Inpatient exercises — capsular release & subacromial decompression Info Evidence
Reviewed by Dr Kieran Hirpara, Specialist Orthopaedic Surgeon Last reviewed
These are the gentle exercises to begin in hospital after a capsular release or a subacromial decompression. For these operations the priority is to keep the shoulder moving freely.
Your exercises
Kieran Hirpara 4.0
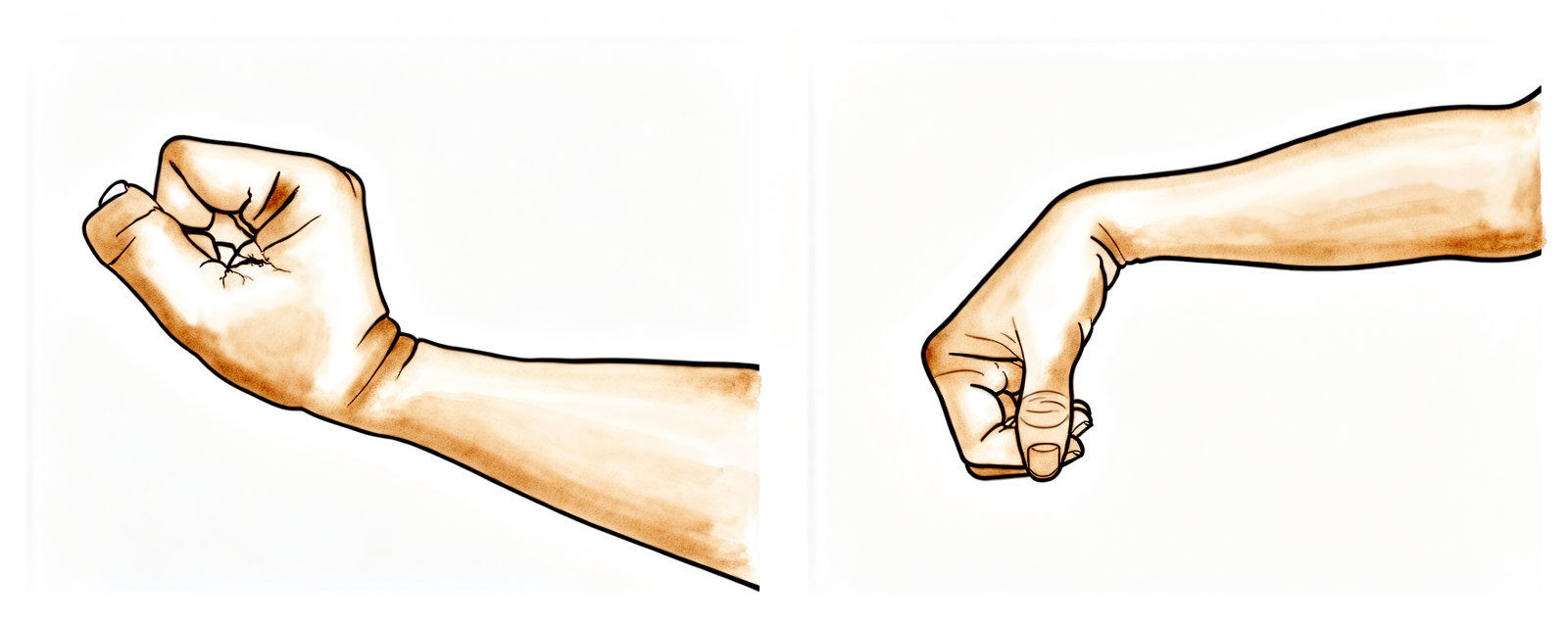
Wrist movement
Keep your hand moving by bending your wrist forwards, backwards and side to side.
10 times, 3 times per day
Kieran Hirpara 4.0
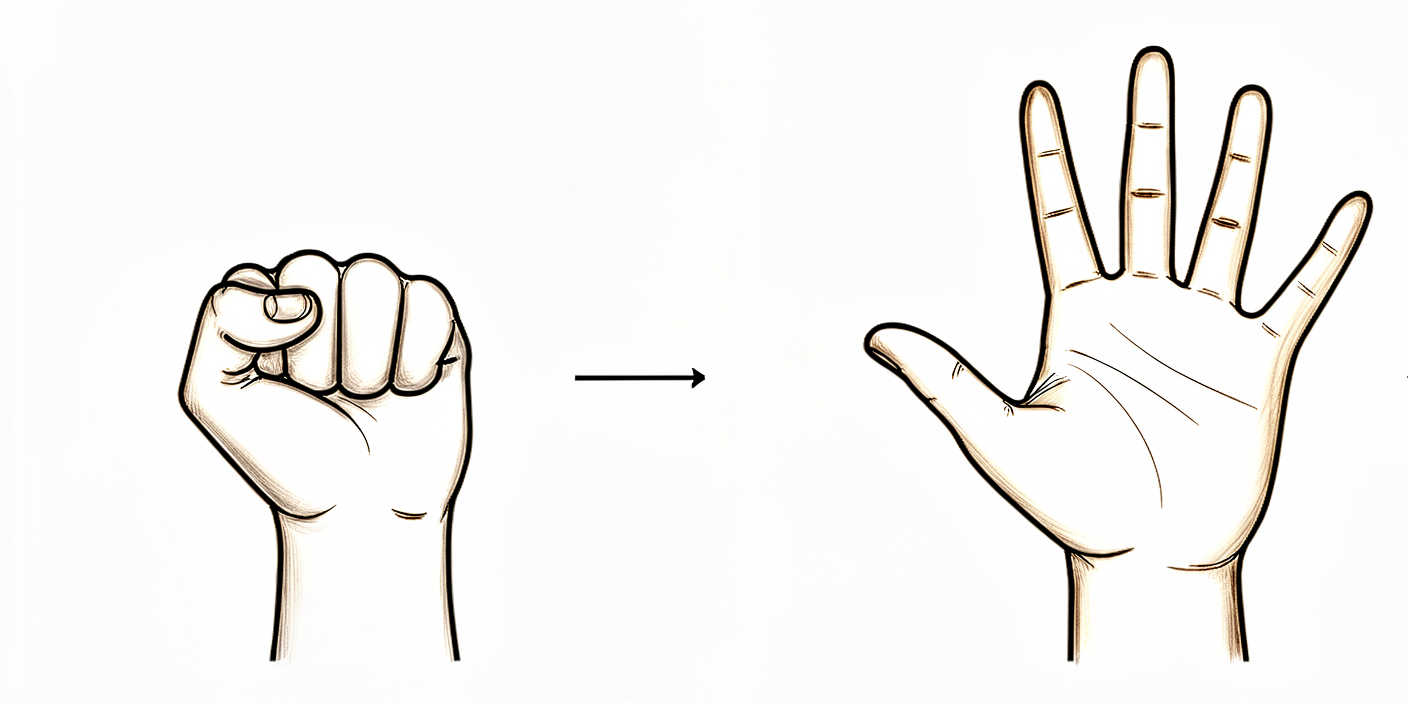
Open and close hand
Keep your hand and fingers moving by opening and closing them, or by squeezing a stress ball.
10 times, 3 times per day

Kieran Hirpara 4.0
Elbow bends
Bend and straighten your elbow.
10 times, 3 times per day
Kieran Hirpara 4.0
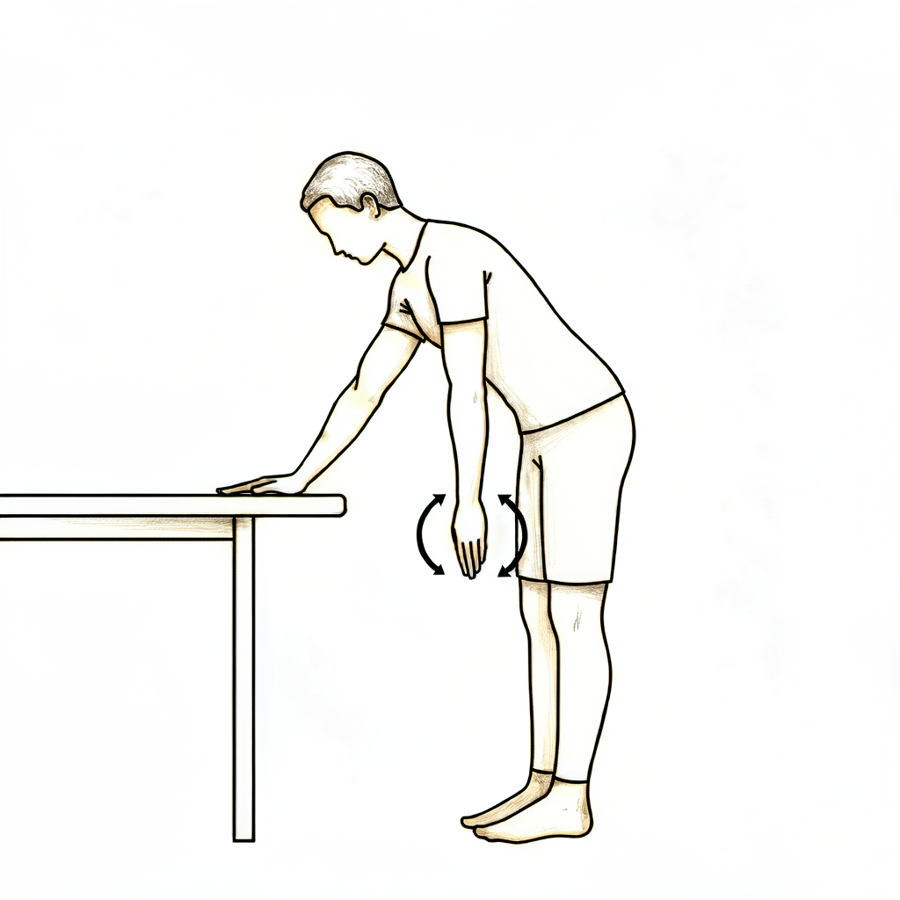
Pendulums
This is a passive exercise. Lean forward and let your arm relax down. Use your body to move the arm gently either clockwise or anti-clockwise, along with forwards, backwards and side to side.
About 30 seconds each way, 3 times per day

Kieran Hirpara 4.0
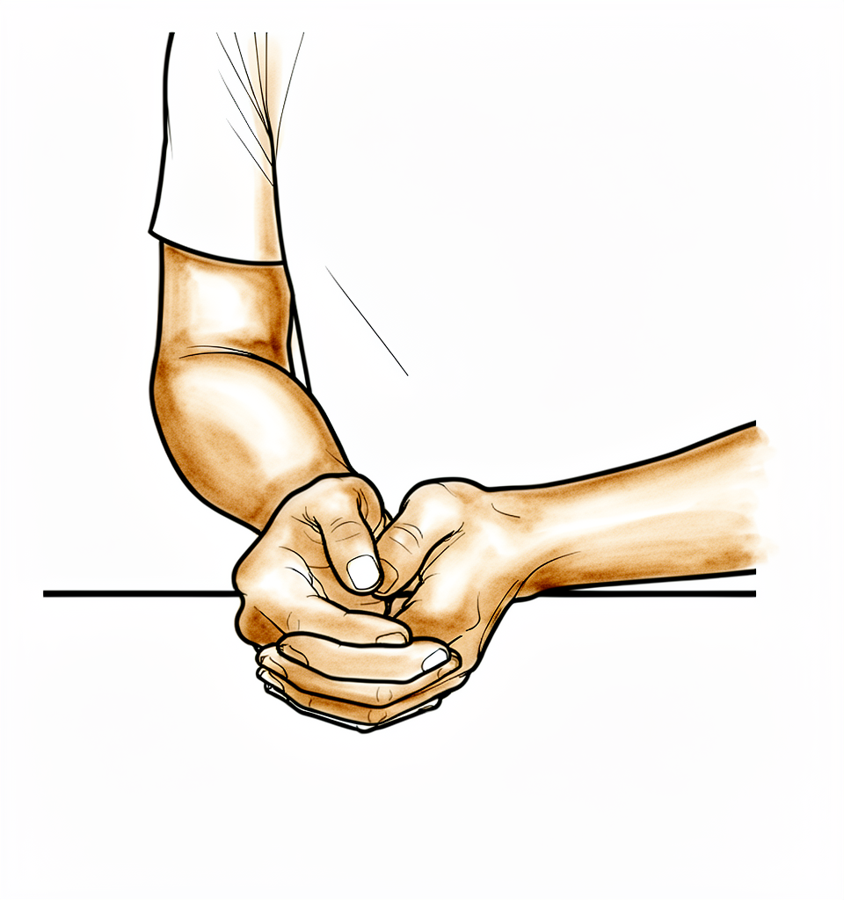
Assisted abduction
Sitting on a chair and leaning forward, cradle the arm again and help it out to the side (like rocking a baby).
10 times, 3 times per day
Kieran Hirpara 4.0
External rotation
Sitting on a chair, only move your arm from where it sits in the sling to pointing straight in front of you. Don't go further outwards.
10 times, 3 times per day
Kieran Hirpara 4.0
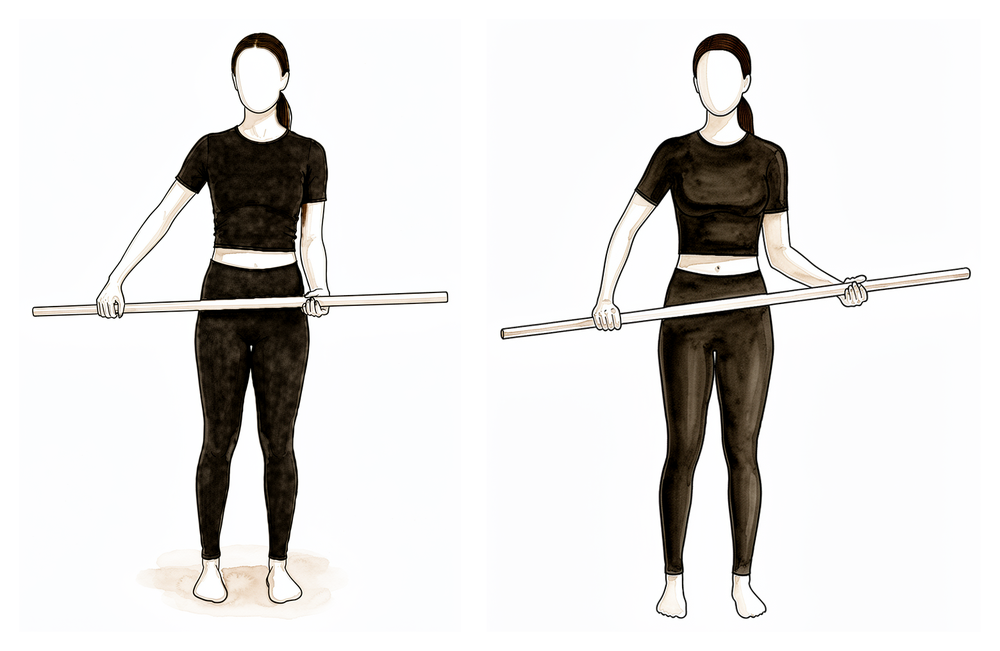
Assisted external rotation with a stick
Lie on your back with your elbow tucked by your side and bent to a right angle. Hold a stick in both hands and use your good arm to turn the operated hand outwards, rotating the shoulder. After this operation there is no limit on how far out you go, so gently push the range a little further as it frees up.
10 times, 3 times per day
Kieran Hirpara 4.0
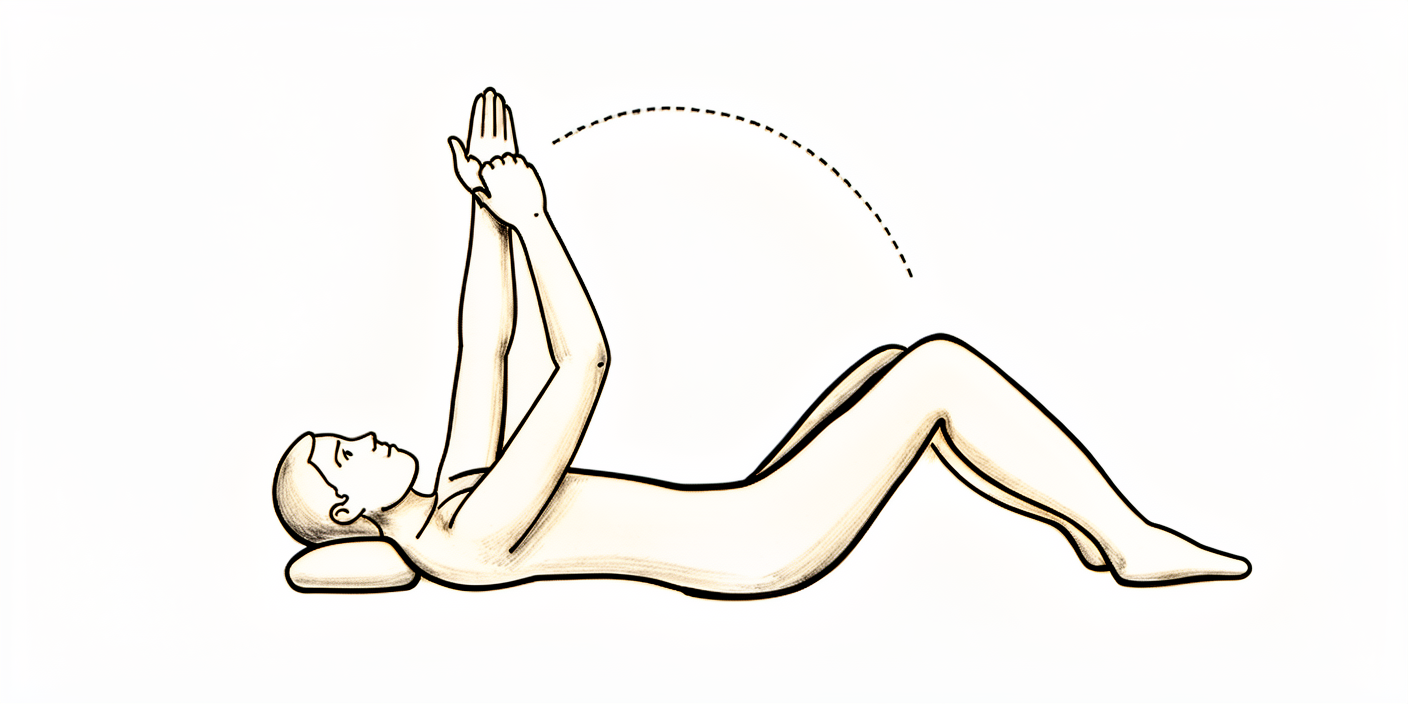
Assisted forward flexion (lying)
If you prefer, lie on your back and hold a stick or a rolled towel in both hands. Use your good arm to push the operated arm up over your head, as far as it will comfortably go, then lower it slowly. Push into a firm stretch each time.
10 times, 3 times per day
Kieran Hirpara 4.0
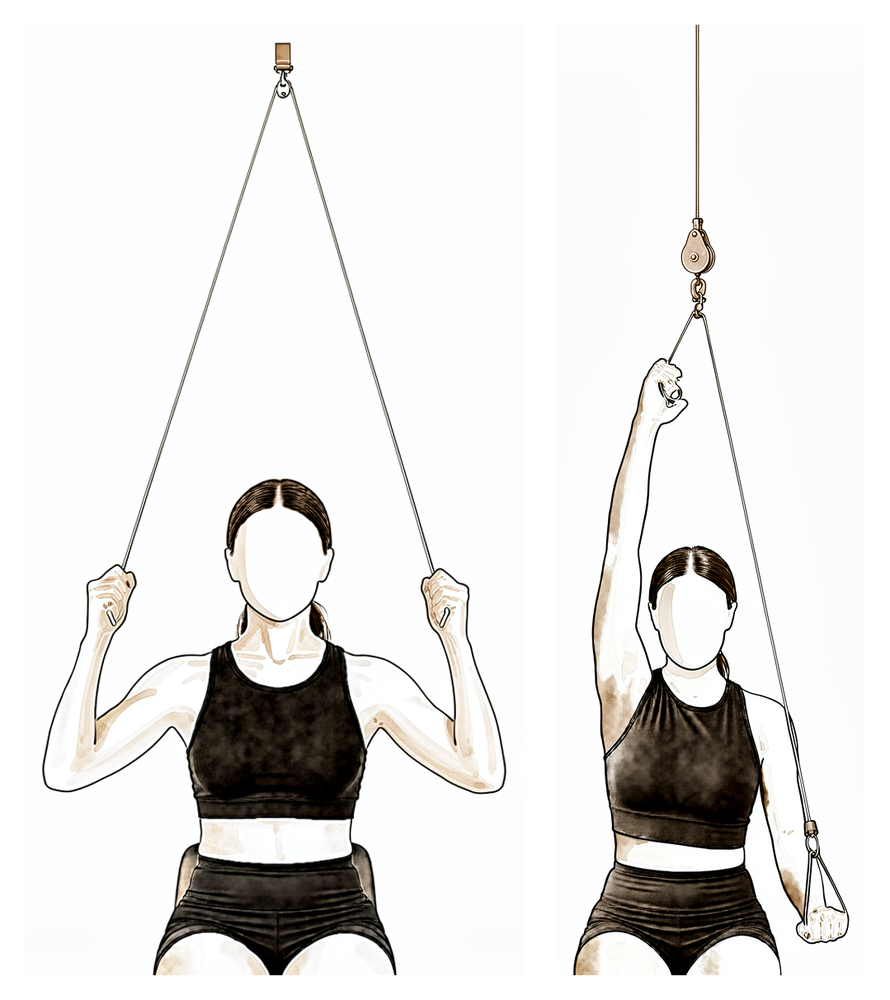
Over-door pulley
Sit under an over-door pulley with a handle in each hand. Pull down with your good arm to raise the operated arm overhead as far as it will go, then lower slowly. Take it to a firm stretch each time, not severe pain.
10 times, 3 times per day
Kieran Hirpara 4.0
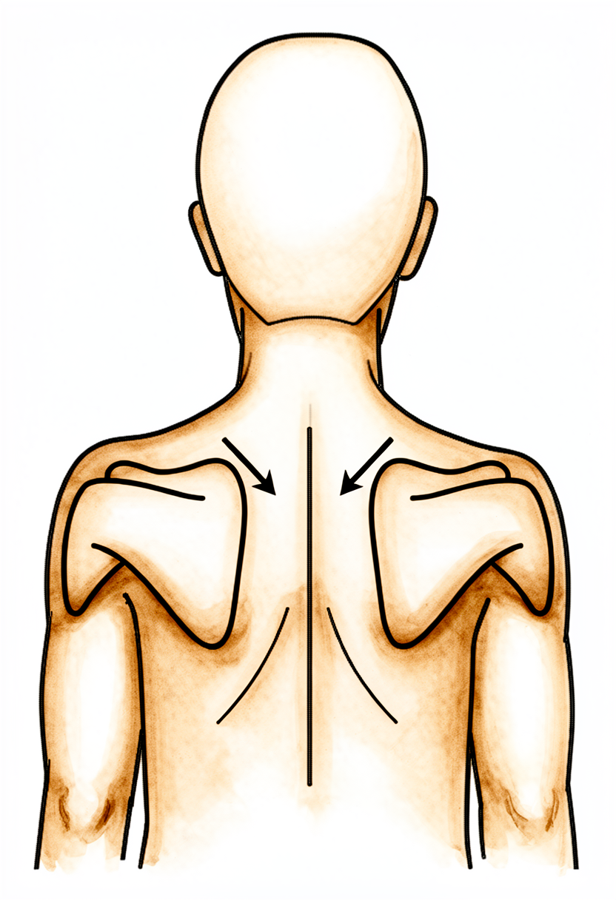
Lower trapezius setting
Squeeze your shoulder blades downwards and together.
Hold 5 seconds, 5 times, 3 times per day
Kieran Hirpara 4.0
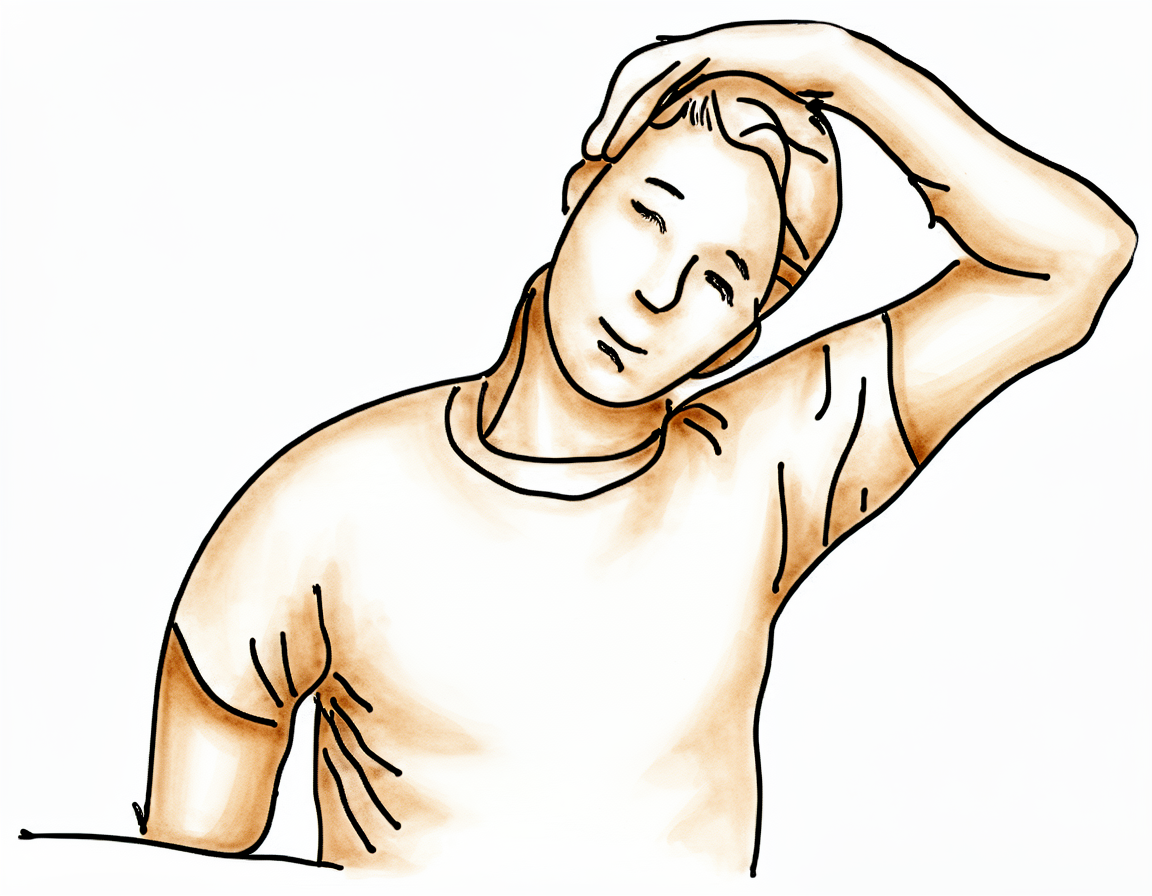
Upper trapezius stretch
Use your non-operated arm to bring your ear towards your shoulder, away from the operated side.
Hold 10 seconds, 3 times, 3 times per day
Kieran Hirpara 4.0
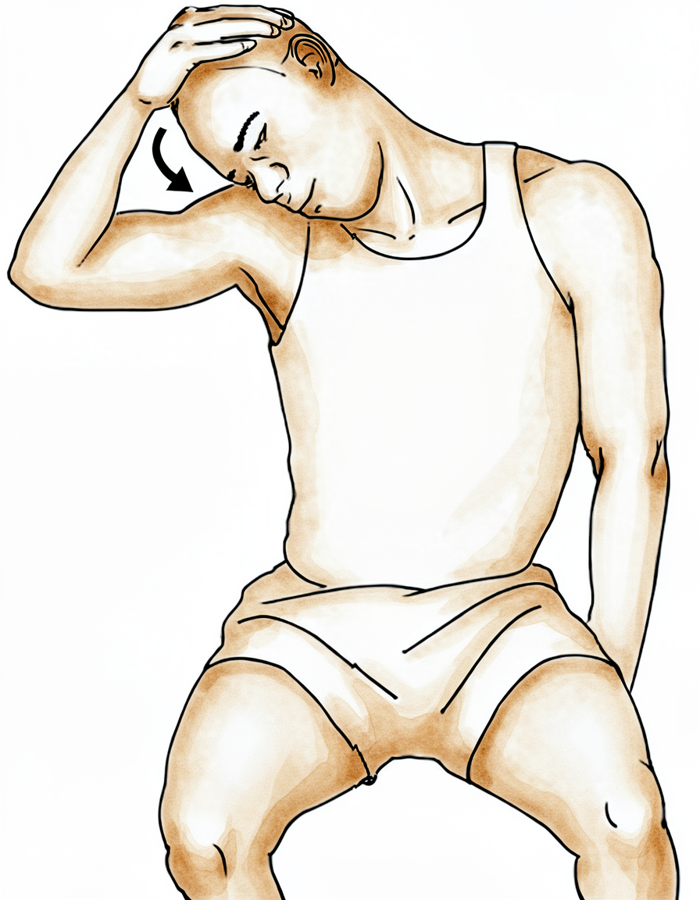
Levator scapulae stretch
Use your non-operated arm to bring your nose towards your armpit area, away from the operated side.
Hold 10 seconds, 3 times, 3 times per day
Kieran Hirpara 4.0
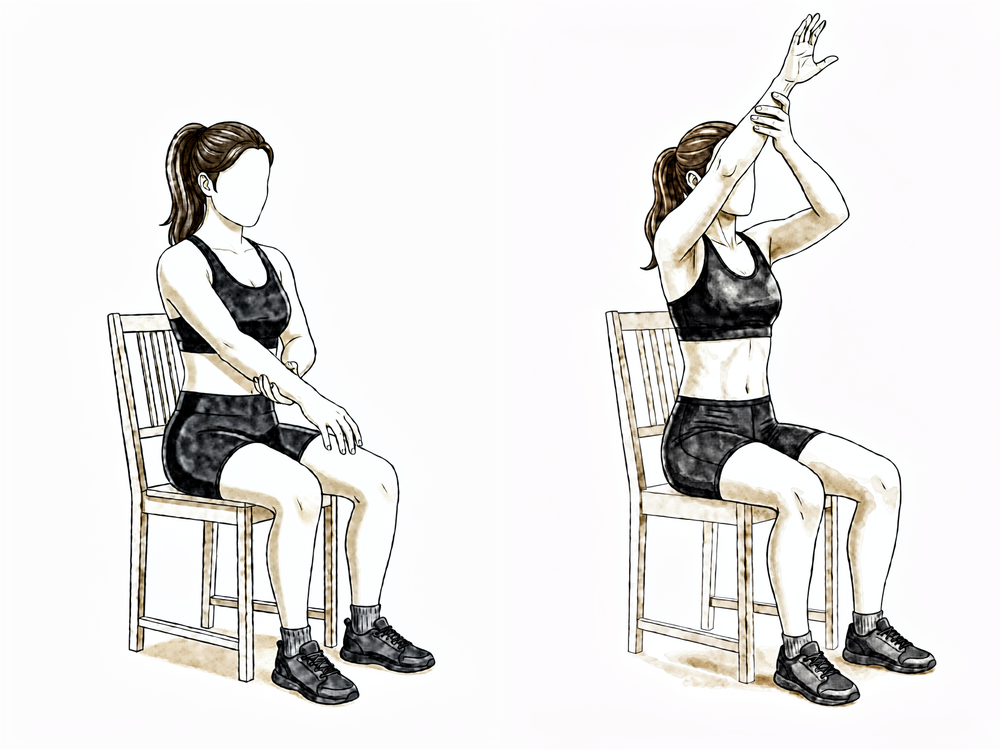
Assisted forward elevation (sitting)
Sitting and leaning forward slightly, support the operated forearm with your good hand and use it to lift the operated arm forwards and up in front of you, as far as is comfortable, then lower it slowly. Let the good arm do the work so the operated shoulder stays relaxed.
As guided by your physiotherapist
Begin these gentle exercises in hospital and continue them at home. They should be comfortable; ease back if pain increases.
Wearing your sling
- The sling is only to be worn for comfort, and should be left off as much as possible. You don't need to sleep in the sling.
- Move and use your arm as much as possible.
- It is advisable to wear the sling when out of the house, to prevent people knocking into your arm.
- Aim for physiotherapy sessions at least twice a week for the first six weeks.
- Use ice for pain relief if needed.
- When wearing your sling, relax your shoulder and let the sling take the weight of your arm.
- Take your painkillers before you do your exercises, and before your physiotherapy appointments.
- Unless you have arranged your own physiotherapy, an appointment has been made for you and is detailed in your discharge pack.
- If you have any problems, contact the rooms or let your physiotherapist know.
When you go home
Once you are home, your recovery continues with the full rehabilitation protocol for your operation: capsular release; subacromial decompression.
These early in-hospital exercises are adapted from published patient guidance and rehabilitation protocols for these procedures, and the week ranges are typical rather than fixed; your physiotherapist guides your recovery individually based on how your shoulder responds. The evidence behind this early phase (why the priority after a capsular release is immediate movement rather than protecting the shoulder) is summarised in the evidence section, available as a PDF from the top of this page.
Evidence & references
Topic scope: the early in-hospital phase of rehabilitation for patients who have just had an arthroscopic capsular release (for a stiff/frozen shoulder) and/or an arthroscopic subacromial decompression (acromioplasty). This page covers only the first day or two after surgery — getting the shoulder moving before the patient goes home. The full recovery course lives in the parent protocols: capsular release and subacromial decompression. Read those for the week-by-week plan, strengthening and return to work/sport.
Defining principle of this pathway (the inversion): unlike most shoulder operations — where a repair (cuff, labrum, instability) must be protected in a sling and range of motion is restricted to let the tissue heal — capsular release does the opposite. Nothing has been repaired, so there is no construct to protect. The shoulder was deliberately freed up in theatre, and the enemy now is re-stiffening. The in-hospital priority is therefore immediate, aggressive range of motion from day 0–1, usually with no protective sling (or a sling only for comfort, discarded quickly), to hold on to the range gained at surgery. A subacromial decompression is also a "make room / take pressure off" operation with no repair, so it follows the same early-movement logic. The single thing that changes this is if the surgeon also had to repair a rotator cuff tear at the same time — then the slower, protected cuff-repair pathway applies and the surgeon will say so.
The early in-hospital phase
The aim of the first day or two is simple: keep the shoulder moving and keep the patient comfortable enough to do so. In hospital, patients are started on gentle hand, wrist and elbow movements, pendulum (Codman) swings, and assisted elevation and external rotation — exactly the gentle exercises listed on the patient page. Adequate pain relief is the practical key, because a comfortable patient will move the arm, and a moving arm does not re-stiffen.
For capsular release in particular, surgeons commonly inject an intra-articular corticosteroid and perform a gentle controlled manipulation at the end of the operation to confirm the gained range and to damp down the post-operative inflammation that drives re-contracture [Smith 2017, PMC5137660]. The early motion exercises then begin straight away — often the same day or the first day after surgery.
Evidence by theme
Immediate-motion capsular-release protocols
Published arthroscopic capsular release (ACR) series describe starting motion immediately, not after a protected period. The largest cohort (Kanbe 2018, n = 255) commenced "passive, assisted-active and stooping (pendulum) exercises for forward flexion and external rotation 1 day after surgery," progressing to active strengthening at ~2 weeks and return to work by 4–6 weeks [Kanbe 2018]. Surgical-technique reviews echo this: active-assisted and passive range-of-motion exercises — pendulum/circumduction and pulley work — "can be started on the first postoperative day," and patients perceive the improvement in motion immediately, which reinforces their commitment to moving the arm [Essential Surgical Technique, PMC6221416]. Several ACR series pair the release with an intra-articular steroid + controlled manipulation at the index procedure to limit re-stiffening [Smith 2017, PMC5137660]. Evidence: large cohorts + expert/consensus.
Subacromial decompression — early motion, sling for comfort only
Arthroscopic subacromial decompression (acromioplasty) likewise has no repair to protect. Patient-guidance protocols start physiotherapy immediately after surgery, with a sling worn only 1–2 weeks for comfort and early active range of motion (forward elevation below shoulder height, gentle rotation) from the outset; strengthening follows at 4–6 weeks and unrestricted activity by 6–12 weeks [Boston Shoulder Institute SAD protocol; London Shoulder Partnership]. The important caveat, stated in every protocol, is that a concomitant rotator cuff repair (or biceps/SLAP repair) converts the recovery to the slower, protected pathway [PMC6145625].
Why immediate motion (and not protection)
A small number of patients develop stiffness after even simple arthroscopic shoulder procedures, which is the failure mode early movement is designed to prevent [Frozen shoulder after simple arthroscopic procedures, 10.1302/0301-620x.97b7.35387]. Conversely, the corpus also flags chondrolysis after shoulder arthroscopy as a rare but serious complication — a reminder that "aggressive" here means aggressive motion, on a comfortable, well-analgesed patient, not aggressive intra-articular intervention [10.1177/0363546503262176].
Phased timeline — early phase only
| Phase | Window | Sling | ROM / use | Notes |
|---|---|---|---|---|
| 0 — In hospital (this page) | Day 0–1 | None, or comfort only — left off as much as possible, not worn to sleep | Gentle hand/wrist/elbow movement; pendulums; assisted forward flexion + external rotation begun day 1; HEP several times/day | Take painkillers before exercises and physio; ice for pain. Capsular release: intra-articular steroid ± gentle manipulation often given in theatre |
| 1 — First weeks (see parent protocol) | Week 0–2+ | Comfort only, discarded early | Continue assisted/active motion to hold the gained range; physio ≥ 2×/week early on | Full week-by-week plan, strengthening and return to function are in the capsular release and subacromial decompression protocols |
Branch point — if a rotator cuff repair was also performed: the recovery converts to the protected rotator-cuff-repair pathway (sling ~6 weeks, restricted motion, delayed strengthening). The surgeon confirms which pathway applies before discharge — this is a surgeon-decided point, not a default.
Key controversies / evidence quality
- The post-operative rehab protocol is consensus/expert, not RCT-derived. There is no high-level trial defining the optimal regimen after capsular release; published protocols are large cohorts and surgeon patient-guidance documents and vary in detail [Kanbe 2018; Willmore 2020 review]. What is consistent across them all is the immediate-motion, no-protective-sling principle.
- Sling: comfort only vs none. Protocols differ on whether to use a comfort sling at all and for how long (days to ~2 weeks for decompression). All agree it must be left off as much as possible and is never a protective device here.
- Steroid + manipulation at the index procedure. Common in ACR to limit re-stiffening, but the exact regimen (dose, whether to manipulate) is surgeon preference, not standardised by trial.
Evidence-strength flags
- MODERATE (large cohorts): clinical outcomes of arthroscopic capsular release with day-1 motion (Kanbe 2018, n = 255); subacromial decompression outcomes.
- WEAK / CONSENSUS: the early-phase rehab protocol itself — immediate motion, sling-for-comfort rules, intra-articular steroid + manipulation timing (surgeon patient-guidance and expert review; no defining rehab RCT).
- Branch-point claim (cuff repair → protected pathway): STRONG rationale and uniformly stated across protocols.
Citations
RAG corpus (180,000+ Orthopaedic articles)
- Arthroscopic capsular release for refractory shoulder stiffness: a critical analysis of effectiveness in specific etiologies. J Shoulder Elbow Surg. DOI: 10.1016/j.jse.2009.08.004
- Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am. 1997. DOI: 10.2106/00004623-199708000-00006
- Arthroscopic release for chronic, refractory adhesive capsulitis of the shoulder. J Bone Joint Surg Am. 1996. DOI: 10.2106/00004623-199612000-00003
- Clinical outcome of arthroscopic capsular release for frozen shoulder: essential technical points in 255 patients (Kanbe 2018; day-1 ROM, 4–6 wk return to work). J Orthop Surg Res. 2018. DOI: 10.1186/s13018-018-0758-5
- Establishing the MCID and PASS thresholds following arthroscopic capsular release for idiopathic adhesive capsulitis. Arthroscopy. 2023. DOI: 10.1016/j.arthro.2023.08.083
- Frozen shoulder after simple arthroscopic shoulder procedures. Bone Joint J. 2015. DOI: 10.1302/0301-620x.97b7.35387
- Glenohumeral chondrolysis after shoulder arthroscopy (rare serious complication; "aggressive" = motion, not intra-articular intervention). Am J Sports Med. 2004. DOI: 10.1177/0363546503262176
- Effect of capsular release in the treatment of shoulder stiffness concomitant with rotator cuff repair. Am J Sports Med. 2014. DOI: 10.1177/0363546513519326
Literature & published protocols (URLs)
- Kanbe K. Clinical outcome of arthroscopic capsular release for frozen shoulder (day-1 ROM protocol). PMC: https://pmc.ncbi.nlm.nih.gov/articles/PMC5857121/
- Smith CD et al. Arthroscopic capsular release for idiopathic frozen shoulder with intra-articular injection and controlled manipulation. PMC5137660: https://pmc.ncbi.nlm.nih.gov/articles/PMC5137660/
- Essential surgical technique for arthroscopic capsular release (active-assisted/passive ROM from first post-op day). PMC6221416: https://pmc.ncbi.nlm.nih.gov/articles/PMC6221416/
- Arthroscopic subacromial decompression and acromioplasty — rehabilitation and concomitant-repair caveat. PMC6145625: https://pmc.ncbi.nlm.nih.gov/articles/PMC6145625/
- Boston Shoulder Institute — Post-operative arthroscopic subacromial decompression protocol (sling 1–2 wk for comfort, immediate physio): https://bostonshoulderinstitute.com/wp-content/uploads/2014/07/Shoulder-Subacromial-Decompression-protocol2.pdf
- The London Shoulder Partnership — Subacromial decompression (acromioplasty): http://thelondonshoulderpartnership.co.uk/shoulder/shoulder-surgery/subacromial-decompression-acromioplasty/
- J Paget NHS — Patient information: arthroscopic capsular release following a frozen shoulder (sling for comfort, early movement): https://www.jpaget.nhs.uk/media/efmf3bab/arthroscopic-capsular-release-following-a-frozen-shoulder.pdf





