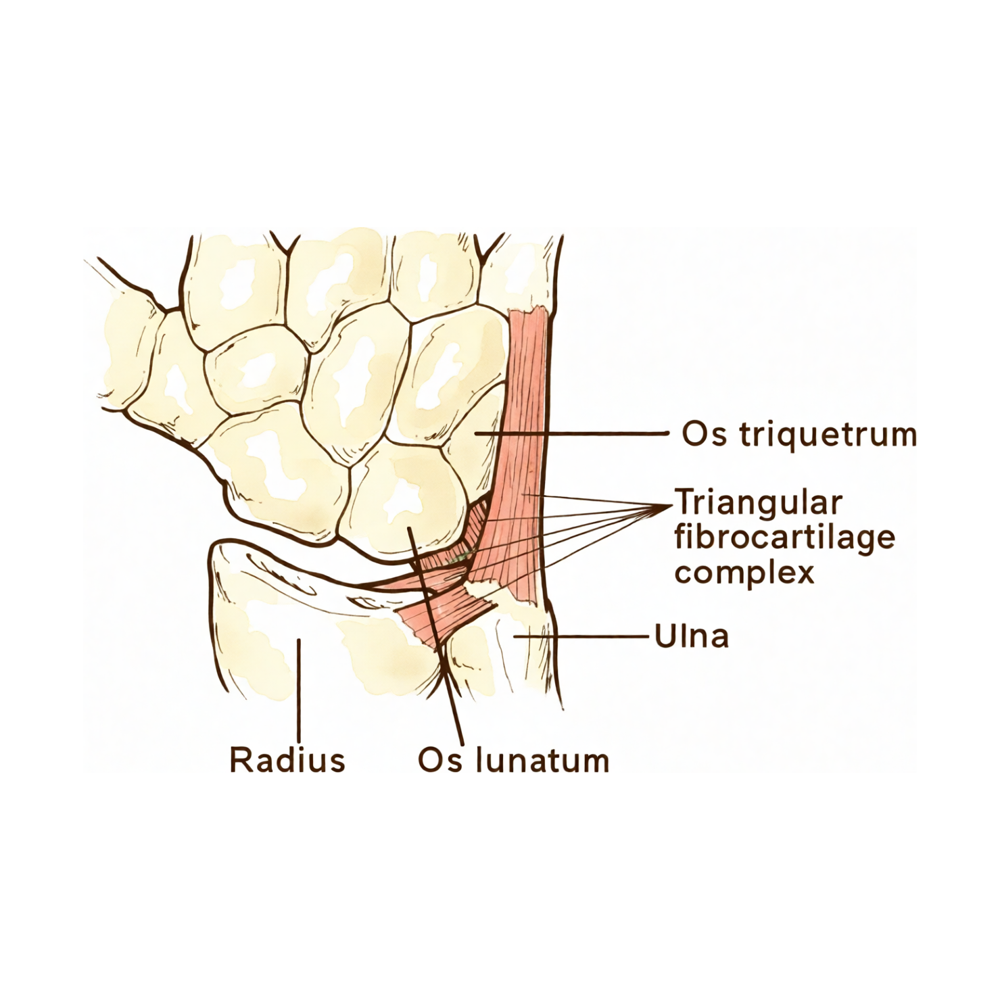
Two forearm bones run up to the wrist: the radius (thumb side) and the ulna (little-finger side). For the wrist to work smoothly, the ends of these two bones should sit at roughly the same level. In ulnar impaction, the ulna is relatively too long compared with the radius, a condition doctors call positive ulnar variance.
Some people are simply born with a slightly long ulna. In others it develops later: most often when a broken wrist heals slightly shortened, leaving the radius a touch shorter than it was and the ulna effectively standing proud.
Whatever the cause, that little bit of extra length means the end of the ulna grinds against the small wrist bones it sits next to (the lunate and the triquetrum) every time you load the wrist. In between those bones sits a cushion of cartilage called the TFCC (the triangular fibrocartilage complex), which acts as a shock-absorber. Repeated abutment slowly wears this cushion down, can tear the TFCC, and over time bruises and even forms small cysts in the bone underneath. That wear-and-tear process is what produces the pain, the clicking, and the loss of comfort with gripping and twisting. (We have a separate page on TFCC injuries, which often go hand-in-hand with this condition.)
What we can do about it
The good news is that most people settle with non-operative treatment, and that is always where we start.
Calming it down. The first steps are simple: modify the activities that load the ulnar wrist (especially heavy gripping, twisting and weight-bearing) for a while, wear a wrist splint to rest the joint, and use anti-inflammatory medication to settle the pain and swelling. Sometimes a steroid injection into the joint helps break the cycle of inflammation.
Confirming the diagnosis. Alongside treatment we usually take X-rays to measure exactly how the two bones line up (sometimes with a special "grip" view that exaggerates the impaction), and often an MRI to look at the cartilage, the TFCC and the bone underneath. Occasionally a keyhole look inside the joint (arthroscopy) is used to confirm what is going on and treat it at the same time.
If it persists. When good non-operative treatment hasn't settled things, the aim of surgery is to take the pressure off the ulnar side of the wrist. The most established option is an ulnar-shortening osteotomy, where the surgeon removes a small slice of the ulna to bring it back to the right length and holds it with a small plate while it heals. A less invasive alternative in selected cases is an arthroscopic "wafer" procedure, which shaves a small amount off the very end of the ulna through keyhole surgery. Both work by stopping the bone from grinding against the wrist.
What to expect
For most people, ulnar impaction is a problem we can get on top of. Non-operative measures settle a large proportion of cases, and the symptoms ease once the joint is no longer being repeatedly overloaded.
When surgery is needed, shortening the ulna is a reliable operation, and studies that have followed patients for many years report good, lasting pain relief and high satisfaction. The bone needs time to heal, so there is a recovery period of some weeks in a splint or cast while the osteotomy unites, followed by a gradual return to gripping and loading. The main things to be aware of are that the bone occasionally takes longer than expected to knit, and that the small plate can sometimes be felt under the skin and is occasionally removed once everything has healed. Overall, the great majority of people return to their everyday activities with the pain resolved.
When to see someone
- Ulnar-sided wrist pain that won't settle over a few weeks, or that keeps coming back with gripping and twisting, and is worth having assessed.
- Pain that follows a previous wrist fracture, especially if the wrist has never felt quite right since.
- A persistent click, clunk or catching on the little-finger side of the wrist, particularly with weight-bearing.
- Pain that is stopping you doing your job or your daily activities. This is the point at which it is worth looking into what is driving it and what can be done.





